國人冠心病合并糖尿病患者接受雷帕霉素洗脫鈷鉻合金支架植入術(shù)后的長期預(yù)后分析
2016-07-25 11:46:42潘月毅瓦哈甫馬木提左武旭楊繼娥錢菊英葛均波
中國臨床醫(yī)學(xué) 2016年3期
潘月毅,瓦哈甫·馬木提,左武旭,楊繼娥,張 峰*,錢菊英,葛 雷,周 俊,葛均波
1. 復(fù)旦大學(xué)附屬中山醫(yī)院心內(nèi)科,上海 200032 2. 新疆維吾爾自治區(qū)喀什地區(qū)第二人民醫(yī)院心內(nèi)科,喀什 844000
?
國人冠心病合并糖尿病患者接受雷帕霉素洗脫鈷鉻合金支架植入術(shù)后的長期預(yù)后分析
潘月毅1△,瓦哈甫·馬木提2△,左武旭1,楊繼娥1,張峰1*,錢菊英1,葛雷1,周俊1,葛均波1
1. 復(fù)旦大學(xué)附屬中山醫(yī)院心內(nèi)科,上海200032 2. 新疆維吾爾自治區(qū)喀什地區(qū)第二人民醫(yī)院心內(nèi)科,喀什844000
[摘要]目的: 評價冠心病合并糖尿病患者植入新型雷帕霉素洗脫鈷鉻合金支架(CoCr-SES)的長期療效和安全性。方法: 以一項前瞻性、多中心注冊研究中植入CoCr-SES的1 045例糖尿病患者為研究對象,隨訪該組患者的死亡、心肌梗死(MI)、血運重建和血栓(ST)等事件的發(fā)生率。主要終點事件定義為由心血管死亡、非致死性MI和靶血管血運重建(TVR)組成的主要不良心血管事件(MACE),臨床隨訪時間為3年。結(jié)果: 在3年隨訪時,1 045例合并有糖尿病的冠心病患者中,主要不良心血管事件(major advere cardiavsacalar event, MACE)發(fā)生率為10.0%,包括41例(3.92%)心血管死亡、38例(3.63%)非致死性MI和25例(2.39%)靶血管血運重建。3年內(nèi)ST的發(fā)生率為1.1%,包括7例(0.7%)早期ST和4例(0.4%)晚期ST。結(jié)論: 冠心病合并糖尿病患者植入CoCr-SES后的3年期MACE及ST的發(fā)生率均較低,為國產(chǎn)CoCr-SES在冠心病合并糖尿病患者中的應(yīng)用提供了有效的證據(jù)。(臨床試驗注冊號:NCT00868829)
[關(guān)鍵詞]冠心病;糖尿病;藥物洗脫支架;鈷鉻合金
