右美托咪定對老年人髖部手術后認知功能障礙的影響
2015-08-24 08:56:56張云飛高偉忠馬世穎劉金碧
天津醫藥 2015年6期
張云飛,高偉忠,馬世穎,劉金碧
藥物臨床觀察
右美托咪定對老年人髖部手術后認知功能障礙的影響
張云飛,高偉忠,馬世穎,劉金碧
目的 觀察硬膜外麻醉復合不同劑量右美托咪定對老年人髖部手術后循環和認知功能障礙(POCD)的影響。方法 選擇2013年6月—2014年9月,65歲以上髖部手術患者120例,行硬膜外麻醉聯合右美托咪定靜脈泵注,按右美托咪定的泵注量不同,分為A組0.2 μg·h-1·kg-1,B組0.4 μg·h-1·kg-1和C組0.6 μg·h-1·kg-1,每組40例。觀察并記錄3組患者入室時(T0)、用藥后10 min(T1)、用藥后20 min(T2)、停藥即刻(T3)、停藥后10 min(T4)以及手術完畢時(T5)的心率(HR)、平均動脈壓(MAP)、血氧飽和度(SpO2)。應用簡易智力狀態量表(MMSE)測試3組患者術前24 h(t1)、術后12 h(t2)、術后24 h(t3)及術后72 h(t4)認知功能。結果 3組患者在T0時MAP、HR及SpO2比較差異無統計學意義;C組T2、T3時HR和MAP均較A組、B組明顯下降(均P<0.05)。3組術前MMSE評分差異無統計學意義,B組t2、t3時的MMSE評分均明顯高于A組和C組(P<0.05);B組POCD發生率明顯低于A組和C組(P<0.05)。結論 硬膜外麻醉復合右美托咪定以0.4 μg·h-1·kg-1靜脈泵注對老年患者的循環干擾小,可減少老年患者圍手術期認知功能障礙的發生。
麻醉,硬膜外;認知障礙;手術后期間;老年人;右美托咪定
老年患者術后認知功能障礙(POCD)十分常見,嚴重影響生活質量。研究發現右美托咪定(dexmedetomidine,DEX)具有中樞抗交感作用,能維持心血管功能穩定,抑制應激反應和炎癥反應等,降低老年患者POCD的發病率,但對右美托咪定的適宜劑量缺乏大規模的臨床研究[1],且右美托咪定專家指南(2013版)規定的右美托咪定使用劑量范圍較大[2],臨床工作中發現不同劑量右美托咪定所產生的效果差別較大,本研究通過觀察硬膜外麻醉復合不同劑量右美托咪定對老年人髖部手術POCD的影響,為臨床使用提供參考。
1 資料與方法
1.1 一般資料 選擇2013年6月—2014年9月本院硬膜外麻醉行髖部手術老年患者120例。ASA分級Ⅰ~Ⅱ級,年齡≥65歲。排除標準:青光眼、癡呆或精神分裂癥;有嚴重高血壓病史、缺血性心臟病史、心臟傳導阻滯病史;服用抗抑郁藥物或β受體阻滯藥物者;拒絕參加本研究者。采用隨機數字表法隨機均分為3組,A組、B組和C組的劑量分別為0.2、0.4、0.6 μg·h-1·kg-1,靜脈泵注。其中股骨頭壞死38例,粗隆間骨折31例,股骨頸骨折46例,髖臼骨折5例。所有患者麻醉均由同一工作組完成。本研究經醫院倫理委員會批準,所有入選患者均被告知研究內容,并簽署知情同意書。
