A comparison study of Quetiapine and Risperidone’s effectiveness and safety on treating alcohol-induced mental disorder
2016-12-09 07:45:57BeiLVHaishuiDUAN
上海精神醫(yī)學(xué) 2016年4期
關(guān)鍵詞:安全性
Bei LV, Haishui DUAN
·Original research article·
A comparison study of Quetiapine and Risperidone’s effectiveness and safety on treating alcohol-induced mental disorder
Bei LV, Haishui DUAN
mental disorder, alcohol, Quetiapine, effectiveness
1. Introduction
Psychoactive substance is referred to as the kind of chemical substance that can affect people’s emotion,daily behavior and the state of consciousness, and result in abusing substances[1]. The symptoms of the mental disorders caused by that mainly include hallucinations,delusions, emotional impulsiveness, being paranoid and so on[2]. Previous studies suggest that the prognosis of psychoactive substance-induced mental disorders is always bad. For psychoactive substance-induced mental disorders, the psychotic symptoms are always remained,and the social function will be impaired if it is severe.Alcohol-induced mental disorder is a clinically common disorder induced by abusing psychoactive substances;taking medicine is the first choice of treating this kind of disorder, and large doses of B vitamins combining with small doses of antipsychotics are mostly used in clinical settings currently[3]. Several foreign studies have shown that treating mental disorders induced by psychoactive substances with Quetiapine and Risperidone can achieve good effectiveness, and both drugs can control hallucinations and delusions effectively. However, little research has been done to compare these two drugs.The present study found that treating alcohol-induced mental disorder with Quetiapine is effective with a low chance of adverse reactions, and it is reported as the following.
2. Material, participants and methods
2.1 Study design
The present study adopted a randomized, open and controlled design. It is an analysis of clinical cases.
2.2 Choosing cases
The process used to recruit participants is presented in Figure 1. All participants were the patients with alcoholinduced mental disorder who were admitted into our hospital from January 2012 to December 2014. In order to compare the differences between treating mentally ill patients with Quetiapine and Risperidone, the possible confounding factors needed to be eliminated. Therefore,the present study only recruited mentally ill patients whose main medicine was Quetiapine or Risperidone in our hospital. One hundred and seventy-nine patients who were below 60 were recruited initially, then 31 patients were excluded due to a variety of reasons(i.e. Six patients were excluded during the treatment.Seven patients refused to participate in the randomized controlled study. Four patients could not stop relevant medicines before the study. Four patients failed to follow the instructions to take medicine. Four patients took their consent forms back. Two patients have other histories of abusing substances. Two patients were receiving psychological therapy. Two patients dropped out.). Then 148 patients were divided into two groups by random numbers. There were 75 patients in the experimental group with the age range from 33 to 57.The average age was 40.1 (6.3), and the average year of abusing alcohol was 11.7 (7.1). The average course of disease was 23.1 (6.5) months. The control group was constituted by 73 patients with an age range from 31 to 58. The average age was 39.8 (6.0), and the average year of abusing alcohol was 12.1 (6.8). The average course of disease was 22.7 (6.3) months. The ages and histories of abusing alcohol of both groups were not different significantly, so they were comparable. This study design was approved by the ethic committee of Chongqing San Xia Central Hospital. The participants and their family have signed the consent forms.
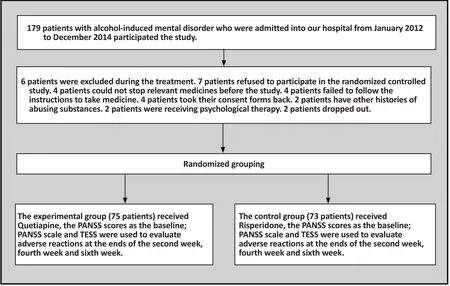
Figure 1. Flowchart of the study
Diagnosis and inclusion criteria: All patients met the criteria of psychoactive substance-induced mental disorder in Chinese classification and diagnostic criteria of mental disease, the third version (CCMD-3)[4]. 1) They met the criteria of psychoactive substance-induced mental disorder in Chinese classification and diagnostic criteria of mental disease, the third version (CCMD-3),and there was exact evidence indicating the substance was alcohol; 2) The patients’ scores in Positive and Negative Syndrome Scale (PANSS) were equal to or above 60[5]; 3) Patients’ physical examination and testing results were normal, and there was no relevant drug contraindications; 4) The age range was 18-60; 5)The legal guardians have signed the consent forms.
Exclusion criteria: 1) The patients who had severe medical conditions and could not tolerate relevant drugs were excluded; 2) The patients who had other substance abuse history, or were in lactation or were pregnant were excluded; 3) The patients who were diagnosed with schizophrenia, bipolar disorder or other mental disorders were excluded; 4) The patients who were allergic to Quetiapine or Risperidone were excluded; 5) The patients whose legal guardians refused to participate were excluded; 6) The patients who had to receive electrical stimulation therapies or psychological therapies or other therapies that might compromise the results of the present study were excluded.