目前,接受經(jīng)皮冠狀動脈介入治療(percutaneous coronary intervention, PCI)的患者中約25%合并糖尿病[1]。大量臨床隨機對照研究及薈萃分析結(jié)果顯示,糖尿病患者PCI術(shù)后不良心血管事件的發(fā)生風(fēng)險明顯高于非糖尿病患者[2]。近年來,隨著藥物洗脫支架(drug-eluting stent, DES)的更新?lián)Q代,第二代DES已基本取代第一代DES。研究表明,新一代DES的有效性和安全性較第一代DES有所提高[3-4],其在臨床的應(yīng)用范圍也隨之?dāng)U大。 然而,糖尿病患者的支架選擇仍然備受爭議。Firebird 2鈷鉻合金雷帕霉素藥物洗脫支架(cobalt-chromium sirolimus-eluting stent, CoCr-SES)是由我國自主研發(fā)的新一代DES,在國內(nèi)已被廣泛應(yīng)用于臨床[5-7],但對其在糖尿病患者中的應(yīng)用價值仍研究較少。因此,本研究重點探討新一代CoCr-SES在冠心病合并糖尿病患者中的長期預(yù)后,為CoCr-SES在糖尿病患者中的應(yīng)用提供可靠的安全性及有效性證據(jù)。
1資料與方法
1.1研究設(shè)計該研究為大型前瞻性、多中心臨床注冊研究——FOCUS研究(臨床試驗注冊號:NCT00868829)的一項亞組分析。研究入選了常規(guī)臨床工作中需要進行支架治療的所有患者,1周內(nèi)發(fā)生過急性心肌梗死的患者除外。所有入組患者均只接受Firebird 2 支架治療,隨訪時間為支架置入術(shù)后3年。自2009年3月至2011年1月,共計5 084例患者被入選到FOCUS 研究中,其中4 720例患者完成了3年隨訪。本亞組分析從FOCUS研究中選取了冠心病合并糖尿病的中國患者1 045例作為研究對象,該組患者來自中國各省市共計86個醫(yī)院,能較好地代表國人冠心病合并糖尿病患者人群。研究隨訪該組患者的死亡、心肌梗死、血運重建、血栓等不良事件的發(fā)生率,目的在于探究Firebird 2 支架在冠心病合并糖尿病患者中的長期應(yīng)用價值。
