記憶障礙遠程康復訓練模式的療效
2016-06-07 08:09:24高明明惲曉平張慧麗郭華珍王科英牛秀蓮喬穎欣
中國康復理論與實踐 2016年5期
高明明,惲曉平,張慧麗,郭華珍,王科英,牛秀蓮,喬穎欣
?
記憶障礙遠程康復訓練模式的療效
高明明1,2,惲曉平1,2,張慧麗1,2,郭華珍1,2,王科英3,牛秀蓮4,喬穎欣5
[摘要]目的觀察記憶障礙遠程康復訓練模式的療效。方法2010年8月~2015年4月,將符合納入標準的記憶障礙患者81例隨機分為對照組(n=26)、儀器組(n=33)和遠程組(n=22)。所有入組患者均服用改善腦血管藥物。儀器組和遠程組分別采用認知康復系統或其遠程康復版進行以記憶康復為主的訓練,共6周。訓練前后采用韋氏記憶量表、Rivermead行為記憶測驗第2版和Rey聽覺詞語學習測驗進行評定。結果訓練后,儀器組和遠程組各項成績較治療前明顯提高(t>3.795,P<0.01),遠程組與儀器組間無顯著性差異(P>0.05)。對照組兩次評定成績無顯著性差異(t<0.771,P>0.05)。結論記憶障礙康復訓練可明顯改善患者的記憶能力,遠程認知康復訓練系統可以達到與本地訓練相近的療效。
[關鍵詞]記憶障礙;認知康復;遠程康復
[本文著錄格式]高明明,惲曉平,張慧麗,等.記憶障礙遠程康復訓練模式的療效[J].中國康復理論與實踐,2016,22(5): 518-522.
作者單位:1.首都醫科大學康復醫學院,北京市100068;2.中國康復研究中心北京博愛醫院康復評定科,北京市100068;3.黑龍江省大慶油田總醫院康復科,黑龍江大慶市163001;4.上海市殘疾人康復職業培訓中心,上海市200127;5.黑龍江省海員總醫院康復科,黑龍江哈爾濱市150020。
獲得性腦損傷(acquired brain injury,ABI)已經成為發達國家重要的致殘因素[1]。世界衛生組織預測,到2020年,ABI的兩大主要疾病腦外傷和腦卒中將會被列為人類最為關注的五大病因[2];其所導致的運動功能障礙及認知障礙等,嚴重影響患者日后的生活。
近10年來,遠程醫療發展迅速,全世界許多國家的衛生系統都已開始應用信息通信技術為身處偏遠地區的患者提供健康服務[3-4]。所謂遠程康復,是指應用計算機技術、互聯網技術以及多媒體信息技術,為功能障礙與殘疾者提供康復服務,支持其獨立生活[5]。遠程康復已涉足認知、語言康復[6-11],吞咽康復[12],運動療法[13-24]、作業療法等領域。基于互聯網的遠程康復使患者得以在基層醫院、社區、家中獲得康復指導,從而實現康復的連續性和可移動性[25-26]。
針對ABI患者,Jelcic等[27]、Poon等[28]應用遠程康復技術分別對早期阿爾茨海默病患者及存在記憶障礙的社區老年人進行認知康復,取得了與傳統面對面療法相近的療效。Ng等[29]與Williamson等[30]將遠程康復技術分別應用于腦外傷患者執行功能及面孔識別障礙的治療。
Azad等[31]與Barton等[32]分別報道了遠程醫療與視頻遠程醫療為醫療資源匱乏的偏遠地區提供便利服務的情況,并提倡持續發展該項技術。Solana等介紹一種名為“Guttmann神經私人助理教練(GNPT)”的遠程認知康復平臺[33];Tost等研發一種基于虛擬環境的認知遠程康復分散式系統[34],均取得較好療效。
國內報道相對較少,主要集中于應用遠程康復技術對腦梗死患者進行家庭運動康復指導[35]及對出院后的腦卒中患者進行電話隨訪[36]等。在香港,治療師和患者/家屬間可通過互聯網進行遠程認知康復評估與訓練[37-39]。
以往研究多數為滿意度調查或電話隨訪,只有少數研究進行療效觀察,且僅限于與面對面治療做比較。本研究應用遠程認知康復系統進行多中心前瞻性記憶障礙康復訓練,旨在觀察記憶障礙遠程康復訓練的療效。
1 資料與方法
1.1一般資料
選擇2010年8月~2015年4月,在中國康復研究中心神經康復科、黑龍江省大慶油田總醫院康復科、上海市殘疾人康復職業培訓中心、黑龍江省海員總醫院康復科收治的住院及門診ABI所致記憶障礙患者。
入選標準:①年齡≥16歲;②生命體征平穩,病情穩定,疾病癥狀不再進展持續48 h以上;③由知情者確認患者有記憶力減退主訴;④簡易精神狀態檢查(Mini-Mental State Examination,MMSE)評分≥16分;蒙特利爾認知評定(Montreal Cognitive Assessment,MoCA)評分≥11分;⑤服用改善腦血管藥物;⑥簽署知情同意書。