Drop-out criteria: 1) The patients who became intolerant of the drugs or suffered from worse symptoms could drop out; 2) The patients who refused to participate, lost contact or had other unexpected situations could drop out; 3) The patients who did not take medicine according to the instruction could drop out.
2.3 Medicine
Quetiapine, product name: Qi Wei, dose: 100mg, Hunan Dong Ting Pharmaceutical Co., Ltd, China, approved number: H2000466.
Risperidone, product name: Wei Si Tong, dose: 1mg per tablet, Xian Yang Sen Pharmaceutical Co., Ltd, China,approved number: H20010309.
2.4 Grouping and treatment
The present study is a 6-week randomized, double-blind,controlled clinical study. One hundred and forty-eight patients were divided into the experimental group (i.e.receiving Quetiapine, 75 cases) and the control group(i.e. receiving Risperidone, 73 cases) with randomized number generated by a computer. In order to be clean,all patients stopped taking any relevant medicine a week before the study, and they also stop drinking alcohol,smoking and other factors that might have an effect on their prognoses. The patients in the experimental group took Quetiapine orally. In the first week of the treatment, the dose was increased gradually. In other words, on the first and second days, they took 25 mg three times per day, and then the dose was increased by 25 mg every two days. On the seventh day, the dose was 75 mg three times per day. In the second week of the treatment, the dose was adjusted within 100-300 mg every day, depending on patients’ symptoms and tolerance of the medicine, and the average dose was 151.2 (27.3) mg. The course of treatment was 6 weeks.The patients in the control group took Risperidone orally, starting with 1 mg/d. The dose was increased to 4 mg/d gradually, and was adjusted according to the symptoms and tolerance of the medicine. The highest dose was 6 mg/d, and the average dose was 2.3 (0.9)mg/d. The course of treatment was also 6 weeks. During the treatment course, all patients did not take other antipsychotics at the same time. For the ones who showed severe insomnia were treated with Zolpidem.If the patients had tremor and delirium responses during the treatment, they were injected with 100 mg B1vitamin, 0.5 mg B12vitamin with the supportive treatment of 1 mg Clonazepam intravenous infusion and adding Potassium.
2.5 Outcome measures and effectiveness
Two professional clinicians examined the same patients at the end of the second, fourth and sixth week, and scored them independently. Pearson product-moment correlation indicated that the consistency between two raters was good. Scores of PANSS indicated the effectiveness of the treatments on patients. The patients’ blood, urine, liver function, kidney function,blood sugar and ECG were examined regularly, and their adverse reactions were documented during the treatment. Treatment Emergent Symptom Scale was employed to evaluate the effectiveness and adverse reactions, and the results were documented[6].
The methods of rating effectiveness can be referred to the method adopted in the citation[7], and the effectiveness is classified as cured, improved markedly,improved and ineffective. Cured: the reduction rate of PANSS score >= 75%; improved markedly: the reduction rate of PANSS score is between 50% and 74%; improved:the reduction rate of PANSS score is between 25% and 49%; ineffective: the reduction rate of PANSS score< 25%; the total effectiveness = (cured + improved markedly + improved)/n × 100%; the cure rate = (cured/n × 100%). The reduction rate of PANSS score (%) =(the total score before treatment - the total score after treatment)/the total score before treatment × 100%.
2.6 Statistics
SPSS 17.0 software was used to analyze the data.Measurement data were presented as the mean(standard deviation), and independent sample t-tests were employed. Number data were presented as relative number of constituent ratios (%), and χ2 tests were employed. The present study used repeated measures analysis of variance to evaluate the changes of two groups’ PANSS scores after 6 weeks of treatment.It means significant differences when p≤0.05.
3. Results
3.1 Normal information
There were 75 patients in the experimental group(63 males, 12 females). The age range was 18-67, and the average age was 32.8 (17.8). The average years of consuming alcohol was 18.3 (3.9). The course of disease ranged from 3 months to 16 years, and the average course was 2.9 (4.5) years. The PANSS score was 82.62(11.47) after they were admitted into the hospital.There were 73 patients in the control group (66 males, 7 females). The age range was 18-70, and the average age was 37.9 (16.8). The average years of consuming alcohol was 16.4 (4.2). The course of disease ranged from 4.5 months to 13 years, and the average course was 5.8 (1.8)years. The PANSS score was 81.21 (18.16). There were no significant differences between two groups’ gender,course of disease and scores (p>0.05), so they were comparable clinically.