1.2介入治療及用藥所有入選患者均接受標(biāo)準(zhǔn)冠脈造影及支架植入手術(shù)治療。多支病變患者若需植入多枚支架,則所有支架均需選擇Firebird 2支架。術(shù)前用藥包括阿司匹林100 mg/d×3 d,氯吡格雷75 mg/d×3 d,或單次給予阿司匹林及氯吡格雷負荷劑量各300 mg。根據(jù)患者情況,部分患者術(shù)前及術(shù)后48 h合并應(yīng)用血小板糖蛋白Ⅱb/Ⅲa 受體拮抗劑鹽酸替羅非班。患者術(shù)后均接受雙聯(lián)抗血小板藥物治療(氯吡格雷75 mg/d, 阿司匹林100 mg/d)至少12個月,阿司匹林100 mg/d需終生服用。同時根據(jù)患者病情,給予血管緊張素轉(zhuǎn)換酶抑制劑、β受體阻滯劑、硝酸酯類及他汀類藥物治療。
1.3終點事件及定義本研究的主要終點事件為主要不良心血管事件(major adverse cardiovascular event, MACE),MACE 是由心血管死亡、非致死性心肌梗死(myocardial infarction, MI)及靶血管血運重建(target vessel revascularization, TVR)組成的復(fù)合終點事件。次要終點事件則包括構(gòu)成主要終點事件的3個組成成分以及全因死亡、MI、靶病變血運重建(target lesion revascularization, TLR)及學(xué)術(shù)研究學(xué)會(academic research consortium, ARC)定義的確定的/可能的血栓形成(stent thrombosis, ST)。另外,ST 根據(jù)發(fā)生的時間進一步分為早期ST(血栓發(fā)生在支架植入后30 d內(nèi))和晚期ST(血栓發(fā)生在支架植入30 d后)。所有終點事件均按照ARC的定義進行界定。

2結(jié)果
2.1糖尿病患者的臨床特征結(jié)果(表1)表明:在完成3年隨訪的4 720例患者中,具有糖尿病患者1 045例,占冠心病患者的22.1%。糖尿病患者的平均年齡為(64.1±10.4)歲,其中男性63.1%,吸煙患者占31.8%。大部分患者同時合并有高血壓(73.5%),相當(dāng)部分患者并發(fā)高膽固醇血癥(33.5%)。另外,慢性腎衰竭、卒中、心源性休克及冠心病家族史的比例分別為1.9%、8.3%、0.4%和5.5%。