高血壓患者夜間血壓變化與顱內動脈粥樣硬化狹窄的相關性
2016-06-03 01:40:07廖光昊黎紅華
中國實用神經疾病雜志 2016年8期
關鍵詞:高血壓
崔 敏 濮 捷 廖光昊 吳 樂 吳 倩 武 強 黎紅華
廣州軍區武漢總醫院神經內科 武漢 430070
?
高血壓患者夜間血壓變化與顱內動脈粥樣硬化狹窄的相關性
崔敏濮捷廖光昊吳樂吳倩武強黎紅華
廣州軍區武漢總醫院神經內科武漢430070
【摘要】目的探討高血壓患者夜間血壓變化與顱內動脈粥樣硬化狹窄(ICAS)的相關性。方法對高血壓患者進行動態血壓監測和腦血管磁共振血管成像(MRA)檢查。顱內大動脈內徑狹窄程度≥50%定義為ICAS,ICAS病灶數≥2定義為多發性ICAS。根據日間與夜間平均血壓水平,將晝夜血壓變化分為杓型、非杓型、反杓型。結果共359例高血壓患者進入本研究:ICAS患者135例,單發性ICAS 86例,多發性ICAS 49例;226例(63.0%)日間平均血壓升高,322例(89.7%)夜間平均血壓升高;杓型37例(10.3%),非杓型166例(46.2%),反杓型156例(43.5%)。多因素Logistic回歸分析提示:日間平均血壓升高、夜間平均血壓升高、夜間血壓非杓型改變、夜間血壓反杓型改變均與ICAS無顯著相關性(P>0.05);夜間血壓反杓型改變與多發性ICAS密切相關(P<0.05)。結論夜間血壓反杓型改變可能是多發性ICAS的獨立危險因素。
【關鍵詞】高血壓;動態血壓監測;磁共振血管成像;夜間血壓;顱內動脈粥樣硬化狹窄
顱內動脈粥樣硬化狹窄(intracranial atherosclerotic stenosis,ICAS)在亞洲人群中顯著高發,藥物預防的效果欠佳。目前,顱內血管介入治療ICAS尚未在臨床廣泛開展,因此,探討ICAS的危險因素、提高預防效果具有重要臨床意義。高血壓已被證實是ICAS發生、發展的重要危險因素,但既往研究多采用診室血壓這一診斷標準。近期臨床研究提示,動態血壓較診室血壓能夠更可靠地預測心血管事件的發生,尤其是夜間平均收縮壓水平升高是風險最高的預測因子[1]。研究[2]證實,夜間平均血壓升高與頸動脈粥樣硬化密切相關。目前,夜間血壓變化與ICAS發生的關系尚不清楚。本研究應用動態血壓監測(ambulatory blood pressure monitoring,ABPM)檢查,探討高血壓患者夜間血壓變化與ICAS發生的相關性。
1對象與方法
1.1研究對象回顧在我院神經內科住院、并完成了動態血壓監測和腦血管磁共振血管成像(MRA)檢查的高血壓患者的臨床資料。入選標準:(1)高血壓患者;(2)年齡≥40歲;(3)完成了ABPM和MRA檢查的患者。排除標準:(1)年齡<40歲;(2)非高血壓患者;(3)非動脈粥樣硬化性顱內動脈狹窄(動脈夾層、動脈炎、放療后、煙霧病、顱內占位病變等);(4)病情危重、顱內高壓、昏迷、并發嚴重心肺肝腎功能障礙的患者;(5)未完成ABPM和MRA檢查的患者。
1.2顱內動脈檢查方法應用1.5T MRI檢查顱內大動脈。ICAS定義為大腦中動脈、大腦前動脈、大腦后動脈、頸內動脈顱內段、基底動脈、椎動脈顱內段主干血管內徑狹窄程度≥50%[3]。將ICAS病灶數≥2定義為多發性ICAS。采用WASID方法測量顱內動脈狹窄率[4]。
1.3動態血壓監測方法應用無創袖帶式動態血壓監測儀觀察患者的24 h血壓。24 h平均血壓≥130/80 mmHg、日間平均血壓≥135/85 mmHg、夜間平均血壓≥120/70 mmHg定義為血壓升高。根據日間與夜間平均血壓水平,將夜間血壓變化分為以下幾種類型:(1)杓型:夜間平均血壓水平低于日間平均血壓≥10%;(2)非杓型:夜間平均血壓水平低于日間平均血壓<10%;(3)反杓型:夜間平均血壓水平高于日間平均血壓[5]。將發生ICAS的患者分入ICAS組,未發生ICAS的患者分入對照組。

