慢性心力衰竭合并貧血臨床特征分析
2016-09-09 09:42:36范新俊馬禮坤
中國現代醫學雜志 2016年14期
范新俊,馬禮坤
(安徽醫科大學附屬省立醫院 心內科,安徽 合肥 230001)
慢性心力衰竭合并貧血臨床特征分析
范新俊,馬禮坤
(安徽醫科大學附屬省立醫院 心內科,安徽 合肥 230001)
目的通過回顧性研究慢性心力衰竭(CHF)患者合并貧血臨床特征,探討其臨床價值。方法將CHF合并貧血的患者作為觀察組(68例),不合并貧血癥狀的患者為對照組(38例),并依據心功能分級為Ⅱ~Ⅳ級,分別比較兩組患者心功能情況和臨床癥狀,探究貧血與老年CHF嚴重程度之間的相關性。結果在患者一般資料中,兩組在左心室射血分數和左心室舒張末內徑比較差異有統計學意義;兩組貧血數據指標中,血紅蛋白和貧血發生率以及鐵缺乏發生率比較差異有統計學意義;血清鐵蛋白水平在對照組與心功能Ⅳ組比較差異有統計學意義;血清鐵水平在對照組分別與心功能Ⅱ級組、Ⅲ級組、Ⅳ級組之間以及在心功能Ⅱ級組與Ⅳ級組、心功能Ⅲ級組與Ⅳ級組之間比較差異有統計學意義;血紅蛋白水平在對照組分別與心功能Ⅱ級組、Ⅲ級組、Ⅳ級組之間比較差異有統計學意義;患者貧血發生率對照組分別與心功能Ⅱ級組、Ⅲ級組、Ⅳ級組之間比較差異有統計學意義;患者鐵缺乏發生率對照組分別與心功能Ⅲ級組、Ⅳ級組之間以及在心功能Ⅱ級組與Ⅲ級組之間比較差異有統計學意義;觀察組中的貧血患者與非貧血患者在鐵缺乏發生率、血清鐵蛋白、血清鐵比較差異有統計學意義。結論貧血發生率、鐵缺乏發生率在重度心力衰竭組的發生率明顯高于輕、中度心力衰竭組,對于CHF鐵缺乏患者,進行適當的鐵劑補充,可以改善患者心功能癥狀。
慢性心力衰竭;貧血;鐵缺乏
據目前統計慢性心力衰竭(chronic heart failure,CHF)占全球人口2%左右[1],在心血管疾病中已經成為最重要的死亡原因,據不完全統計在住院的患者當中有將近25%發生心力衰竭[2],而我國目前的CHF的發生率為0.9%[3];在臨床當中,筆者發現有部分CHF患者有貧血癥狀,為了能夠進一步了解CHG與貧血的相關性,筆者對CHF患者進行分析總結,將貧血與CHF的相關性進行報道如下。
1 資料與方法
1.1臨床資料
選取安徽醫科大學附屬省立醫院心內科2014~2015年出現68例CHF患者(觀察組)。根據美國心臟協會(New York heart association,NYHA)進行心功能分級[4],貧血患者都符合貧血的診斷標準[5]。其中,男性30例(44.12%),合并貧血36例(52.94%)。對照組選擇38例心臟病患者。心電圖(Electrocardiogram,ECG)及心臟超聲(ultrasound cardiogram,UCG)檢查無異常,沒有感染、血液疾病等慢性病可能影響鐵代謝,其中,男性14例(36.84%)。
1.2統計學方法
查閱觀察組68例CHF患者的病例資料,統計分析患者一般資料以及記錄患者的貧血指標、鐵代謝指標等相關數據。采用SPSS 20.0統計軟件進行數據分析,計量資料用均數±標準差()表示,計數資料用例數與百分比(%)表示,用χ2檢驗,組間比較用t檢驗;多組間差異的顯著性分析用單因素方差分析;分析分類反應變量與多自變量的關系用二分類變量的Logistic回歸模型,P<0.05為差異有統計學意義。
2 結果