排除標準:①言語篩查不能完成兩步指令;②注意力維持時間<5 min;③卒中后抑郁;④長期服用降低認知功能藥物;⑤并發其他神經及精神疾病。
根據標準共入選98例。研究過程中,因病情加重或出現并發癥終止訓練7例,因費用問題中途退出5例,因患者家庭發生重大變故中途退出4例,因訓練強度過大無法繼續配合1例,實際完成試驗者81例。以隨機區組化法分為對照組(n=26)、儀器組(n=33)和遠程組(n=22)。三組間性別及年齡無顯著性差異(P>0.05)。見表1。
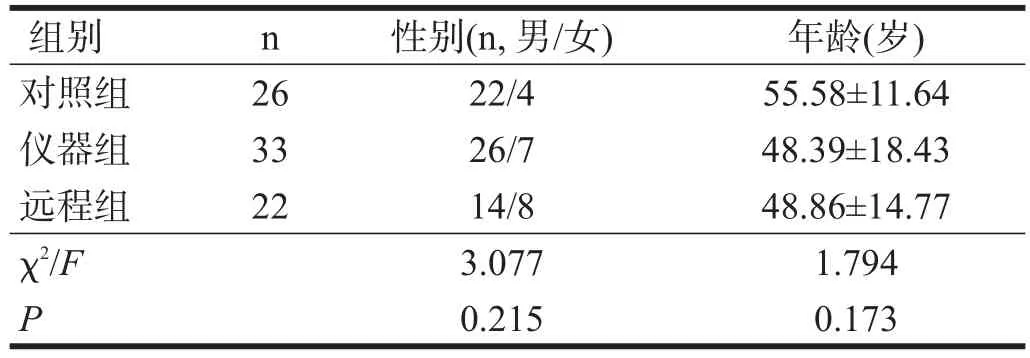
表1 各組一般資料比較
1.2方法
儀器組采用“認知康復診療系統”,遠程組采用“認知康復診療系統遠程康復版”(http://www.jizhiyiliao.com/),每次訓練30 min,每天1次,每周5 d,共6周。兩組訓練內容相同,除少量知覺、注意等輔助訓練外,主要進行記憶功能康復訓練,包括漢字、詞語、段落、空間、圖片、人像人名等記憶及相關日常生活活動能力(activities of daily living,ADL)訓練等。訓練方法綜合應用無錯性學習、聯想、重復、取消提示及間隔提取技術等[40]。對照組研究期內不進行康復訓練,待觀察期結束再行康復。
所有患者均服用改善腦血管藥物,并參加常規運動功能康復。
1.3認知功能評定
包括瞬時、短時及長時記憶的評定。瞬時記憶評定采用修訂版韋氏記憶量表中的瞬時記憶測驗;短時記憶測驗采用韋氏記憶量表中的圖片回憶(權重0.25)、Rivermead行為記憶測驗第2版中的圖片再認(權重0.15)、故事即刻回憶(權重0.30)及聽覺詞語學習測驗(取自Rey聽覺詞語學習測驗,權重0.30);長時記憶評定采用Rivermead行為記憶測驗第2版的故事延遲回憶(權重0.30)和人像延遲回憶(權重0.30)以及定向力(權重0.40)。
各量表計算標準分,根據權重換算成記憶評分。記憶總分=瞬時記憶評分×0.2+短時記憶評分×0.4+長時記憶評分×0.4。
在訓練前及6周訓練結束時分別進行評定。采用成績提高百分比判定療效:≥40A為顯效,20A~<40A為有效,<20A為無效。
1.4統計學分析
采用SPSS 17.0進行數據分析。所有數據均符合正態分布,以表示。組間比較應用多樣本方差分析(ANOVA)及Post Hoc兩兩比較,組內訓練前后比較采用配對t檢驗;性別構成比采用χ2檢驗。療效比較采用非參數檢驗。顯著性水平α=0.05。
2 結果
組內比較,儀器組和遠程組瞬時、短時、長時記憶及總分明顯提高(P<0.01)。對照組兩次成績無顯著性差異(P>0.05)。組間比較,瞬時記憶、短時記憶、長時記憶及總分治療前無顯著性差異,治療后有顯著性差異(P<0.05)。兩兩比較,儀器組和遠程組高于對照組(P<0.05),儀器組與遠程組間無顯著性差異(P>0.05)。見表2~表5。
療效比較,儀器組及遠程組總有效率顯著高于對照組(P<0.001)。見表6。

表2 各組訓練前后瞬時記憶評分比較

表3 各組訓練前后短時記憶評分比較

表4 各組訓練前后長時記憶評分比較

表5 各組訓練前后記憶總分比較

表6 各組臨床療效比較(n)
3 討論
上世紀中后期,許多國家開始應用遠程康復系統為患者服務,服務對象包括早期阿爾茨海默病患者、社區老年人、腦外傷患者等。我國雖起步較晚,但隨著互聯網的廣泛普及,國內城鎮大部分區域已為互聯網所覆蓋,為推廣遠程認知康復提供了可能性。2007年,惲曉平等就提出構建基于互聯網的認知遠程康復治療系統的理念并進行系統研發[41]。2015年,How與臨床醫生合作探討創傷性腦損傷患者的遠程認知康復[42]。本研究應用“認知康復診療系統(遠程康復版)”,實現認知障礙評定診斷基礎上的在線康復。上海、大慶、哈爾濱等地醫院參加本項研究,可為國內推廣遠程認知康復提供示范。
本研究顯示,在訓練內容相同的條件下,遠程認知康復訓練也可顯著改善患者的記憶功能,療效與本地儀器訓練模式相近。遠程認知康復的優勢之一在于患者可不受時間、場所限制,并可一天內多次進行強化訓練。多個認知康復療效機制的研究證實,大量反復訓練和刺激,可增加全腦及局部腦區的血供;促進和激活神經網絡的可塑性改變;改善腦區異常激活模式;相關認知功能腦網絡區域間的功能與結構連接增強或發生重組[43-44]。本研究中,遠程組與儀器組訓練強度相同,療效相近;若充分發揮遠程認知康復的優勢,患者的認知功能有可能得到進一步提升。
本研究通過多中心、前瞻性隨機對照研究,證明遠程認知康復訓練的有效性。遠程認知康復模式及其訓練系統作為一種新興、便捷的康復手段,可作為面對面康復訓練的補充訓練模式,使更多患者受益,適宜在認知康復領域推廣。