3.2 Comparing PANSS scores of before and after treatment
After two weeks of treatment, patients in both groups had improved, and their PANSS scores were lower than those before being admitted into the hospital. Moreover, the reduction of PANSS score in the experimental group was more obvious than that in the control group. The differences in the scores of positive symptoms, negative symptoms and total scores between two groups were significant. After six weeks of treatment, the experimental group’s patients’ scores in all items of PANSS was lower than those in the control group, and both groups’ scores were better than those before treatment (all p<0.05). Furthermore, the scores after the second week, the forth week and the sixth week were all lower than the baseline score, and the experimental group’s PANSS scores were still lower than the control group’s PANSS scores. The differences were all significant statistically (Table 1).
Table 1. The comparisons of both groups’ PANSS scores before and after treatment (±s, points)
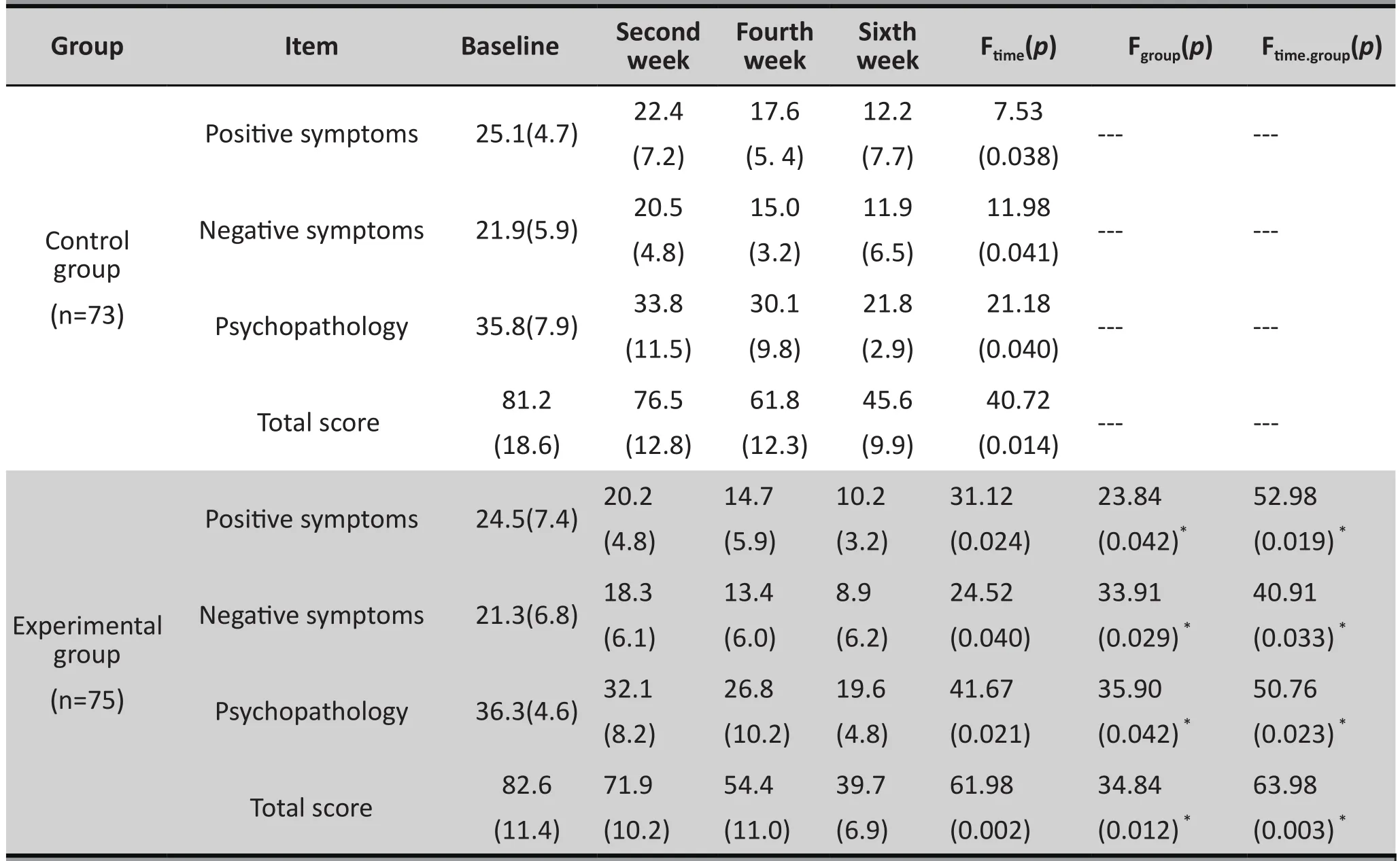
Table 1. The comparisons of both groups’ PANSS scores before and after treatment (±s, points)
* Ftime(p): the results of repeated measure ANOVAs within the experimental and control groups;Fgroup(p) and Ftime.group(p): the between group factor results and between group x time factor results of the repeated measure ANOVAswhich were used to compare the changes of the scores of all items over time between the experimental and control groups.