1.2 麻醉方法 所有患者麻醉前常規監測血壓(BP)、脈搏、呼吸及脈搏血氧飽和度,開放靜脈通路,滴注乳酸林格注射液,予鹽酸右美托咪定靜脈持續泵注。側臥位選擇L2~3間隙行硬膜外穿刺,頭側置管3 cm,予2%利多卡因試驗量3 mL,待麻醉平面出現,排除蛛網膜下腔麻醉后,予0.894%羅哌卡因6 mL硬膜外腔注入,留置硬膜外導管備術中追加局麻藥物和術后硬膜外自控鎮痛(PCEA),術中控制麻醉平面在T10以下,所有患者面罩吸氧(流量2 L/min),在清點器械準備縫合創面時停泵注鹽酸右美托咪定。若患者術中BP降低超過基礎值的20%,給予麻黃堿10 mg靜脈注射;若心率(HR)<55次/min,給予阿托品0.5 mg靜脈注射。
1.3 監測指標 (1)一般資料。性別、年齡、體質量、ASA分級、術中失血量,手術時間、麻醉時間。(2)不同時點循環指標及血氧飽和度(SpO2)指標。患者入室時(T0)、用藥后10 min (T1)、用藥后20 min(T2)、停藥即刻(T3)、停藥后10 min(T4)以及手術完畢時(T5)的HR、平均動脈壓(MAP)、SpO2。(3)認知功能評定。應用簡易智力狀態檢查(MMSE)[3]測試方法分別評定3組患者術前24 h(t1)、術后12 h(t2)、術后24 h(t3)及術后72 h(t4)的認知功能。總分為30分,≤23分為認知功能缺陷,下降2分以上為認知功能下降。所有患者術后予48 h PCEA,配方為甲磺酸羅哌卡因注射液400 mg加生理鹽水至200 mL,速度為4 mL/h,追加量(自控鎮痛劑量)為:2 mL,鎖定時間15 min,維持VAS評分≤4分。
1.4 統計學方法 采用SPSS 18.0統計軟件進行分析。計量數據以±s表示,組間比較采用單因素方差分析,組間多重比較用SNK法,計數資料用例或例(%)表示,組間比較采用卡方檢驗,P<0.05為差異有統計學意義。
2 結果
2.1 一般資料及術中情況比較 3組患者一般資料各指標以及手術時間、麻醉時間、失血量比較差異均無統計學意義,見表1。
Tab.1 Comparison of the parameters of general data and intraoperative situation in patients among three groups表1 3組患者一般資料及術中情況各指標的比較(n=40,±s)
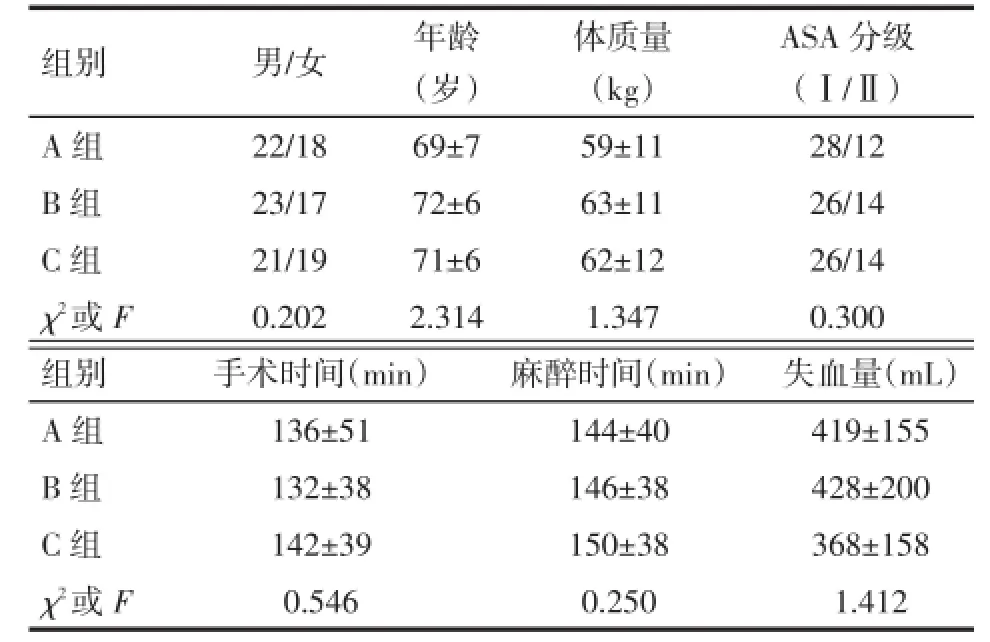
Tab.1 Comparison of the parameters of general data and intraoperative situation in patients among three groups表1 3組患者一般資料及術中情況各指標的比較(n=40,±s)
均P>0.05
組別 男/女 年齡 體質量ASA分級(歲) (kg) (Ⅰ/Ⅱ)A組22/1869±759±1128/12 B組23/1772±663±1126/14 C組21/1971±662±1226/14 χ2或F0.2022.3141.3470.300組別 手術時間(min) 麻醉時間(min)失血量(mL)A組136±51144±40419±155 B組132±38146±38428±200 C組142±39150±38368±158 χ2或F0.5460.2501.412
2.2 不同時點循環指標及SpO2比較 3組患者在T0時HR、MAP比較差異均無統計學意義,T1時HR 和MAP均較基礎值降低。與A組、B組相比,C組患者T2、T3時HR及MAP明顯下降,差異有統計學意義(P<0.05)。3組患者SpO2差異無統計學意義,見表2。