1.1%的患者表現(xiàn)為嚴重左心功能不全[左室射血分數(shù)(LVEF)<30%],15.5%的患者既往進行過PCI術(shù),1.5%的患者具有冠狀動脈旁路移植術(shù)(coronary artery bypass grafting, CABG)史,16.7%的患者既往發(fā)生過心肌梗死。穩(wěn)定型心絞痛、不穩(wěn)定型心絞痛及無癥狀心肌缺血的患者分別占18.2%、63.4%和10.0%。
2.2糖尿病患者的病變特點結(jié)果(表2)表明:1 045例冠心病合并糖尿病患者中,共計1 598個靶病變接受了支架植入治療,患者的平均病變數(shù)為1.5±0.7。 其中3.0%的病變位于左主干,43.2%位于左前降支,23.7%位于左回旋支,29.8%位于右冠脈。大部分病變(65.3%)屬于B2/C類病變,復(fù)雜病變包括15.8%的分叉病變、9.3%的冠狀動脈開口病變、4.4%的慢性完全閉塞性病變和12.2%的中重度鈣化病變。參考血管直徑為(2.8±0.7) mm,病變長度為(29.0±17.5) mm,術(shù)前狹窄程度為(86.0±10.3) %。其中,小血管病變和長病變的比例分別為35.8%和42.2%。病變平均植入支架數(shù)為(1.4±0.6)枚,植入支架平均直徑為(2.8±0.7) mm,平均長度為(24.7±7.0) mm。
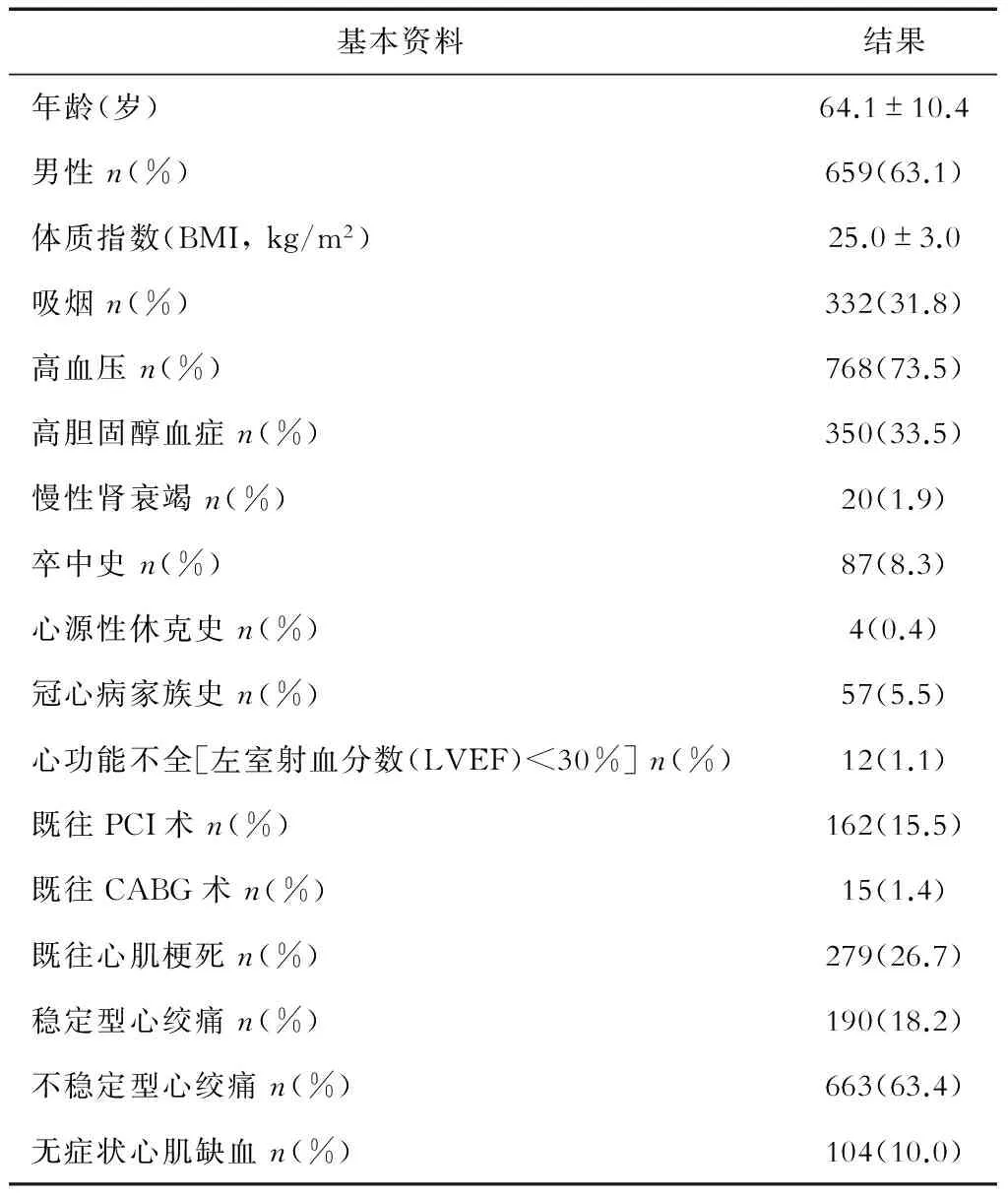
表1 糖尿病患者臨床基線資料 N=1 045
2.3糖尿病患者的臨床預(yù)后冠心病合并糖尿病患者植入CoCr-SES支架3年后,MACE的發(fā)生率為10.0%,包括3.9%(41例)心血管死亡,3.6%(38例)非致死性MI和1.2%(25例)TVR。全因死亡發(fā)生率為55例(5.3%),MI發(fā)生率為4.2%(44例),其中包括1.5%(16例)與靶血管相關(guān)的MI。5.3%患者發(fā)生了血運重建,其中4.8%(50例)為再次PCI,其余0.5%(5例)為CABG。另外,ARC明確的/可能的ST發(fā)生率為1.1%, 包括0.7%(7例)早期ST和0.4%(4例)晚期ST(表3)。
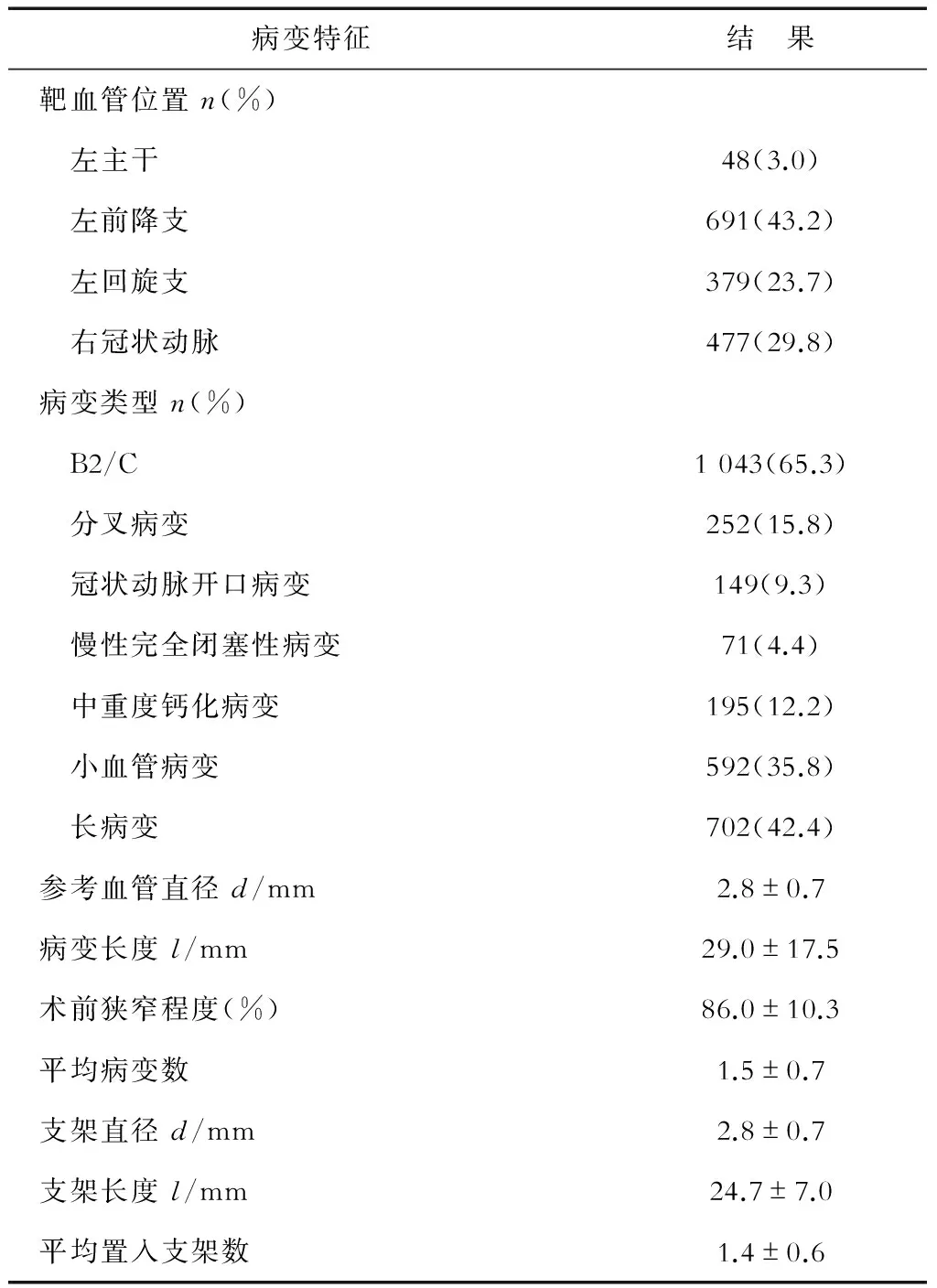
表2 糖尿病患者靶病變特征 N=1 598
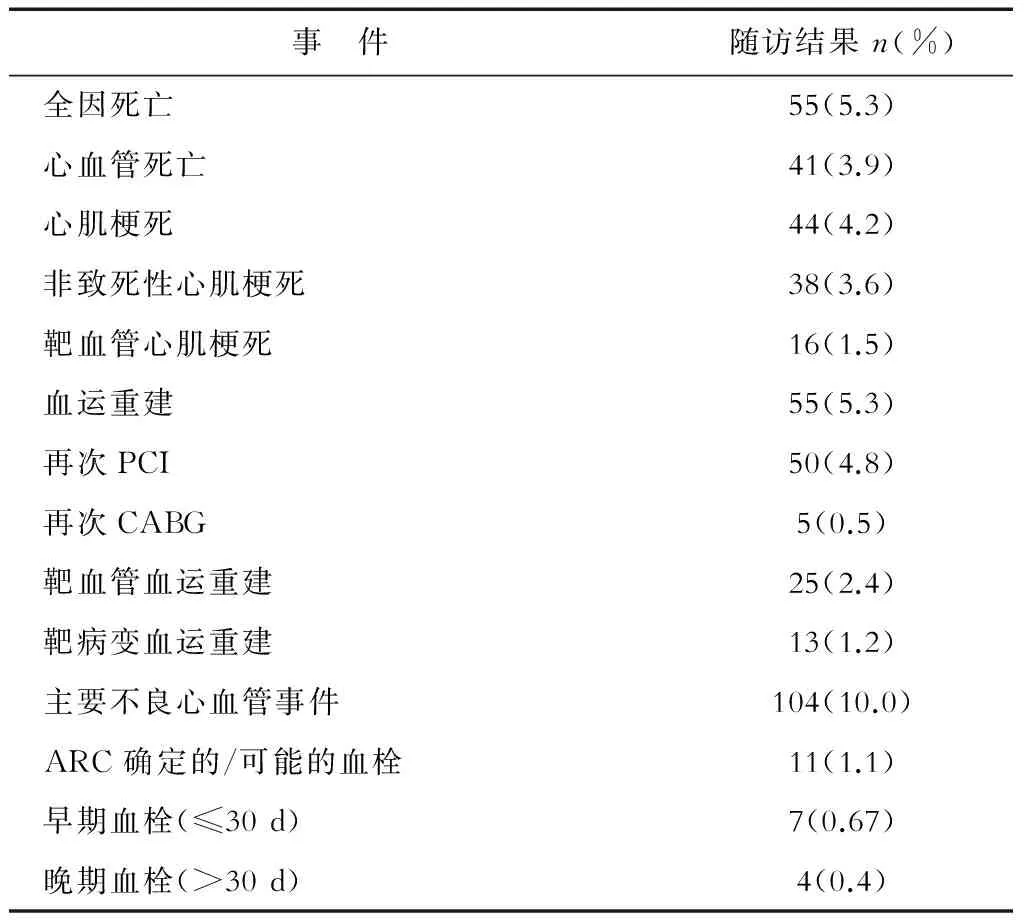