2.1患者一般資料情況
在患者一般資料中,兩組在左心室射血分數和左心室舒張末內徑比較差異有統計學意義,在性別、年齡、吸煙史、體重指數、三酰甘油、高密度脂蛋白、低密度脂蛋白、總膽固醇、腎小球濾過率均差異無統計學意義(P>0.05)。觀察組男性30例(44.12%),對照組男性14例(36.84%),觀察組吸煙30例(44.12%),對照組吸煙14例(36.84%)。見表1。
2.2兩組貧血數據指標比較
兩組貧血數據指標比較,血紅蛋白和貧血發生率以及鐵缺乏發生率差異有統計學意義,兩組在血清鐵蛋白、血清鐵、總鐵結合力和平均紅細胞體積比較差異無統計學意義。見表2。

表1 兩組患者一般資料
2.3對照組貧血指標與觀察組的心功能分級分別進行比較
白蛋白在觀察組NYHAⅡ級、NYHAⅢ級和NYHAⅣ級與對照組比較差異有統計學意義,白蛋白在觀察組NYHAⅡ級、NYHAⅢ級和NYHAⅣ級組間比較差異無統計學意義;貧血發生率在觀察組NYHAⅡ級、NYHAⅢ級和NYHAⅣ級與對照組比較差異有統計學意義,貧血發生率在觀察組NYHAⅣ級與NYHAⅢ級比較差異有統計學意義;鐵缺乏發生率在觀察組NYHAⅢ級和NYHAⅣ級與對照組比較差異有統計學意義,鐵缺乏發生率在觀察組NYHAⅢ級與NYHAⅡ級比較差異有統計學意義;血清鐵蛋白在觀察組NYHAⅣ級與對照組比較差異有統計學意義;血清鐵在觀察組NYHAⅡ級、NYHAⅢ級和NYHAⅣ級與對照組比較差異有統計學意義,血清鐵在觀察組NYHAⅣ級與NYHAⅢ級比較差異有統計學意義,同時在血清鐵在觀察組NYHAⅣ級與NYHAⅡ級比較差異有統計學意義。見表3。
2.4觀察組中貧血患者與非貧血患者比較
觀察組中的貧血患者與非貧血患者鐵缺乏發生率、血清鐵蛋白、血清鐵比較差異有統計學意義,而總鐵結合力在觀察組中的貧血患者與非貧血患者比較差異無統計學意義。見表4。
2.5觀察組患者的危險因素分析
血清鐵和血清鐵蛋白觀察組患者的危險因素間的比較差異無統計學意義,血紅蛋白可以作為心力衰竭患者的獨立危險因素。見表5。
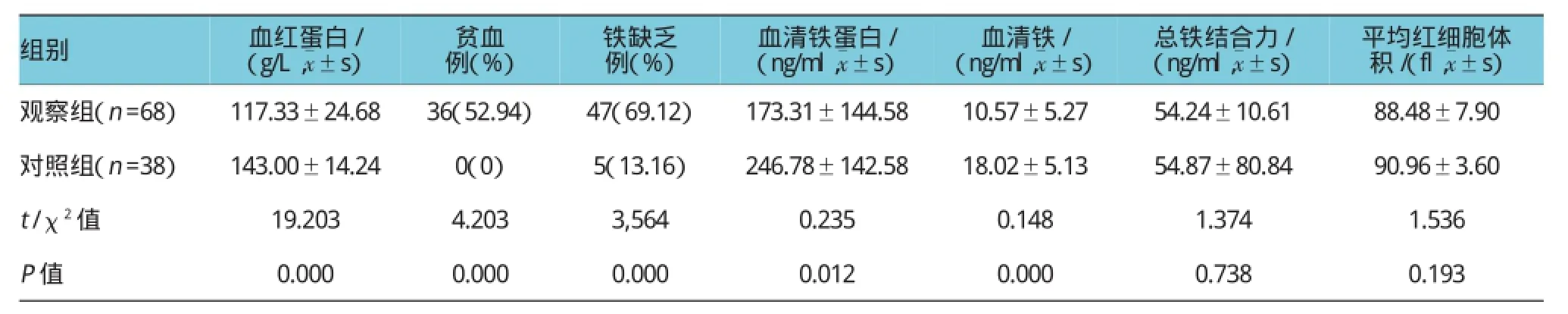
表2 兩組貧血數據指標比較
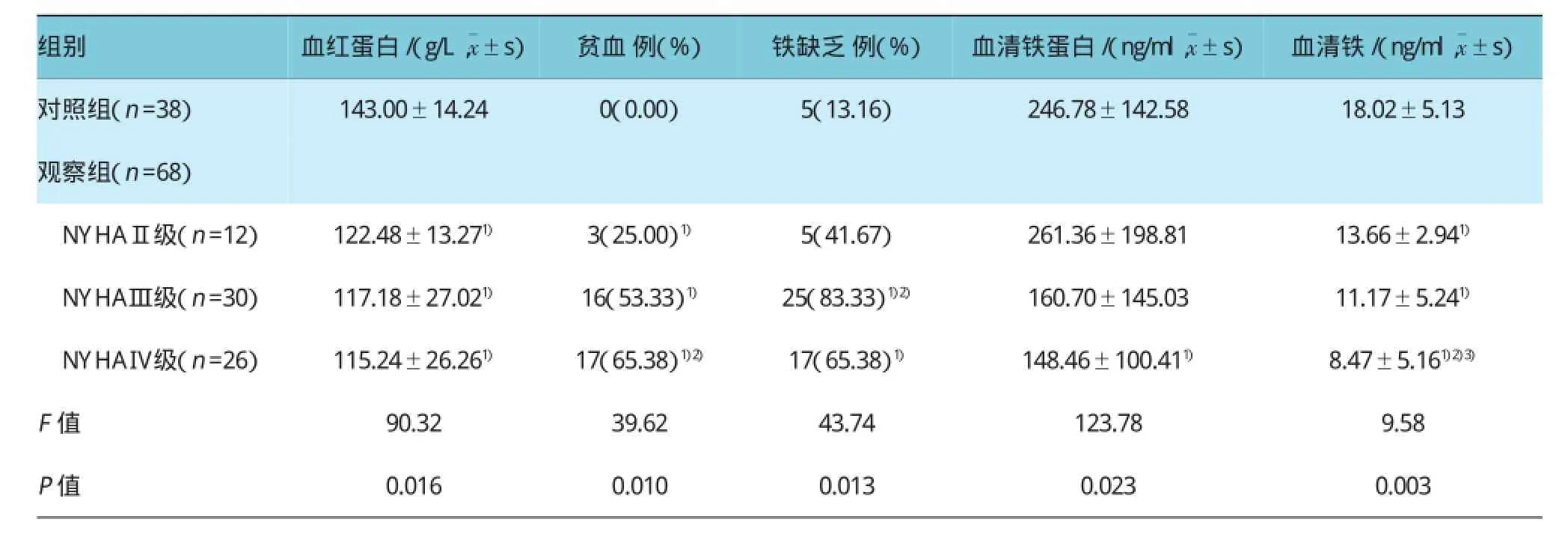
表3 對照組貧血指標與觀察組的心功能分級分別進行比較

表4 觀察組中貧血患者與非貧血患者比較

表5 觀察組患者的危險因素分析
3 討論
據相關文獻報道分析貧血已經是CHF死亡率增高的獨立危險原因之一[6],在文獻報道中貧血患者在CHF的出院患者當中構成比達到17%[7],也有報道在CHF中鐵缺乏引起的貧血比例達到40%之多[8],本研究發現,觀察組患者貧血36例,其發生率為52.94%,觀察組患者鐵缺乏47例,其發生率為69.12%,對照組患者鐵缺乏5例,其發生率為13.16%。