2.3 3組患者術中血管活性藥物用量比較 C組術中麻黃堿及阿托品用量比例高于A組和B組(P<0.05),見表3。
2.4 3組患者POCD發生率及不同時點MMSE評分比較 B組術后POCD發生率低于A組、C組(P<0.05)。3組患者術前(t1)MMSE評分差異無統計學意義。B組患者t2、t3的MMSE評分均明顯高于A組和C組(P<0.05),見表4。
3 討論
POCD是指術前無精神異常的患者麻醉手術后,出現暫時性可逆的記憶力和定向力等認知功能障礙,同時伴有人格和社交能力的改變,少數患者發展為永久性損害。POCD的發生與創傷應激、炎癥反應及中樞膽堿能系統功能降低等因素有關[4]。同時,年齡是發生POCD的高危因素,老年人大腦神經元數量減少,與認知功能相關的受體,尤其是膽堿能受體的減少及對麻醉藥的敏感性增加都是發生POCD的重要原因。循證醫學和動物實驗表明,神經元形態和生物學重構是通過激活炎性因子介導的炎癥反應造成中樞神經系統炎性反應,在大腦最易受到影響的老年期,引起認知功能受損[5-7]。動物實驗也證實,在手術或外周炎性刺激時,老年大鼠較成年大鼠更容易發生POCD[8]。MMSE量表具有簡便易行、不受情緒影響,敏感性和特異性均較高等特點,故國內外普遍采用MMSE評分法評判患者是否發生POCD[9]。
Tab.2 Comparison of parameters of circulation indicator and oxyhemoglobin saturation in different time points among three groups表2 3組不同時點循環指標及SpO2比較 (n=40,±s)
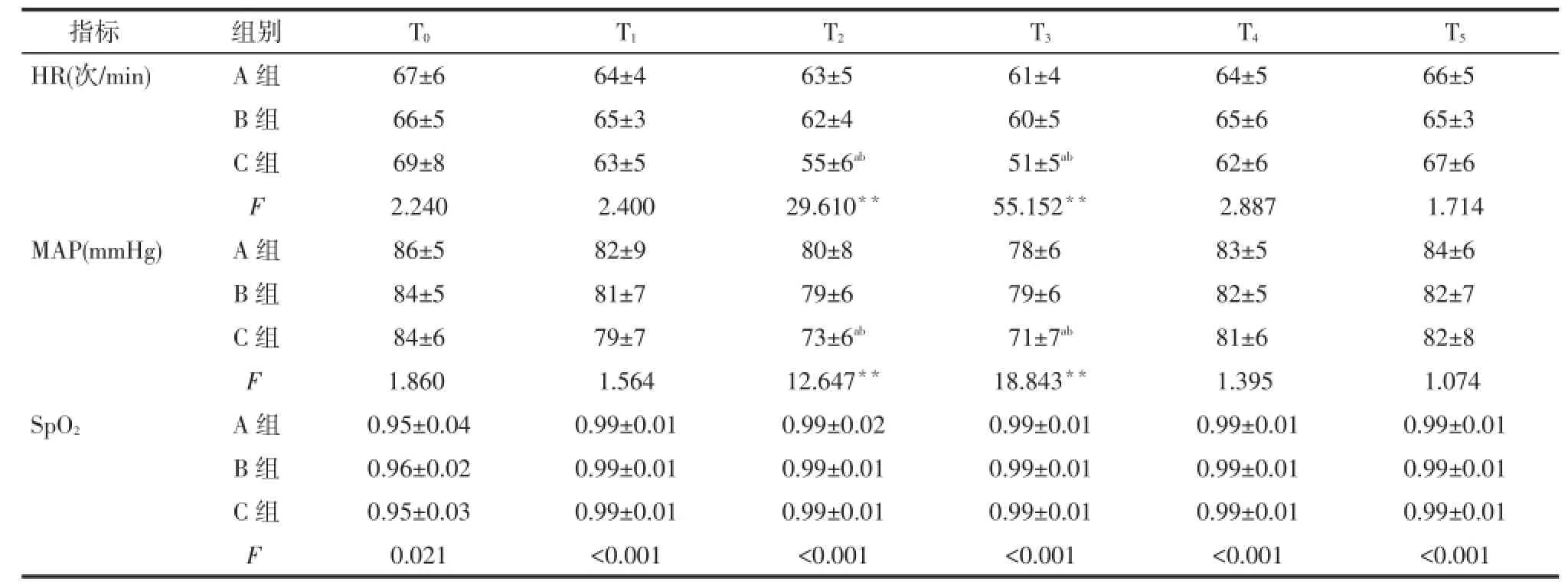
Tab.2 Comparison of parameters of circulation indicator and oxyhemoglobin saturation in different time points among three groups表2 3組不同時點循環指標及SpO2比較 (n=40,±s)
*P<0.05,**P<0.01;a與A組比較,b與B組比較,P<0.05;表3、4同;1 mmHg=0.133 kPa
指標組別T0T1T2T3T4T5HR(次/min)A組67±664±463±561±464±566±5 B組66±565±362±460±565±665±3 C組69±863±555±6ab51±5ab62±667±6 F 2.2402.40029.610**55.152**2.8871.714 MAP(mmHg)A組86±582±980±878±683±584±6 B組84±581±779±679±682±582±7 C組84±679±773±6ab71±7ab81±682±8 F 1.8601.56412.647**18.843**1.3951.074 SpO2A組0.95±0.040.99±0.010.99±0.020.99±0.010.99±0.010.99±0.01 B組0.96±0.020.99±0.010.99±0.010.99±0.010.99±0.010.99±0.01 C組0.95±0.030.99±0.010.99±0.010.99±0.010.99±0.010.99±0.01 F 0.021<0.001<0.001<0.001<0.001<0.001