表3 患者3年隨訪結(jié)果
3討論
高血糖一直被認為是冠心病的高危因素之一,糖尿病患者冠心病的發(fā)生率明顯增加。目前,在進行PCI治療的冠心病患者中,25%~30%的患者同時合并糖尿病。在裸支架時代,CABG一直被認為是緩解糖尿病患者心絞痛癥狀及降低患者死亡率最有效的治療手段[9]。然而,隨著支架技術(shù)的革新,DES的問世大大擴展了PCI支架置入術(shù)在復(fù)雜冠心病患者中的應(yīng)用。在過去的20年內(nèi),隨著DES廣泛應(yīng)用于臨床,大量隨機對照研究及大型臨床注冊研究結(jié)果顯示,與裸支架相比,DES 支架能夠顯著降低糖尿病患者支架術(shù)后的再狹窄率及血管重建率。糖尿病患者植入第一代DES后,其血管重建、死亡及心肌梗死的發(fā)生率均明顯降低,分別為12%~24%、15%和18%[10-11],然而其不良事件的發(fā)生率仍明顯高于非糖尿病患者。
與非糖尿病患者相比,糖尿病患者冠脈病變彌漫且小血管受累更為常見[12],這些因素使得糖尿病患者接受支架治療后臨床預(yù)后較差。既往研究表明,糖尿病是影響PCI術(shù)后冠心病患者臨床預(yù)后的獨立危險因素。臨床隨機對照試驗、meta分析和大量臨床登記研究顯示第2代DES的應(yīng)用可以改善糖尿病患者的臨床預(yù)后[13-14]。但對于糖尿病患者PCI術(shù)中支架的選擇尚無定論。Firebird 2 CoCr-SES是在第1代Firebird 雷帕霉素洗脫支架的基礎(chǔ)上研發(fā)的新一代DES,在國內(nèi)已被廣泛應(yīng)用于臨床,然而目前對Firebird 2支架應(yīng)用于冠心病合并糖尿病患者中的安全性及有效性的研究尚少。本研究通過隨訪FOCUS研究中,糖尿病患者植入Firebird 2支架后3年的臨床預(yù)后,首次為Firebird 2支架在國人糖尿病患者中的應(yīng)用提供了可靠的臨床證據(jù)。
本研究亞組分析發(fā)現(xiàn),糖尿病患者植入Firebird 2支架后3年,復(fù)合終點事件MACE的發(fā)生率較低,僅為10%,與目前國際報道的其他類型的第二代DES植入后的MACE發(fā)生率相當(dāng)[10, 13, 15-16]。