
“Thumb’s off” for acrometastasis of renal cell carcinoma:Is there a role for acrometastasectomy in the era of targeted therapy?
2018-09-20 08:07:12
Asian Journal of Urology 2018年3期
Dear Editor,
Malignant tumours of the hand are relatively uncommon.Acrometastasis,defined as metastatic bone lesions of the hand or feet are exceedingly rare,with a reported incidence rate of between 0.007%and 0.2%of all metastatic lesions[1].Acrometastasis of metastatic renal cell carcinoma(mRCC)accounts for only 10%-12%of the reported cases with majority of cases originating from primary lung cancer.The presentation poses a diagnostic and management dilemma and is usually delayed as the symptoms and signs are similar to infective or benign conditions.Typically the prognosis is grim[2,3].In this rarest of rare cases,we report a patient of renal cell carcinoma(RCC)with metastasis to the right shoulder and acrometastasis of the right thumb.We highlight the multidisciplinary team approach utilized and the management by multimodal therapy to achieve the best palliative outcome.
A 52-year-old male had undergone a radical left hemicolectomy with en bloc cytoreductive nephrectomy and adrenalectomy in a private hospital for a metastatic,locally advanced renal tumour with radiological evidence of regional lymph node involvement,lung and liver metastasis(cT4N1M1).Intra-operatively lymph node dissection was not carried out due to the extensive nature of the disease.Histopathological examination(HPE)of the resected specimen was of clear cell renal cell carcinoma(ccRCC)Fuhrman grade 3(pT4NxM1)with involvement of the colon and left adrenal gland.In view of metastasis,he was subsequently started on tablet pazopanib,a tyrosine kinase inhibitor(TKI)used for disease control of mRCC,at 800 mg daily.However due to adverse events of hand foot syndrome and hepatotoxicity within a month,the dose was halved to 400 mg daily.
Seven months later he presented to our hospital with complaints of right shoulder pain causing limited range of movement.As there were no prior bone imaging,magnetic resonanceimaging(MRI)oftherighthumeruscomplemented with a computed tomography(CT)angiogram(Fig.1)and a whole body technetium bone scan was done,revealing an expansile lytic lesion at the proximal right humerus with no other bone involvement.A month later an intra-articular wide excision of tumour and cement spacer insertion was done by the orthopaedic team.The HPE con firmed the lesion as clear cell mRCC,Fuhrman grade 3,consistent with the primary tumour.The margins were tumour free and therefore no adjuvant radiotherapy was planned by the team.
His pain was relieved and he was undergoing physiotherapy to gain functionality of the affected joint.Unfortunately in the following month on routine orthopaedic follow-up,patient had complaints of right thumb swelling and pain of 1 week duration;X-ray film showed a lytic destruction of the distal phalanx,suspicious of an acrometastatic lesion(Fig.2).In view of the recent single bone metastasis with no local recurrence,decision was made to proceed with a right thumb interphalyngeal disarticulation.The HPE con firmed it as mRCC acrometastasis,again consistent with the primary tumour.
A surveillance CT thorax,abdomen and pelvis a month laterrevealedamixedresponse.Thoughthelunglesionshad reduced in size,the liver lesions had increased in size with new bone metastasis noted over the right scapular,bilateral pelvic joints,vertebral bodies and enlarging mediastinal,hilar and para-aortic lymph nodes.In view of the overwhelming tumour burden and worsening general condition,hewasnotkeenforfurthertreatment.Hewascounselledfor palliative therapy and was co-managed by the palliative team,who kept him comfortable on multimodal analgesia for bone pain with radiotherapy to the spine for cord compression symptoms secondary to metastatic lesions.Tablet pazopanib was still continued.He succumbed to his disease few months later.His overall survival from time of initialdiagnosisofmRCCanddiagnosisofacrometastasiswas 13 months and 6 months,respectively.
Acrometastases are rare observations.They are generally diagnosed in symptomatic patients with well known history of malignancy and typically represents disseminated preterminal disease,although in 10%of cases,they represent the first sign of occult malignancy[4].RCC acrometastasis to the hand and foot account for a worldwide reported 30 cases and 21 cases respectively[5].Interestingly none of the cases reported shoulder and thumb as metastatic sites in the same patient.To our knowledge,this is the first reported case of mRCC to the shoulder and thumb.