Group Item Baseline Second week Fourth week Sixth week Ftime(p) Fgroup(p) Ftime.group(p)Positive symptoms 25.1(4.7) 22.4(7.2)17.6(5. 4)12.2(7.7)7.53(0.038) --- ---Control group(n=73)Negative symptoms 21.9(5.9) 20.5(4.8)15.0(3.2)11.9(6.5)11.98(0.041) --- ---Psychopathology 35.8(7.9) 33.8(11.5)30.1(9.8)21.8(2.9)21.18(0.040) --- ---Total score 81.2(18.6)76.5(12.8)61.8(12.3)45.6(9.9)40.72(0.014) --- ---52.98(0.019) *Negative symptoms 21.3(6.8)18.3(6.1)Positive symptoms 24.5(7.4)20.2(4.8)14.7(5.9)10.2(3.2)31.12(0.024)23.84(0.042)*Experimental group(n=75)40.91(0.033) *Psychopathology 36.3(4.6)32.1(8.2)13.4(6.0)8.9(6.2)24.52(0.040)33.91(0.029) *63.98(0.003) *50.76(0.023) *Total score 82.6(11.4)26.8(10.2)19.6(4.8)41.67(0.021)35.90(0.042) *71.9(10.2)54.4(11.0)39.7(6.9)61.98(0.002)34.84(0.012) *
3.3 Comparing effectiveness before and after treatment
After six weeks of treatment, both groups’ patients had clear improvements. The total effectiveness rate of the experimental group was 94.7%, which was obviously higher than that of the control group (90.4%). The cure rate of the experimental group was also clearly higher than that of the control group (24.7%). These two comparisons were both significant statistically (χ2=3.14,p=0.035) (See Figure2 & Table 2).
3.4 The evaluation of the safety
After six weeks of treatment, there was no abnormal results on both groups’ patients’ regular examinations and testing, and there were no patients who dropped out of the treatment. There were 10 patients (13.3%)who showed adverse reactions in the experimental group. The adverse reactions mainly included the loss of appetite, insomnia and so on. There were 14 patients (19.2%) who showed adverse reactions in the control group, and the main symptoms were sleepiness,insomnia, extrapyramidal reaction and so on. After