[參考文獻]
[1]Brain InjuryAssociation ofAmerica[EB/OL].[2014-03].http:// www.biausa.org/announcements/brain-injury-association-of -america-applauds-introduction-of-national-traumatic-brain-injury-researc.
[2]World Health Organization.Burden Disease Statistics[EB/ OL].[2014-03].http://www.who.int/mediacentre/factsheets/ fs310/en/.
[3]Brennan DM,Tindall L,Theodoros D,et al.A blueprint for telerehabilitation guidelines:October 2010[J].Telemed J E Health,2011,17(8):662-665.
[4]Forducey PG,Ruwe WD,Dawson SJ,et al.Using telerehabilitation to promote TBI recovery and transfer of knowledge[J]. NeuroRehabilitation,2003,18(2):103-111.
[5]Rosen MJ.Telerehabilitation[J].NeuroRehabilitation,1999,12 (1):11-26.
[6]Cherney LR,van Vuuren S.Telerehabilitation,virtual therapists,and acquired neurologic speech and language disorders[C].Seminars in speech and language.NIH Public Access,2012,33(3):243.
[7]Constantinescu G,Theodoros D,Russell T,et al.Treating disordered speech and voice in Parkinson's disease online:a randomized controlled non-inferiority trial[J].Int J Lang Commun Disord,2011,46(1):1-16.
[8]Brennan DM,Georgeadis AC,Baron CR,et al.The effect of videoconference-based telerehabilitation on story retelling performance by brain-injured subjects and its implications for remote speech-language therapy[J].Telemed J E Health,2004,10(2):147-154.
[9]Dechene L,Tousignant M,Boissy P,et al.Simulated in-home teletreatment for anomia[J].Int J Telerehab,2011,3(2):3-10.
[10]Agostini M,Garzon M,Benavides-Varela S,et al.Telerehabilitation in poststroke anomia[J].Biomed Res Int,2014,2014: 706909.
[11]Meyer AM,Getz HR,Brennan DM,et al.Telerehabilitation of anomia in primary progressive aphasia[J].Aphasiology,2016,30(4):483-507.
[12]Ward EC,Sharma S,Burns C,et al.Validity of conducting clinical dysphagia assessments for patients with normal to mild cognitive impairment via telerehabilitation[J].Dysphagia,2012,27(4):460-472.