Tab.3 Comparison of different dosage in patients during perioperative period表3 3組患者圍術期輔助用藥量比較[n=40,例(%)]
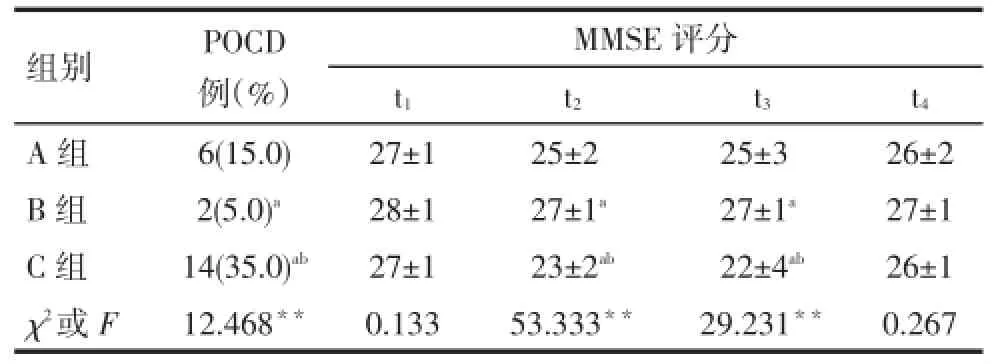
Tab.4 Comparison of the incidence of POCD and MMSE score in patients among different groups表4 3組患者POCD發生率及MMSE評分比較(n=40)
右美托咪定屬咪唑類衍生物,是一種新型高選擇性α2受體激動劑,具有良好的鎮靜、鎮痛及可喚醒的特點,又由于呼吸抑制輕和血流動力學穩定等特點,而廣泛應用于臨床麻醉中[2]。已有研究表明其可以通過減少炎癥因子如白細胞介素(IL)-1β和IL-6等的表達,來減輕炎癥反應,減少POCD的發生[10]。
髖部手術刺激強,應激使免疫系統產生大量炎性介質,通過炎性反應產生大量炎性因子,進而干擾神經活動,引起中樞神經系統退行性變,造成認知功能障礙。本臨床觀察中B組POCD發生率較A組、C組低(P<0.05),可能與A組右美托咪定劑量較低,不足以干預炎性因子的產生有關。老年患者心肺儲備功能減低,血管順應性差,對循環的調節能力有限,C組使用較大劑量右美托咪定使循環抑制造成血壓波動,導致腦組織供血不足,造成缺血缺氧腦損傷,同時C組中使用抗膽堿藥阿托品的量較A組和B組多(P<0.05),抗膽堿藥可明顯增加POCD的發生[11]。
綜上所述,硬膜外麻醉復合0.4 μg·h-1·kg-1右美托咪定在老年人髖部手術中血流動力學平穩,術后POCD發生率低,值得臨床推廣。
[1]Wan L,Jin LM,Cui CL,et al.The current studies on the effects of dexmedetomidine on postoperative cognitive dysfunction in the elerly[J].Chinese Journal of Gerontology,2013,12(33):6339-6345.[萬利,金立民,崔常雷,等.右美托咪定在老年人術后認知障礙應用的研究進展[J].中國老年病學雜志,2013,12(33):6339-6345].doi:10.3969/j.issn.1005-9202.2013.24.138.
[2]Chinase Society of Anesthesiology.The guidelines of dexmedetomidine in clinical practice(2013)[J].Chinese Journal of Anesthesiolo-gy,2013,10(33):1165-1169.[中華醫學會麻醉學分會.右美托咪定臨床應用指導意見(2013)[J].中華麻醉學雜志,2013,10(33): 1165-1169].