these 24 patients in both groups were treated, their symptoms were improved; and none of them stopped the treatment due to the adverse reactions. Compared to the control group, the experimental group clearly had fewer cases with adverse reactions, and this difference was significant (χ2=6.073, p=0.041) (Table 3).
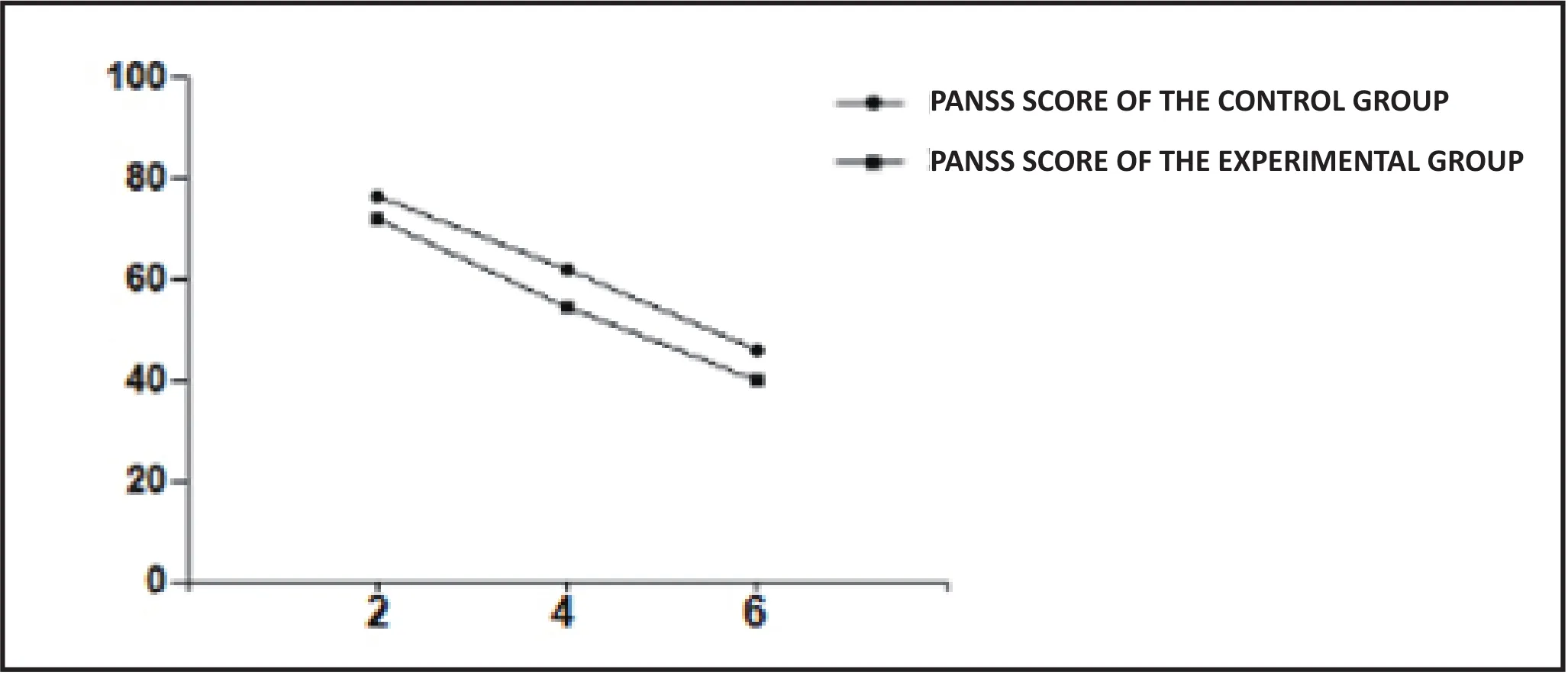
Figure 2. Total PANSS scores comparison between two groups
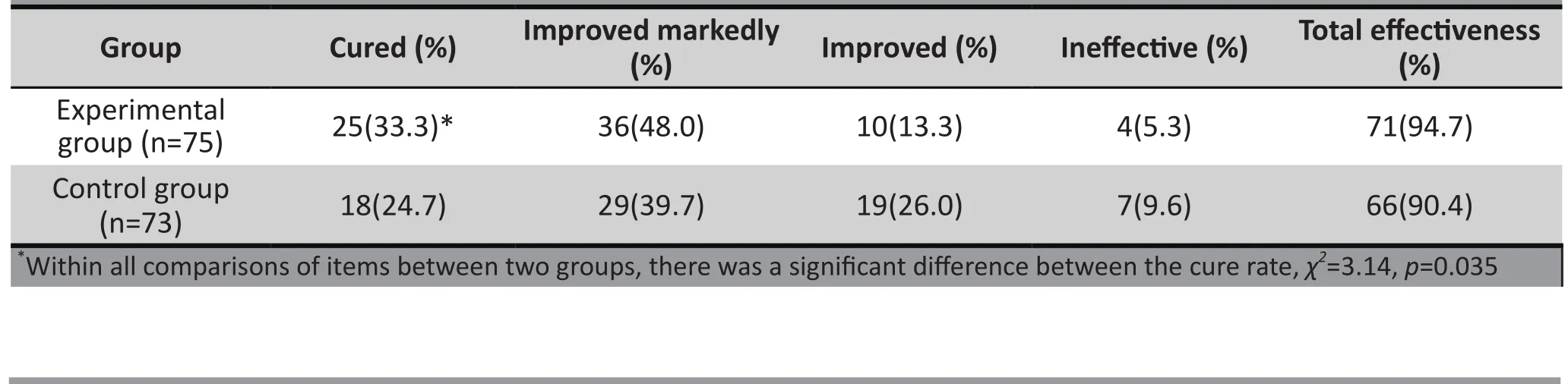
Table 2 The comparisons of the effectiveness of two groups before and after treatment

Table 3 The comparisons of the adverse reaction rate between two groups
4. Discussion
4.1 Main findings
Alcohol-induced mental disorder is a clinically common mental disorder, and its morbidity is increasing. The present study has shown that compared to Risperidone,Quetiapine has better effectiveness on treating patients with this disorder. Quetiapine can lower patients’scores on the positive symptoms, negative symptoms,psychopathology and the total scores within a short period of time, and improve patients’ clinical symptoms.The comparison between these two groups were significantly different. After six weeks of treatment, the cure rate (33.3%) and the total effectiveness rate (94.7%)of the experimental group were higher than those of the control group (24.7%, 90.4%), so the prognoses were satisfying. The rate of the adverse reactions caused by the Quetiapine treatment (13.3%) was lower than that of the control group (19.2%), and this difference was significant statistically. Moreover, the scores after the second week, the fourth week and the sixth week were lower than the baseline score, and the experimental group’s PANSS scores were lower than those of the control group. The differences of all items between two groups were significant statistically.