一項大規(guī)模注冊研究提示DES可顯著降低PCI術(shù)后3年死亡率及心肌梗死的發(fā)生率[10],在我們的研究中,F(xiàn)irebird 2支架植入后3年,全因死亡、心血管死亡及心肌梗死的發(fā)生率均較低。另外,本研究中各種不良事件的發(fā)生率均低于國際報道的第一代DES 植入后不良事件的發(fā)生率。這一方面說明了Firebird 2支架在糖尿病患者中的有效性和安全性明顯高于第一代DES,另一方面也說明了其在國人糖尿病患者中的應(yīng)用價值不差于其他類型的第二代DES。
研究表明,糖尿病患者血小板活性增加[18],因此ST發(fā)生率是糖尿病患者PCI術(shù)后最受關(guān)注的問題之一。既往研究提示,糖尿病患者植入第二代DES后,其血栓發(fā)生率為0.74%~1.60%[19]。我們的分析結(jié)果顯示,F(xiàn)irebird 2支架植入后3年,ST的累計發(fā)生率為1.1%,其中大部分為早期ST,隨著支架置入時間的延長,ST的發(fā)生率也隨之降低,但仍有0.4%的晚期ST發(fā)生。這一結(jié)果進一步證實了Firebird 2支架應(yīng)用于糖尿病患者具有較高的安全性及有效性,為其在糖尿病患者中的廣泛應(yīng)用提供了可靠的證據(jù)。
綜上所述,糖尿病患者植入Firebird 2 CoCr-SES 3年后,其死亡、MI及血運重建的發(fā)生率均較低,總體不良事件的發(fā)生率與國際報道的第二代DES植入后不良事件的發(fā)生率相當(dāng),且明顯優(yōu)于第一代DES。Firebird 2 CoCr-SES作為中國自主研發(fā)的新一代DES,其在糖尿病患者中的應(yīng)用具有較高的安全性和有效性。然而本研究為單組注冊研究,沒有直接與其他二代藥物支架對比,所得結(jié)果為描述性數(shù)據(jù),因此無法避免非對照研究的內(nèi)在局限性。
參考文獻
[1]Wilson SR, Vakili BA, Sherman W, et al. Effect of diabetes on long-term mortality following contemporary percutaneous coronary intervention: analysis of 4,284 cases[J]. Diabetes Care, 2004,27(5):1137-1142.