[13]Trialists ESD.Services for reducing duration of hospital care for acute stroke patients[J].Cochrane Database Syst Rev,2005 (2):CD000443.
[14]Mas Mà,Inzitari M.A critical review of early supported discharge for stroke patients:from evidence to implementation into practice[J].Int J Stroke,2015,10(1):7-12.
[15]Langhorne P,Widen-Holmqvist L.Early supported discharge after stroke[J].J Rehabil Med,2007,39(2):103-108.
[16]Levy CE,Silverman E,Jia H,et al.Effects of physical therapy delivery via home video telerehabilitation on functional and health-related quality of life outcomes[J].J Rehabil Res Dev,2015,52(3):361-370.
[17]Finkelstein J,Wood J,Cha E.Impact of physical telerehabilitation on functional outcomes in seniors with mobility limitations[C].Engineering in Medicine and Biology Society(EMBC),2012 Annual International Conference of the IEEE.IEEE,2012:5827-5832.
[18]Cikajlo I,Rudolf M,Goljar N,et al.Telerehabilitation using virtual reality task can improve balance in patients with stroke[J].Disab Rehabil,2012,34(1):13-18.
[19]Arpaia P,Cimmino P,De Matteis E,et al.A low-cost force sensor-based posturographic plate for home care telerehabilitation exergaming[J].Measurement,2014,51:400-410.
[20]Lin KH,Chen CH,Chen YY,et al.Bidirectional and multi-user telerehabilitation system:clinical effect on balance,functional activity,and satisfaction in patients with chronic stroke living in long-term care facilities[J].Sensors,2014,14(7): 12451-12466.
[21]Lloréns R,Noé E,Colomer C,et al.Effectiveness,usability,and cost-benefit of a virtual reality-based telerehabilitation program for balance recovery after stroke:a randomized controlled trial[J].Arch Phys Med Rehabil,2015,96(3):418-425. e2.
[22]Yip MP,Chang AM,Chan J,et al.Development of the Telemedicine Satisfaction Questionnaire to evaluate patient satisfaction with telemedicine:a preliminary study[J].J Telemed Telecare,2003,9(1):46-50.
[23]Piron L,Turolla A,Tonin P,et al.Satisfaction with care in post-stroke patients undergoing a telerehabilitation programme at home[J].J Telemed Telecare,2008,14(5):257-260.
[24]Linder SM,Rosenfeldt AB,Bay RC,et al.Improving quality of life and depression after stroke through telerehabilitation[J]. Am J Occup Ther,2015,69(2):6902290020.
[25]Bae J,Zhang W,Tomizuka M.Network-based rehabilitation system for improved mobility and tele-rehabilitation[J].IEEE Transactions on Control Systems Technology,2013,21(5): 1980-1987.
[26]Fraunhofer Institute for Open Communication Systems FOKUS,Physio for the Home[Z].Berlin:Research News Fraunhofer,2013-01.
[27]Jelcic N,Agostini M,Meneghello F,et al.Feasibility and efficacy of cognitive telerehabilitation in early Alzheimer's disease:a pilot study[J].Clin Interven Aging,2014,24(9): 1605-1611.
[28]Poon P,Hui E,Dai D,et al.Cognitive intervention for community-dwelling older persons with memory problems:telemedicine versus face-to-face treatment[J].Int J Geriatr Psychiatry,2005,20(3):285-286.
[29]Ng EM,Polatajko HJ,Marziali E,et al.Telerehabilitation for addressing executive dysfunction after traumatic brain injury[J].Brain Inj,2013,27(5):548-564.
[30]Williamson J,Isaki E.Facial affect recognition training through telepractice:two case studies of individuals with chronic traumatic brain injury[J].Int J Telerehabil,2015,7(1):13.
[31]Azad N,Amos S,Milne K,et al.Telemedicine in a rural memory disorder clinic:remote management of patients with dementia[J].Can Geriatr J,2012,15(4):96-100.
[32]Barton C,Morris R,Rothlind J,et al.Video-telemedicine in a memory disorders clinic:evaluation and management of rural elders with cognitive impairment[J].Telemed J E Health,2011,17(10):789-793.
[33]Solana J,Cáceres C,García-Molina A,et al.Improving brain injury cognitive rehabilitation by personalized telerehabilitation services:Guttmann Neuropersonal Trainer[J].IEEE J Biomed Health Inform,2015,19(1):124-131.
[34]Tost D,Grau S,Ferré M,et al.PREVIRNEC:a cognitive telerehabilitation system based on virtual environments[C]. Virtual Rehabilitation International Conference,2009.IEEE,2009:87-93.