Psychoactive substances can lead to the strengthening effect of the dopamine midbrain limbic system. Previous studies have shown that almost all the psychoactive substances including alcohol,amphetamines, and opioid drugs can make the dopamine level outside the cells higher than the normal level. Boutros et al. have found that when the psychoactive substance-induced mental disorders last more than six weeks, the mental symptoms are no longer related to the severity of abusing substances simply, but probably related to the pathological changes inside the brain[8]. Alcohol is a kind of neural characteristic friendly substances that can induce anesthetic effect; consuming alcohol in a long term can lead to alcohol abuse, alcohol dependence, alcohol poison and withdraw symptoms, these consequences could impair patients’ physical, mental and social function severely[9]. Currently, the main treatment for alcohol-induced mental disorder is medicine, and atypical antipsychotic drugs can alleviate this kind of mental disorder effectively[10]. But besides the mental disorder, alcohol also affects patients’ physical health,such as extrapyramidal system impairment and so forth; therefore, both treatment effectiveness and drugs’safety should be under consideration[11]. If during the treatment, patients with alcohol-induced mental disorder show tremor, delirium and other symptoms that jeopardize their lives, we need to prevent them from dying with corresponding treatments.
Risperidone is a derivative of benzene, and it is a selective single amine antagonist;it is one of the antipsychotic drugs that are used commonly in China,and it has a relatively good effectiveness on treating psychoactive substance-induced mental disorder[12].But Risperidone’s blocking effect on D2 receptors is relatively strong, and it will lead to extrapyramidal system symptoms such as dysmyotonia, tremor,delirium, relentlessness and so on during the treatment;furthermore, Risperidone and its metabolism can block the D2 receptors on the hypothalamic-funnel pathway, which will lead to hyperprolactinemia[13].Patients could stop taking medication due to the adverse reactions listed above, which leads to bad treatment effectiveness and a relapse. Quetiapine is a kind of atypical antipsychotic drugs that becomes popular recently, and it has interaction with plenty neurotransmitter receptors. It is the antagonist of multiple neurotransmitter receptors in the neural system. Previous studies have shown that it plays its role by blocking 5-HT and DA receptors, and this can improve patients’ positive symptoms in mental system effectively[14,15], which will help alleviate patients’clinical symptoms; in the meantime, studies have also found that Quetiapine can stimulate dopamine’s activity which was in a low excited state, therefore they suggest that it is effective on treating the invisible symptoms and cognition function impairment caused by alcohol[16]. Quetiapine’s affinity to 5-HT receptor is clearly higher than that to DA receptor, so it has less effect on other body parts while it is treating the mental disorder.Therefore, it has less side effects and a higher clinical adaptability, which extends its clinical application range[17].
4.2 Limitations
The present study is a control study with a single center and a relatively small sample size, and the treatment the participants received before they were admitted into the hospital was not considered. Therefore, in order to verify the findings of the present study, the sample size should be expanded and the study design should be stricter. In this study, we increased the dose gradually so that the impairments caused by the medication can be reduced; in the meantime, we also gave the patients a period of time to adjust the drugs.We are able to evaluate the responses of patients with mental disorder to Quetiapine and Risperidone after six weeks of treatment, but we still need more time to explore the safety and the effectiveness of drugs and their effectiveness on preventing mental disorders from relapsing. During the treatment, clinicians evaluated the adverse reactions in every clinical interview, but no standardized assessment tools were used to quantize the severity of complications. Hence, some adverse reactions which were not very severe were overlooked.
4.3 Implication
Even though the present study has a relatively small sample size and a short duration of observation, the clinical results of two groups of patients have still provided amble evidence that supports the following statement: the effect of Quetiapine on treating mental disorder induced by alcohol is better than that of Risperidone, and it can improve the symptoms quickly;moreover, the chance of causing adverse reactions is low, which suggests that it is safe.
Funding
None.
Conflict of interest statement
The authors declared no conflict of interest related to this manuscript.
Informed consent
All participants and their legal guardians provided signed informed consent to participate this study.
Ethics approval
The study was approved by the Ethics Committee of Chongqing San Xia Central Hospital Pinghu Branch.