[2]Van Belle E, Perie M, Braune D, et al. Effects of coronary stenting on vessel patency and long-term clinical outcome after percutaneous coronary revascularization in diabetic patients[J]. J Am Coll Cardiol, 2002,40(3):410-417.
[3]Kedhi E, Gomes ME, Lagerqvist B, et al. Clinical impact of second-generation everolimus-eluting stent compared with first-generation drug-eluting stents in diabetes mellitus patients: insights from a nationwide coronary intervention register[J]. JACC Cardiovasc Interv, 2012,5(11):1141-1149.
[4]Kim WJ, Lee SW, Park SW, et al. Randomized comparison of everolimus-eluting stent versus sirolimus-eluting stent implantation for de novo coronary artery disease in patients with diabetes mellitus (ESSENCE-DIABETES): results from the ESSENCE-DIABETES trial[J]. Circulation, 2011,124(8):886-892.
[5]Ge JB, Zhang F, Qian JY, et al. Six-month clinical outcomes of Firebird 2TM sirolimus-eluting stent implantation in real-world patients with coronary artery diseases[J]. Chin Med J (Engl), 2011,124(6):831-835.
[6]Zhang F, Ge J, Qian J, et al. Real-world use of the second-generation cobalt-chromium sirolimus-eluting stents: 12-month results from the prospective multicentre FOCUS registry[J]. EuroIntervention, 2012,8(8):896-903.
[7]Zhang F, Ge J, Qian J, et al. Two-year clinical outcomes of patients with the second-generation cobalt-chromium sirolimus-eluting stents from the real-world FOCUS registry[J]. Int J Cardiol, 2013,166(3):750-752.
[8]Mavromatis K, Samady H, King SR. Revascularization in patients with diabetes: PCI or CABG or none at all[J]. Curr Cardiol Rep, 2015,17(3):565.
[9]Braunwald E. Effects of coronary-artery bypass grafting on survival. Implications of the randomized coronary-artery surgery study[J]. N Engl J Med, 1983,309(19):1181-1184.
[10]Garg P, Normand SL, Silbaugh TS, et al. Drug-eluting or bare-metal stenting in patients with diabetes mellitus: results from the Massachusetts Data Analysis Center Registry[J]. Circulation, 2008,118(22):2277-2285.
[11]Stenestrand U, James SK, Lindback J, et al. Safety and efficacy of drug-eluting vs. bare metal stents in patients with diabetes mellitus: long-term follow-up in the Swedish Coronary Angiography and Angioplasty Registry (SCAAR)[J]. Eur Heart J, 2010,31(2):177-186.
[12]Luscher TF. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part Ⅱ[J]. Circulation, 2003,108(13):1655-1661.
[13]Ji MS, Jeong MH, Ahn YK, et al. Comparison of Resolute zotarolimus-eluting stents versus everolimus-eluting stents in patients with metabolic syndrome and acute myocardial infarction: propensity score-matched analysis[J]. Int J Cardiol, 2015,199:53-62.
[14]Brener SJ, Kereiakes DJ, Simonton CA, et al. Everolimus-eluting stents in patients undergoing percutaneous coronary intervention: final 3-year results of the Clinical Evaluation of the XIENCE Ⅴ Everolimus Eluting Coronary Stent System in the Treatment of Subjects With de Novo Native Coronary Artery Lesions trial[J]. Am Heart J, 2013,166(6):1035-1042.
[15]Konishi Y, Ashikaga T, Sasaoka T, et al. Comparison of outcomes after everolimus-eluting stent implantation in diabetic versus non-diabetic patients in the Tokyo-MD PCI study[J]. J Cardiol, 2015.
[16]Park KW, Lee JM, Kang SH, et al. Everolimus-eluting Xience v/Promus versus zotarolimus-eluting resolute stents in patients with diabetes mellitus[J]. JACC Cardiovasc Interv, 2014,7(5):471-481.
[17]Moses JW, Leon MB, Popma JJ, et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery[J]. N Engl J Med, 2003,349(14):1315-1323.