筆者發現,按照貧血的診斷標準,觀察組患者貧血發生率與對照組比較差異有統計學意義,研究結果和國內外研究結果類似,也充分說明CHF患者并發貧血的發生率比較高[9-11];到目前為止已有多項報道顯示貧血能夠增加心力衰竭患者的死亡發生率,是CHF死亡率增高的獨立危險[12];血紅蛋白作為貧血的標志物,筆者還通過觀察血紅蛋白的水平,進一步研究血紅蛋白和CHF的相關性;眾所周知,血紅蛋白是紅細胞(red blood cell,RBC)的功能主要完成者,主要是在RBC內具有運輸氧O2和二氧化碳CO2;當CHF患者的血紅蛋白水平下降的時候,CHF患者的循環系統有可能向不好的方向發展,進而加劇患者心功能的惡化[13];據相關文獻報道,CHF患者的血紅蛋白水平與再次住院率和死亡發生率有一定相關性,血紅蛋白越低,再次住院率和死亡發生率也會越低,CHF患者的血紅蛋白每降低10 g/L,死亡的發生率增加到16%左右[14];本課題組統計發現血紅蛋白在觀察組和對照組比較差異有統計學意義,顯示出患者的心功能下降,血紅蛋白也有降低的趨勢,由此來看在CHF住院患者當中進行復查血紅蛋白的含量,有利于幫助臨床醫務人員對CHF患者的治療。
最近國內外相關文獻報道顯示,CHF患者也常常并發鐵缺乏(iron deficiency,ID),鐵的缺乏會引起人體的血紅蛋白合成進行性減少,進一步影響RBC運輸O2和CO2的能力,從而影響患者的循環系統[15-16];有文獻報道顯示[17-18],ID會引起相關機制導致患者心臟的心肌不同程度的增厚和擴張,甚至纖維化,CHF患者ID的缺乏會間接引起人體的運動耐力進行性降低,并且能夠在血紅蛋白降低之前,ID在人體內就已經發生一系列變化;而本研究統計發現,觀察組患者鐵缺乏47例,其發生率為52.94%,對照組患者鐵缺乏僅為5例,其發生率為13.16%,鐵缺乏發生率兩組比較差異有統計學意義,鐵缺乏發生率在觀察組NYHAⅢ級和NYHAⅣ級與對照組比較差異有統計學意義,鐵缺乏發生率在觀察組NYHAⅢ級與NYHAⅡ級比較差異有統計學意義,這也進一步證實鐵缺乏會引起患者心功能惡化,在心力衰竭患者當中鐵缺乏比較低,醫務人員在臨床當中不能忽視檢查單鐵缺乏的標記,對于心功能NYHAⅢ級和NYHAⅣ級的患者要更加注意鐵缺乏;血清鐵蛋白是人體中鐵的重要儲存方式,也是人體內鐵含量最多蛋白復合物,當機體發生改變的時候,人體中血清鐵蛋白水平會出現升高或者降低,而本研究統計發現,血清鐵蛋白在觀察組NYHAⅣ級與對照組比較差異有統計學意義,說明患者心功能越差,血清鐵蛋白表現越顯著。
本研究統計分析發現,觀察組中貧血36例,發生率為52.94%,鐵缺乏47例,發生率為69.12%,貧血的發生率低于ID的發生率,觀察組中的貧血患者與非貧血患者在鐵缺乏發生率、血清鐵蛋白、血清鐵比較差異有統計學意義,而總鐵結合力在觀察組中的貧血患者與非貧血患者比較差異無統計學意義,觀察組中的貧血患者鐵缺乏30例,發生率為83.33%,也說明CHF患者ID與貧血具有一定相關性,筆者也發現觀察組中的非貧血患者鐵缺乏17例,發生率為53.13%,說明ID在患者沒有發生貧血之前出現,也進一步顯示在臨床過程當中,CHF患者中早期應該進行ID的篩查提供數據支持,對于CHF鐵缺乏患者,進行適當的鐵劑補充,可以改善患者心功能癥狀。
[1]PFEFFER M A,KARL S,GRANGER CB,et al.Effects of candesartan on mortality and morbidity in patients with chronic heart failure:the charm-overall programme[J].Lancet,2004,10(2):114.