[3]Ji MH,Shen JC,Gao R,et al.Early postoperative cognitive dysfunction is associated with higher cortisol levels in aged patients following hip fracture surgery[J].J Anesth,2013,116(5):533-540.doi:10.1007/s00540-013-1633-5.
[4]van Harten AE,Scheeren TW,Absalom AR.A review of postoperative cognitive dysfunction and neuroinflammation associated with cardiac surgery and anaesthesia[J].Anaesthesia,2012,67(3):280-293.doi:10.1111/j.1365-2044.2011.07008.x.
[5]Vaeas S,Degos V,Tracey KJ,et al.High-mobility group box 1 protein initiates postoperative cognitive decline by engaging bone marrowderived macrophages[J].Anesthesiology,2014,120(5):1160-1167.
[6]Li AM,Shi YS,Gao RP,et al.The neuroprotective effect of dexmedetomidine during periopererative period in patients with meningioma[J].Journal of Clinical Anesthesiology,2013,29(7):665-673.[李愛梅,石翊颯,高瑞萍,等.不同劑量DEX托咪定對腦膜瘤切除術患者術后認知功能的影響[J].臨床麻醉學雜志,2013,29(7):665-673].
[7]Yu T,Qiu HB.Dexmedetomidine in the prevention and treatment of delirium in critically ill patients[J].International Journal of Anesthesiology and Resuscitation,2011,32(3):341-343.[于濤,邱海波.右美托咪啶在重癥患者譫妄的預防和治療作用研究進展[J].國際麻醉學與復蘇雜志,2011,32(3):341-343].doi:10.3760/cma.j.issn.1673-4378.2011.06.022.
[8]Sezer A,Memis D,Usta U,et al.The effect of dexmedetomidine on liver histopathology in a rat sepsis model:an experimental pilot study [J].Ulus Travma Acil Cerrahi Derg,2010,16(2):108.