[18]Tanaka N, Terashima M, Rathore S, et al. Different patterns of vascular response between patients with or without diabetes mellitus after drug-eluting stent implantation: optical coherence tomographic analysis[J]. JACC Cardiovasc Interv, 2010,3(10):1074-1079.
[19]Dangas GD, Serruys PW, Kereiakes DJ, et al. Meta-analysis of everolimus-eluting versus paclitaxel-eluting stents in coronary artery disease: final 3-year results of the SPIRIT clinical trials program (Clinical Evaluation of the Xience Ⅴ Everolimus Eluting Coronary Stent System in the Treatment of Patients With De Novo Native Coronary Artery Lesions) [J]. JACC Cardiovasc Interv, 2013,6(9):914-922.
[本文編輯]葉婷, 曉璐
[收稿日期]2016-01-28[接受日期]2016-03-09
[基金項目]新疆維吾爾自治區(qū)科技支疆項目計劃(201591154). Supported by Xinjiang Science and Technology Support Programme of the Xinjiang Uygur Autonomous Region (201591154).
[作者簡介]潘月毅,碩士生. E-mail: pyylxa@163.com;瓦哈甫·馬木提,主任醫(yī)師. E-mail: whfmut@163.com *通信作者(Corresponding author). Tel:021-64041990, E-mail: zhang.feng@zs-hospital.sh.cn
[中圖分類號]R 815
[文獻標(biāo)志碼]A
Long-term prognosis of cobalt-chromium sirolimus-eluting stent implantation in patients with coronary heart disease complicated with diabetes mellitus
PAN Yue-yi1△, MAMUTI Wahafu2△, ZUO Wu-xu1, YANG Ji-e1, ZHANG Feng1*, QIAN Ju-ying1, GE Lei1, ZHOU Jun1, GE Jun-bo1
1. Department of Cardiology, Zhongshan Hospital, FudanUniversity, Shanghai200032, China 2. Department of Cardiology, Kashgar Prefecture Second People’s Hospital, Kashgar844000, Xinjiang, China
[Abstract]Objective: To evaluate the long-term efficacy and safety of a novel type of cobalt-chromium sirolimus-eluting stent (CoCr-SES) in patients with coronary artery disease (CAD) complicated with diabetes mellitus (DM).Methods: A total of 1 045 Chinese patients with DM were enrolled into a prospective, multicenter registered research and followed up for the incidence of death, myocardial infarction (MI), blood circulation reconstruction and thrombosis (ST) among other events.The primary endpoint was a major adverse cardiovascular event (MACE), which was composed of cardiovascular death, non-fatal myocardial infarction (MI) and target vessel revascularization (TVR), with a clinical follow-up of 3 years.Results: During the 3-year follow-up, among 1 045 cases of coronary heart disease complicated with diabetes mellitus, the rate of MACE was 10.0%, including 41 cases (3.9%) of cardiovascular death, 38 cases (3.6%) of non-fatal MI and 25 cases (2.4%) of TVR. The incidence of stent thrombosis (ST) was 1.1% in 3 years, including 7 cases (0.7%) of early ST and 4 cases (0.4%) of advanced ST.Conclusions: The incidence of MACE and ST is low in patients with coronary heart disease complicated with diabetes at 3 years after implantation of CoCr-SES, providing compelling evidence for the wide use of domestic CoCr-SES in patients with coronary heart disease complicated with diabetes. (Clinical Registry No. NCT00868829)
[Key Words]coronary artery disease; diabetes mellitus; drug-eluting stent; cobalt-chromium
△共同第一作者(Co-first authors).
·論著·
猜你喜歡
中老年保健(2022年5期)2022-08-24 02:35:42
中老年保健(2022年1期)2022-08-17 06:14:56
中老年保健(2021年5期)2021-08-24 07:07:20
中老年保健(2021年9期)2021-08-24 03:51:04
中老年保健(2021年7期)2021-08-22 07:42:16
中老年保健(2021年11期)2021-08-22 03:15:16
天津醫(yī)科大學(xué)學(xué)報(2021年4期)2021-08-21 02:14:32
基層中醫(yī)藥(2020年10期)2020-11-27 01:58:58
智慧健康(2019年36期)2020-01-14 15:22:58
中國衛(wèi)生標(biāo)準(zhǔn)管理(2015年3期)2016-01-14 03:41:45