2結果
2.12組臨床資料比較2012-10—2014-07共359例高血壓病患者進入本研究。男236例,平均年齡(62.1±12.1)歲;女123例,平均年齡(64.8±11.6)歲。ICAS患者135例,單發病灶86例,多發病灶49例(見圖1)。ICAS組患者的年齡高于對照組,且糖尿病和血脂異常的發病率高于對照組(P<0.05)。2組性別、冠心病、吸煙方面無顯著差異(P>0.05)。見圖1。
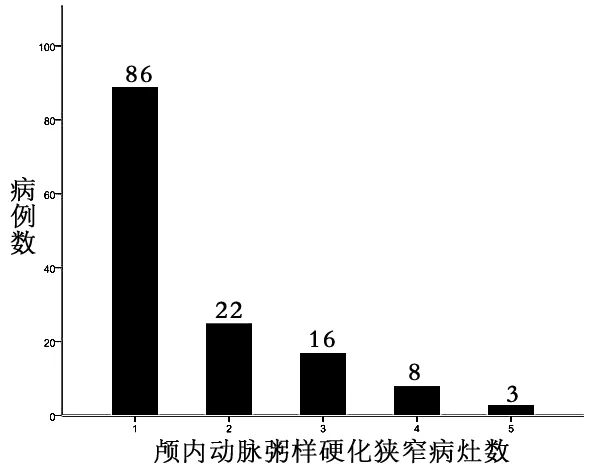
圖1 顱內動脈粥樣硬化狹窄病灶分布情況
2.22組晝夜血壓變化情況比較ICAS組患者的全天平均收縮壓、日間平均收縮壓、夜間平均收縮壓均顯著高于對照組,組間平均舒張壓無顯著差異。2組日間平均血壓升高、夜間平均血壓升高、夜間血壓杓型改變、夜間血壓非杓型改變、夜間血壓反杓型改變的發生率無顯著差異(P>0.05)。見表1。

表1 2組晝夜血壓變化情況比較
2.3晝夜血壓變化與ICAS發生的相關性分析單因素Logistic回歸分析結果提示,日間平均血壓升高、夜間平均血壓升高、夜間血壓非杓型改變、夜間血壓反杓型改變均與ICAS的發生無顯著相關性(P>0.05)。校正性別、年齡、糖尿病、血脂異常、吸煙、冠心病等因素后,亦得到相似的結果。見表2。

表2 高血壓患者晝夜血壓變化與ICAS的相關性分析
注:Model 1:未校正混雜因素;Model 2:校正了年齡、性別、糖尿病、血脂異常、吸煙、冠心病等混雜因素
2.4晝夜血壓變化與多發性ICAS發生的相關性分析單因素Logistic回歸分析結果顯示,日間平均血壓升高、夜間平均血壓升高、夜間血壓非杓型改變與多發性ICAS的發生無顯著相關性(P>0.05);而夜間血壓反杓型改變與多發性ICAS的發生密切相關(P<0.05)。校正性別、年齡、糖尿病、血脂異常、吸煙、冠心病等因素后,亦得到相似的結果。見表3。

表3 高血壓患者晝夜血壓變化與多發性ICAS的相關性分析
3討論
正常人群中晝夜血壓呈杓型變化,即夜間血壓較日間血壓降低10%~20%。在高血壓患者中,常出現夜間血壓升高,甚至出現非杓型、反杓型晝夜血壓變化[6]。本組高血壓患者中,夜間血壓升高發生率明顯高于日間血壓升高,夜間血壓非杓型、反杓型改變的發生率高達80%以上。
夜間血壓升高與心腦血管事件的發生密切相關。Sierra等[7]報道,夜間收縮壓升高是發生冠心病和腦卒中的獨立預測因素。Mesquita-Bastos等[1]發現,夜間平均收縮壓升高患者發生冠心病和腦卒中的風險高于日間平均收縮壓升高者,尤其是夜間初始4 h平均收縮壓升高者的風險更高。Hermida等[8]報道,降低高血壓患者夜間血壓水平可以有效降低心血管事件的發生率和病死率。
夜間血壓升高也與動脈粥樣硬化早期亞臨床改變相關。臨床研究發現,夜間血壓非杓型改變患者的內皮功能損傷顯著重于夜間血壓杓型改變患者[9]。青少年代謝綜合征患者夜間平均收縮壓升高與頸動脈內中膜增厚密切相關[10]。中年高血壓患者夜間平均血壓升高、非杓型改變是頸動脈內中膜增厚的獨立預測因素[2]。降低夜間平均血壓,使非杓型血壓轉變為杓型血壓,也可能改善頸動脈內中膜增厚[11]。
夜間血壓變化與ICAS發生相關性的臨床資料很少。史惠霞等[12]報道ICAS患者的夜間平均脈壓顯著高于對照組患者;而ICAS組與對照組之間,夜間平均血壓升高和非杓型的發生率無顯著差異。本研究結果也提示,夜間平均血壓升高、非杓型和反杓型改變與ICAS的發生無關。但進一步分析提示,多發性ICAS的發生與夜間血壓反杓型改變密切相關。由此推斷,夜間平均脈壓增大可能是顱內動脈早期損傷的重要因素;而夜間血壓的反杓型改變則是顱內動脈硬化進展的重要因素。顱內動脈、頸動脈與夜間血壓變化的相關性存在著差異,可能與不同研究中動脈硬化標準有所差異有關,也可能提示顱內、顱外動脈對高血壓病理損害的反應性存在差異。