[2]MCMURRAY JJ,ADAMOPOULOS S,ANKER SD,et al.Esc guidelines for the diagnosis and treatment of acute and chronic heart failure 2012[J].European Journal of Heart Failure,2012,14(8): 803-869.
[3]姜紅,葛均波.心力衰竭流行病學特點[J].中國醫學前沿雜志:電子版,2010,2(1):1-5.
[4]王吉耀.臨床內科學[M].上海:復旦大學出版社,2003:196.
[5]張之南.血液病診斷及療效標準[M].北京:科學出版社,2007:71.
[6]SHAH R,AGARWAL A K.Anemia associated with chronic heart failure:current concepts[J].Clinical Interventions in Aging,2013,8: 22-111.
[7]TAKESHI Y.Prognostic impacts of anemia in patients with chronic heart failure:an interim analysis of the chart-2 study[J]. Journal of Cardiac Failure,2014,20(8):S100.
[8]YAMAUCHI T,SAKATA Y,TAKADA T,et al.Prognostic impact of anemia in patients with chronic heart failure-with special reference to clinical background:report from the chart-2 study[J]. Circulation Journal,2015,79(9):1984-1993.
[9]TAKADA T,SAKATA Y,MIYATA S,et al.Different impact of anemia in chronic heart failure with preserved vs.reduced ejection fraction-a report from the chart-2 study[J].Journal of Cardiac Failure,2013,19(10):S134-S134.
[10]ENJUANES C,KLIP I T,BRUGUERA J,et al.Iron deficiency and health-related quality of life in chronic heart failure:results from a multicenter european study[J].International Journal of Cardiology,2014,174(2):268.
[11]NAITO Y,SAWADA H,OBOSHI M,et al.Iron restricted pair feeding attenuates hypertension and renal damage in a rat model of chronic kidney disease[J].Circulation,2014,130(Suppl 2): A14817.