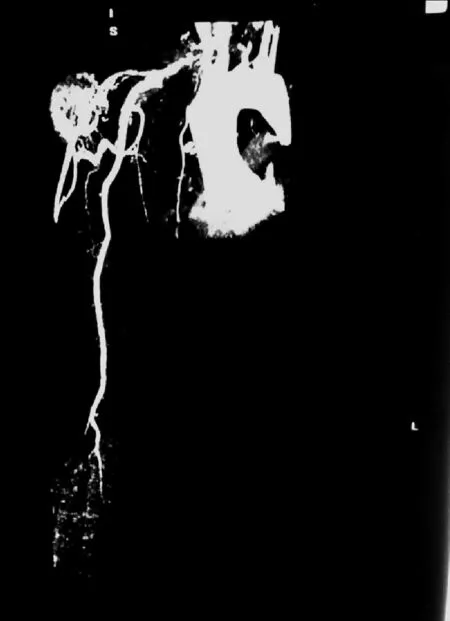
Figure 1 CT angiogram of right upper limb showing metastatic tumour over right humerus 327 mm×451 mm.CT,computed tomography.
Is there a role for acral metastasectomy in the era of targeted therapy?
Metastasectomy is an important component of a bundle care approach known as the sequential multimodal treatment in mRCC.It consists of nephrectomy,metastasectomy and targeted therapy.The inclusion of metastasectomy in this multimodal approach,especially for solitary metachronous lesions has tremendously improved the response rates and progression free survival(PFS)especially in cases oflungmetastasis,wherelungmetastasectomyhad significantly improved 5-year overall survival to 60%[6-8].
Acrometastasis on the other hand,is seen in preterminalpatientswith widespread dissemination and therefore carry grim prognosis.Median survival is 6 months at best.Due to its rarity,there is no standard management protocol that is best tailor managed to the patient.The aim of treatment in this subset of mRCC is palliation.

Figure 2 X-ray film of right hand showing osteolytic changes of right thumb 286 mm×204 mm.
Amputationanddisarticulationarecommonlyperformed for pain relief although conservative management with radiotherapy for immediate pain relief and preservation of normal function has been reported[5,10].
Though our patient was closely followed up,the rapid progression to involve the proximal humerus and then to develop acrometastasis of the thumb was completely unexpected.This could be partly attributed to the suboptimal dosage of pazopanib that was reduced due to the adverse events of the drug.An option that could have been considered was the use of sequential therapy.Sequencing to a different targeted therapy such as the mammalian target of rapamycin(mTOR)inhibitor,everolimus as second line therapy or the newer vascular endothelial growth receptor(VEGFR)kinase inhibitor,axitinib may have proven beneficial,as evidenced by its significant PFS in the AXIS trial[9].
As our patient had limitation of the shoulder joint movement due to pain,irreversible loss of function of the thumb,had good performance status,and patient himself was positive of the outcome;we therefore adhered to the principles of palliative management(adequate tumour resection to achieve disease control,rapid recovery,pain relief,and preservation of hand function at best)[11].Decision was made to limit the disease by multimodal combination of metastasectomy of the humeral lesion followed by acrometastasectomy of the thumb combined with TKI targeted therapy.Though the prognosis remained grim in our patient given his overwhelming tumour burden,the successful surgeries proved beneficial as functionally he had a better quality of life and was pain free before he passed away.Nevertheless he had poor overall survival of 13 months.The survival of 6 months from time of diagnosis of acrometastasis was comparable to the estimated 6-7 months as reported in literature[10].
In conclusion,acrometastasis of mRCC is known to carry a poor prognosis but early multidisciplinary and multimodal approach incorporating nephrectomy,acrometastasectomy and targeted therapy,may prolong survival and improve quality of life.Sequential targeted therapy should be considered in improving PFS,rather than treatment with suboptimal dosing of targeted therapy when faced with adverse events.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2018年3期
Asian Journal of Urology2018年3期
- Asian Journal of Urology的其它文章
- The treatment of complex female urethral pathology
- The choice of surgical approach in the treatment of vesico-vaginal fistulae
- Contemporary diagnostics and treatment options for female stress urinary incontinence
- The aging bladder insights from animal models
- Functional and reconstructive urology(part two)
- The impact of urological resection and reconstruction on patients undergoing cytoreductive surgery(CRS)and hyperthermic intraperitoneal chemotherapy(HIPEC)