本研究結果提示,高血壓患者中夜間血壓升高、夜間血壓非杓型、反杓型改變的發生率高;夜間平均血壓升高、夜間血壓非杓型改變、夜間血壓反杓型改變與ICAS的發生無關;但是,夜間血壓反杓型改變可能是多發性ICAS的獨立危險因素。
4參考文獻
[1]Mesquita-Bastos J,Bertoquini S,Polonia J.Cardiovascular prognostic value of ambulatory blood pressure monitoring in a Portuguese hypertensive population followed up for 8.2years[J].Blood Press Monit,2010,15(5):240-246.
[2]Vasunta RL,Kesaniemi YA,Ylitalo A,et al.Nondipping pattern and carotid atherosclerosis in a middle-aged population: OPERA Study[J].Am J Hypertens,2012,25(1):60-66.
[3]Lopez-Cancio E,Galan A,Dorado L,et al.Biological signatures of asymptomatic extra- and intracranial atherosclerosis: the Barcelona-AsIA (Asymptomatic Intracranial Atherosclerosis) study[J].Stroke,2012,43(10):2712-2719.
[4]Chimowitz MI,Lynn MJ,Howlett-Smith H,et al.Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis[J].N Engl J Med,2005,352(13):1 305-1 316.
[5]Hermida RC,Smolensky MH,Ayala DE,et al.2013 ambulatory blood pressure monitoring recommendations for the diagnosis of adult hypertension,assessment of cardiovascular and other hypertension-associated risk,and attainment of therapeutic goals[J].Chronobiol Int,2013,30(3):355-410.
[6]Gorostidi M,Sobrino J,Segura J,et al.Ambulatory blood pressure monitoring in hypertensive patients with high cardiovascular risk: a cross-sectional analysis of a 20,000-patient database in Spain[J].J Hypertens,2007,25(5):977-984.
[7]de la Sierra A,Banegas JR,Segura J,et al.Ambulatory blood pressure monitoring and development of cardiovascular events in high-risk patients included in the Spanish ABPM registry: the CARDIORISC Event study[J].J Hypertens,2012,30(4):713-719.