[9]Wu XM,Xu X,Wang JK,et al.Efficacy and safety of intravenous dexmedetomidine as an adjunct to general anesthesia[J].Chinese Journal of Anesthesiology,2007,27(9):773-776.[吳新民,許幸,王俊科,等.靜脈注射右美托咪啶輔助全身麻醉的有效性和安全性[J].中華麻醉學雜志,2007,27(9):773-776].
[10]Hudetz JA,Gandhi SD,Iqbal Z,et al.Elevated postoperative inflammatorybiomarkers are associated with short-and medium-term cognitive dysfunclion after coronary artery surgery[J].Anesthesiology,2011,25(1):116.doi:10.1007/s00540-010-1042-y.
[11]Gerlach AT,Dasta JF,Steinberg S,et al.A new dosing protocol reduces dexmedetomidine-associated hypotension incritically ill surgical patients[J].JCritCare,2009,24(4):568-574.doi:10.1016/j.jcrc.2009.05.015.
(2014-10-03收稿 2015-02-02修回)
(本文編輯 李國琪)
Dexmedetomidine on cognitive function of elderly patients who underwent hip orthopedic surgery
ZHANG Yunfei,GAO Weizhong,MA Shiying,LIU Jinbi
Department of Anesthesiology,the First People’s Hospital of Zunyi,Guizhou 563000,China
Objective To observe the effect of a variety dosage of dexmedetomidine on circulatory and cognitive functions in elderly patients who underwent hip orthopedic surgery.Methods A total of 120 patients who underwent hip orthopedic surgery,with age over 65 years old were recruited from 06/2013 to 09/2014 and were administered intravenously dexmedetomidine after epidural anesthesia.Based on the dosage of dexmedetomidine,patients were randomly divided into 3 groups with 40 cases in each group:Group A were given 0.2 μg·h-1·kg-1dexmedetomidine;Group B were given dexmedetomidine 0.4 μg·h-1·kg-1,and group C were given 0.6 μg·h-1·kg-1.The heart rate(HR),mean arterial pressure(MAP),and pulse oxygen saturation(SpO2)were recorded at 6 time points,including the time entering operating room(T0),10 min(T1),20 min(T2)after drug administration,the time of drug withdrawal(T3),10 min after drug withdrawal(T4)and the terminal time of surgery(T5)respectively.Cognitive function was evaluated by mini-mental state examination(MMSE)at the time points of 24 hours before surgery(t1),12 hours(t2),24 hours(t3),and 72 hours(t4)after surgery.Results All 3 groups of patients show no significant differenceof MAP,HR and SpO2at T0(P>0.05).A significant decrease in MAP and HR were observed in Group C at T2and T3time points compared to those in Group A or Group B(P<0.05).There was no significant difference in MMSE at time point T1among all three groups(P>0.05).However,compared to that in group A or group C,MMSE increased significantly at time point T2,T3in group B(P<0.05).In addition,compared to group A or group C,the patients in group B exhibited lower incidence of postoperative cognitive function disorder(P<0.05).Conclusion Continuous intravenous infusion of Dexmedetomidine can be used in elderly patient who underwent hip orthopedic surgery at the dose of 0.4 μg·h-1·kg-1safely with little interference to circulatory and cognitive function in perioperative period.
anesthesia,epidural;cognition disorder;postoperative period;aged;Dexmedetomidine
R614
A DOI:10.11958/j.issn.0253-9896.2015.06.023
基金名稱:遵義市科學技術局聯合科技研發資金項目[遵市科合社字(2014)14號]
遵義市第一人民醫院麻醉科(郵編563000)
張云飛(1973),男,學士學位,副主任醫師,主要從事困難氣道方面研究
猜你喜歡
課堂內外·初中版(科學少年)(2023年10期)2023-12-10 00:43:06
全科護理(2022年10期)2022-12-26 21:19:15
中國合理用藥探索(2022年1期)2022-11-26 00:22:32
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
鄉村科技(2021年33期)2021-03-16 02:26:54
國際放射醫學核醫學雜志(2021年10期)2021-02-28 08:41:58
河北畫報(2020年10期)2020-11-26 07:20:50
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
西南軍醫(2014年5期)2014-04-25 07:42:48
中國合理用藥探索(2014年11期)2014-03-11 20:30:20