[12]SHAN H,GUO Y,PENG J Q,et al.Progress of anemia in chronic heart failure[J].Progress in Modern Biomedicine,2014, 14(17):3377-3379.
[13]PEREIRA C A,ROSCANI M G,ZANATI SG,et al.Anemia, heart failure and evidence-based clinical management[J].Arquivos Brasileiros De Cardiologia,2013,101(1):87.
[14]NICOLAS F,FABIEN D,MARC L,et al.Cardiorenal anemia syndrome in chronic heart failure contributes to increased sympathetic nerve activity[J].International Journal of Cardiology, 2013,168(3):2352.
[15]FILIPPATOS G,FARMAKIS D,COLET J C,et al.Intravenous ferric carboxymaltose in iron-deficient chronic heart failure patients with and without anaemia:a subanalysis of the fair-hf trial[J].European Journal of Heart Failure,2013,15(11):1267.
[16]INéS R,ALEXANDRA G,CARLA D S,et al.Iron deficiency status irrespective of anemia:a predictor of unfavorable outcome in chronic heart failure patients[J].Cardiology,2014,128(4): 320-326.
[17]ZHOU S,ZHUANG Y,ZHAO W,et al.Protective roles of erythropoiesis-stimulating proteins in chronic heart failure with anemia[J].Experimental&Therapeutic Medicine,2014,8(3): 863-870.
[18]WEN CY,YI D.Clinical effect of erythropoietin combined with iron oral on the patients of chronic heart failure complicated with anemia[J].Jilin Medical Journal,2013(19):3785-3787.
(張蕾編輯)
Clinical characteristics of chronic heart failure with anemia and iron deficiency
Xin-jun Fan,Li-kun Ma
(Department of Cardiology,Anhui Provincial Hospital,Anhui Medical University,Hefei,Anhui230001,China)
Objective To investigate the clinical characteristics of chronic heart failure patients with anemia by retrospective study and discuss their clinical value.Methods The patients of chronic heart failure with anemia were marked as observation group(n=68),those without anemia marked as control group(n=38),and their cardiac function was classified into Ⅱ-Ⅳ.Cardiac function and clinical symptoms were compared between the two groups. The relationship between anemia and severity of chronic heart failure was investigated in elderly people.Results In the general information of the patients,the left ventricular ejection fraction and the left ventricular end diastolic diameter were significantly different between both groups.Comparing anemia data of the two groups,hemoglobin and the incidence of iron deficiency and anemia were significantly different.Serum ferritin level was significantly different between the control group and cardiac function Ⅳ group.The serum iron level was significantly different between the control group and the heart function Ⅱ,Ⅲ and Ⅳ groups,and between heart function Ⅳ group and heart function Ⅱ and Ⅲ groups.There were significant differences in the hemoglobin level and the incidence of anemia between the control group and the heart function Ⅱ,Ⅲ and Ⅳ groups.The iron-deficiency incidence wassignificantly different between the control group and the heart function Ⅲ and Ⅳ groups,and between the heart function Ⅱ group and the heart function Ⅲgroup.In the observation group,the anemia patients and non-anemia patients had statistical differences in iron-deficiency occurrence rate,serum ferritin and serum iron.Conclusions The incidence of iron deficiency and anemia in the severe heart failure group is obviously higher than that of mild and moderate heart failure groups.To chronic heart failure patients with iron deficiency,proper complement of iron agent can improve cardiac function in patients with symptoms.
chronic heart failure;anemia;iron deficiency
R 541.6
B
10.3969/j.issn.1005-8982.2016.14.016
1005-8982(2016)14-0082-05
2016-02-01
馬禮坤,E-amil:lkma119@163.com
猜你喜歡
新少年(2022年9期)2022-09-17 07:10:54
中老年保健(2021年3期)2021-08-22 06:50:04
天津醫科大學學報(2021年2期)2021-03-29 05:31:08
現代臨床醫學(2021年1期)2021-01-26 00:56:02
小天使·一年級語數英綜合(2020年6期)2020-12-16 02:56:41
護士進修雜志(2017年2期)2017-02-26 14:32:29
中國衛生標準管理(2015年18期)2016-01-20 09:27:12
北極光(2014年8期)2015-03-30 02:50:51
中國醫藥科學(2015年2期)2015-02-27 12:32:09
中醫研究(2014年2期)2014-03-11 20:28:19