Author contributions
Bei Lv took the responsibility to write the article, and Haishui Duan was in charge of reviewing the content
Reference
1. Zhornitsky S, Tikàsz A, Rizkallah é, Chiasson JP, Potvin S.Psychopathology in substance use disorder patients with and without substance-induced psychosis. J Addict. 2015;2015: 843762. doi: http://dx.doi.org/10.1155/2015/843762
2. Spriggens L, Hides L. Patterns of cannabis use, psychoticlike experiences and personality styles in young cannabis users. Schizophr Res. 2015; 165(1): 3-8. doi: http://dx.doi.org/10.1016/j.schres.2015.03.023
3. Arroll M A, Wilder L, Neil J. Nutritional interventions for the adjunctive treatment of schizophrenia: a brief review. Nutr J.2014; 13: 91. doi: http://dx.doi.org/10.1186/1475-2891-13-91
4. Chinese Medical Association. [Chinese Classification and Diagnostic Criteria of Mental Disorders (CCMD-3)]. Jinan:Shandong science and technology press; 2001. p: 87-88.Chinese
5. Li JB. [Clinical observation of quetiapine and ziprasidone in the treatment of female schizophrenia]. Zhongguo Ye Jin Gong Ye Yi Xue Za Zhi. 2015; 32(1): 86-87. Chinese
6. Wu Y, Xu W, Liu X.Adjunctive treatment with high frequency repetitive transcranial magnetic stimulation for the behavioral and psychological symptoms of patients with Alzheimer’s disease: a randomized, doubleblind, sham-controlled study. Shanghai Arch Psychiatry.2015; 27(5): 280-288. doi: http://dx.doi.org/10.11919/j.issn.1002-0829.215107
7. Sun D, Jiang QP, Li JF, Li W, Yang LH. [Comparative clinical trial of ziprasidone and risperidone in the treatment of male schizophrenia]. Zhongguo Lin Chuang Yao Li Xue Za Zhi. 2009; 25(3): 204-206. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1001-6821.2009.03.003
8. Sorsdahl K, Sewpaul R, Evans M, Naidoo P, Myers B,Stein DJ. The association between psychological distress,alcohol use and physical non-communicable diseases in a nationally representative sample of South Africans. J Health Psychol. 2016; pii: 1359105316642832. doi: http://dx.doi.org/10.1177/1359105316642832
9. Shen YC. [Psychiatry. 4thedition]. Beijing: People’s Medical Publishing House; 2002. p. 351-352. Chinese
10. Ni XD, Xu HD, Wang ZC. [The situation of the drug treatment on alcohol-caused mental disorders]. Shanghai Arch Psychiatry. 2008; 20(6): 371-373. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1002-0829.2008.06.017
11. van der Weide K, van der Weide J. The influence of the cyp3a4*22 polymorphism and cyp2d6 polymorphisms on serum concentrations of aripiprazole, haloperidol,pimozide, and risperidone in psychiatric patients. J Clin Psychopharmacol. 2015; 35(3): 228 -236. doi: http://dx.doi.org/10.1097/JCP.0000000000000319
12. Chen TX, Yan YY, Bao YY. [Clinical efficacy and safety of ziprasidone and risperidone in the treatment of schizophrenia]. Zhongguo Lin Chuang Yao Li Xue Za Zhi.2015; 31(10): 809-811. Chinese. doi: http://dx.chinadoi.cn/10.13699/j.cnki.1001-6821.2015.10.013
13. Luo HX, Song XQ, Li Y. [A clinical control study of risperidone and risperidone in the treatment of schizophrenia].Zhongguo Xian Dai Yao Wu Ying Yong. 2013; 7(22): 145-146.Chinese
14. Erdogan S. [Quetiapine in substance use disorders, abuse and dependence possibility: a review]. Turk Psikiyatri Derg.2010; 21(2): 167-175. Turkish
15. Huang J, Yuan CM, Fang YR. [Research progress of early diagnosis of bipolar disorder]. Shanghai Jiao Tong Da Xue Xue Bao: Yi Xue Ban. 2011; 31(11): 1550-1553. Chinese. doi: http://dx.chinadoi.cn/10.3969/j.issn.1674-8115.2011.11.010
16. Wang CY. [The application of quetiapine]. Shanghai Arch Psychiatry. 2004; 16(02): 110-112. Chinese
17. Maneeton N, Maneeton B, Woottiluk P, Likhitsathian S,Suttajit S, Boonyanaruthee V, et al. Quetiapine monotherapy in acute treatment of generalized anxiety disorder: a systematic review and meta-analysis of randomized controlled trials. Drug Des Devel Ther. 2016; 10: 259-276.doi: http://dx.doi.org/10.2147/DDDT.S89485

Dr. Bei Lv graduated from Mudanjiang Medical School with a bachelor degree in July 2006. She has been working in the elders’ psychological health department in Chongqing San Xia Central Hospital ever since July 2006. She is the chief doctor currently. Her research interest includes the treatment for mental disorders and the analysis of the effectiveness of relevant antipsychotic drugs.