[35]李迥,吳莉青,尚淑玲,等.遠程家庭康復指導與腦梗死患者康復效果[J].中國康復醫學雜志,2012,27(6):572-573.
[36]聶衛莉,聶燕芳.出院后電話隨訪在腦卒中康復過程中的效果觀察[J].護理與臨床,2011,15(8):761-762.
[37]譚聲輝,宋元良,文偉光,等.電腦輔助及遠程認知康復的發展與應用[J].中華物理醫學與康復雜志,2003,25(9):572-573.
[38]竇祖林.遠程康復及其在香港的發展[J].中華物理醫學與康復雜志,2003,25(12):761-762.
[39]Tam SF,Man WK,Hui-Chan CWY,et al.Evaluating the efficacy of tele-cognitive rehabilitation for functional performance in three case studies[J].Occup Ther Int,2003,10(1):20-38.
[40]高明明,惲曉平,張慧麗,等.記憶障礙康復訓練的療效研究[J].中國康復理論與實踐,2011,17(6):527-530.
[41]惲曉平,白晶,張慧麗,等.基于因特網的認知遠程康復治療系統的構建[J].中國康復理論與實踐,2007,13(10):901-903.
[42]How TV,Hwang AS,Green REA,et al.Envisioning future cognitive telerehabilitation technologies:a co-design process withclinicians[J].DisabilRehabilAssistTechnol,2016.[Epub ahead of print].
[43]陳正威,張璞,惲曉平.工作記憶訓練對腦卒中患者大腦功能激活的影響[J].中國康復理論與實踐,2015,21(8):929-933.
[44]Chapman SB,Aslan S,Spence JS,et al.Neural mechanisms of brain plasticity with complex cognitive training in healthy seniors[J].Cereb Cortex,2015,25(2):396-405.
CITED AS:Gao MM,Yun XP,Zhang HL,et al.Efficacy of telerehabilitation mode on memory disorders[J].Zhongguo Kangfu Lilun Yu Shijian,2016,22(5):518-522.
Efficacy of Telerehabilitation Mode on Memory Disorders
GAO Ming-ming1,2,YUN Xiao-ping1,2,ZHANG Hui-li1,2,GUO Hua-zhen1,2,WANG Ke-ying3,NIU Xiu-lian4,QIAO Ying-xin5
1.Capital Medical University School of Rehabilitation Medicine,Beijing 100068,China;2.Department of Rehabilitation Evaluation,Beijing Bo'ai Hospital,China Rehabilitation Research Center,Beijing 100068,China;3.Department of Rehabilitation,Daqing Oilfield General Hospital,Daqing,Heilongjiang 163001,China;4.Shanghai Rehabilitation& Vocational Training Center for the Disabled,Shanghai 200127,China;5.Department of Rehabilitation,Haiyuan Hospital,Harbin,Heilongjiang 150020,China
Correspondence to YUN Xiao-ping.E-mail:xiaoping_yun@163.com
Abstract:Objective To investigate the effect of telerehabilitation on memory disorders.Methods From August,2010 to April,2015,81 patients with memory disorders were randomized into control group(n=26),computer-assisted training group(n=33)and telerehabilitation training group(n=22).All the patients accepted medicine to facilitate the recovery of memory.Besides,the computer-assisted training group and the telerehabilitation training group accepted memory-based training programs with cognitive rehabilitation system locally or on network respectively,for six weeks.They were evaluated with Wechsler Memory Scale,Rivermead Behavioural Memory Test-2nd Edition and Rey Auditory Verbal Learning Test before and after training.Results Both computer-assisted and telerehabilitation training groups improved in all the assessment after training(t>4.059,P<0.001).There was no significant difference between them(P>0.05).There was no significant improvement in the control group after training(t<0.771,P>0.05).Conclusion Memory rehabilitation training can significantly improve memory abilities,similar with locally or telerehabilitation system.
Key words:memory disorders;cognitive rehabilitation;telerehabilitation
DOI:10.3969/j.issn.1006-9771.2016.05.007
[中圖分類號]R749.1
[文獻標識碼]A
[文章編號]1006-9771(2016)05-0518-05
基金項目:科技部科技支撐計劃項目(No.2008BAH26B04)。
作者簡介:高明明(1982-),女,河北承德市人,碩士研究生,主要研究方向:高級腦功能障礙的康復。通訊作者:惲曉平,女,教授,主任醫師。E-mail:xiaoping_yun@163.com。
收稿日期:(2016-03-11修回日期:2016-04-29)