[8]Hermida RC,Ayala DE,Mojon A,et al.Decreasing sleep-time blood pressure determined by ambulatory monitoring reduces cardiovascular risk[J].J Am Coll Cardiol,2011,58(11):1 165-1 173.
[9]Deyneli O,Yazici D,Toprak A,et al.Diurnal blood pressure abnormalities are related to endothelial dysfunction in patients with non-complicated type 1 diabetes[J].Hypertens Res,2008,31(11):2 065-2 073.
[10]Civilibal M,Duru NS,Elevli M.Subclinical atherosclerosis and ambulatory blood pressure in children with metabolic syndrome[J].Pediatr Nephrol,2014,29(11):2 197-2 204.
[11]趙陽,懷丁.CCB矯正非杓型血壓對頸內動脈內中膜厚度的影響[J].中國實用神經疾病雜志,2010,13(21):35-36.
[12]史惠霞,李春蘭.老年高血壓病患者動態血壓與腦動脈粥樣硬化的關系[J].中國社區醫師,2011,13(13):34.
(收稿2015-05-23)
Association between nocturnal blood pressure and intracranial atherosclerotic stenosis in patients with hypertension
CuiMin,PuJie,LiaoGuanghao,WuLe,WuQian,WuQiang,LiHonghua
DepartmentofNeurology,WuhanGeneralHospitalofGuangzhouMilitaryAreaCommand,Wuhan430070,China
【Abstract】Objective To investigate the relationship between changes of nocturnal blood pressure and presence of intracranial atherosclerotic stenosis (ICAS) in patients with hypertension. Methods The patients with hypertensionc aged ≥ 40 years were enrolled in this study. All subjects underwent ambulatory blood pressure monitoring and magnetic resonance angiography (MRA) of the intracranial vessels. The ICAS was defined as that diameter of the stenosed intracranial large arteries was over 50%. The multi-lesion ICAS was defined as that the number of ICAS lesions was ≥2. According to the daytime and nighttime mean blood pressure (BP) level, the circadian BP pattern was divided into three groups: dipper, non-dipper and inverse-dipper. Results A total of 359 patients with hypertension were enrolled in this study. Of all the 359 patients, 135 patients were classified as the ICAS group, including 86 patients with single-lesion ICAS and 49 patients with multi-lesion ICAS. The daytime mean BP increased in 226 patients (63%), and nocturnal mean BP increased in 322 patients (89.7%). The incidence of dipper, non-dipper and inverse-dipper pattern was 10.3%, 46.2% and 43.5%, respectively. Multivariate Logistic regression analysis showed that the elevated nocturnal mean BP, non-dipper and inverse-dipper pattern were not significantly correlated with the presence of ICAS (P>0.05). However, inverse-dipper pattern was significantly associated with presence of multi-lesion ICAS (P<0.05). Conclusion This study suggests that the inverse-dipper pattern may be an independent risk factor for the presence of multiple lesion ICAS.
【Key words】Hypertension; Ambulatory blood pressure monitoring; Magnetic resonance angiography; Nocturnal blood pressure; Intracranial atherosclerotic stenosis
【中圖分類號】R743
【文獻標識碼】A
【文章編號】1673-5110(2016)08-0014-04
基金項目:湖北省衛生計生科研基金項目(編號:WJ2015Z039)
猜你喜歡
青春期健康(2022年19期)2022-10-12 16:46:40
西部醫學(2021年10期)2021-10-28 08:25:50
中老年保健(2021年5期)2021-08-24 07:07:16
中老年保健(2021年11期)2021-08-22 03:14:10
今日農業(2020年19期)2020-12-14 14:16:52
中國生殖健康(2020年6期)2020-02-01 06:29:06
中國生殖健康(2018年6期)2018-11-06 07:09:44
基層中醫藥(2018年4期)2018-08-29 01:25:58
基層中醫藥(2018年6期)2018-08-29 01:20:14
中國繼續醫學教育(2015年2期)2016-01-06 01:36:28