喹硫平與利培酮治療酒精致精神障礙的療效及安全性對(duì)照研究
呂貝, 段海水
精神障礙;酒精;喹硫平;療效
Background:Compared with Risperidone, Quetiapine’s effectiveness and safety on treating alcohol-induced mental disorder is still unclear.Aim:To investigate the clinical effectiveness and safety of Quetiapine on treating alcohol-induced mental disorder.Methods:One hundred and forty-eight patients with alcohol-induced mental disorderwere divided into the experimental group (75 patients) and the control group (73 patients) by the treatments they received. The patients in the experimental group were treated with Quetiapine by taking it three times per day orally. The average maintenance dose was 151.2(27.3) mg/d, and the treatment cycle was 6 weeks. On the other hand,the patients in the control group received Risperidone once per day orally with the average maintenance dose being 2.3(0.9) mg/d, and the treatment cycle was 6 weeks too. PANSS scale was used to assess patients’prognoses before and after the treatment respectively. The researchers also observed the adverse reactions in both treatment strategies and evaluated the effectiveness and safety of both treatment strategies.Results:The PANSS scale score of the experimental group after two weeks of treatment was 71.9 (10.2),which was clearly better than 82.6 (11.4), the score before treatment; moreover, it was significantly better than the control group’s score (76.5 (12.8)). Also, the experimental group’s scores after 4 weeks of treatment and 6 weeks of treatment were significantly better than the control group. The experimental group’s effective rate (94.7%) was higher than the control group’s (90.4%); the cure rate of the experimental group (33.3%)was obviously higher than that of the control group (24.7%), and the difference was statistically significant.The rates of adverse reactions in the experimental and control groups were 13.3% and 19.2% respectively,and they were significantly different from each other.Conclusions:Treating alcohol-induced mental disorder with Quetiapine is more effective than treating it with Risperidone. Quetiapine can improve patients’ symptoms quickly, and lower the chance of getting adverse reactions. It is effective and safe.
[Shanghai Arch Psychiatry. 2016; 28(4): 204-211.
http://dx.doi.org/10.11919/j.issn.1002-0829.216037]
Elderly Mental Health Department, Chongqing San Xia Central Hospital Pinghu Brunch, Sichuan Province
*correspondence: Haishui Duan, Mailing address: female mental health department, No. 826 Beishan Avenue, Wanzhou District, Chongqing, China.Postcode:404100. E-mail: fvhbjiofgjh@sina.com
背景:與利培酮相比,喹硫平治療酒精所致精神障礙的安全性及有效性尚不明確。目標(biāo)探討喹硫平治療酒精所致精神障礙的臨床療效及安全性。方法:將148例酒精所致精神障礙患者按治療方式分為觀察組75例和對(duì)照組73例,觀察組給予喹硫平治療,每日口服3次,平均維持劑量為151.2(27.3) mg/d,治療周期為6周;對(duì)照組予以利培酮口服治療,每天口服1次,平均維持劑量為2.3(0.9) mg/d,維持治療6周。分別于治療前、后用PANSS量表評(píng)分,評(píng)估患者預(yù)后情況,并觀察兩種療法治療過(guò)程中的不良反應(yīng),評(píng)價(jià)兩種治療方法的安全性和有效性。結(jié)果:觀察組患者治療2周后PANSS量表評(píng)分為71.9(10.2)分,較治療前(82.6 (11.4))分明顯好轉(zhuǎn),且優(yōu)于對(duì)照組的76.5(12.8);治療4周、6周后各項(xiàng)評(píng)分均優(yōu)于對(duì)照組,兩組比較差異有統(tǒng)計(jì)學(xué)意義;觀察組有效率(94.7%)優(yōu)于對(duì)照組(90.4%);痊愈率(33.3%)明顯高于對(duì)照組(24.7%) ,兩組比較差異具有統(tǒng)計(jì)學(xué)意義;觀察組和對(duì)照組患者出現(xiàn)不良反應(yīng)的概率分別為13.3%, 19.2%,兩組比較差異具有統(tǒng)計(jì)學(xué)意義。結(jié)論:喹硫平治療酒精所致精神障礙的效果優(yōu)于利培酮,其可快速改善患者癥狀,且不良反應(yīng)發(fā)生的風(fēng)險(xiǎn)低,是安全有效的。
猜你喜歡
現(xiàn)代儀器與醫(yī)療(2022年2期)2022-08-11 09:51:40
汽車工程師(2021年12期)2022-01-18 06:02:43
建材發(fā)展導(dǎo)向(2021年14期)2021-08-23 00:57:04
建材發(fā)展導(dǎo)向(2021年23期)2021-03-08 01:05:44
裝備制造技術(shù)(2020年4期)2020-12-25 05:25:56
科技傳播(2019年22期)2020-01-14 03:05:32
活力(2019年17期)2019-11-26 00:42:18
基層中醫(yī)藥(2018年6期)2018-08-29 01:20:20
上海農(nóng)業(yè)學(xué)報(bào)(2017年3期)2017-04-10 12:39:18
信息安全與通信保密(2016年3期)2016-08-23 01:23:46
- 上海精神醫(yī)學(xué)的其它文章
- Does more data mean higher efficiency? An experience from pre- and post-treatment study with missing data
- Primary delusion and the sociopolitical milieu in India - A case report & short review
- Malignant syndrome or withdrawal reaction?
- A case report of psychoactive drugs aggravating and alleviating Meige syndrome
- The prospects for the clinical application of exploratory eye movement among patients with psychotic disorders
- Repetitive transcranial magnetic stimulation combined with venlafaxine and lorazepam for treatment of generalized anxiety