The genetic basis of ventricular arrhythmias instructurally normal hearts
2019-07-06 02:52:44
實用心電學雜志 2019年3期
Abstract With the development of research on the pathogenesis of arrhythmia, the role of heredity in the occurrence and development of arrhythmia has been gradually revealed. Genetic screening, family screening, and genetic diagnosis play very important roles in the prevention and treatment of genetic related arrhythmias. This paper summarizes the research progress of such arrhythmias.
[Key words] arrhythmia; ventricular arrhythmia; pathogenesis; primary arrhythmia syndrome; genetic diagnosis; genetic screening; family screening
The arrhythmogenic substrate of familial arrhythmia syndromes is either in the electrical(primary arrhythmia syndromes) or structural characteristics (secondary arrhythmia syndromes) of the heart. This article will focus on primary arrhythmia syndromes. Addressed by Dr. Brugada, primary arrhythmia syndromes include, (ⅰ) long QT syndrome; (ⅱ) Brugada syndrome: ST-segment elevation in right precordial leads, right bundle branch block(RBBB), sudden cardiac death(SCD); (ⅲ) catecholaminergic polymorphic ventricular tachycardia(CPVT) or ventricular fibrillation(VF); (ⅳ) short-coupled torsades de pointes; (ⅴ) short QT syndrome; (ⅵ) isolated conduction disorders(atrioventricular node, bundle branch); (ⅶ) atrial fibrillation/standstill; (ⅷ) idiopathic VF.
With collaborative effort of the Heart Rhythm Society(HRS), the European Heart Rhythm Association(EHRA) and the Asia Pacific Heart Rhythm Society(APHRS), a consensus document was published in 2013 to provide clinical guidance for diagnosis, risk stratification and management of patients with inherited primary arrhythmia syndromes[1]. The endorsed new guidelines listed the following as inherited arrhythmia syndromes: (ⅰ) long QT syndrome, (ⅱ) Brugada syndrome, (ⅲ) CPVT/VF, (ⅳ) short QT syndrome, (ⅴ) early repolarization syndrome(ERS) or idiopathic ventricular fibrillation(IVF), (ⅵ) progressive cardiac conduction disease(PCCD), (ⅶ) sudden infant death syndrome(SIDS) or sudden arrhythmic death syndrome(SADS). The number of genes involved in primary arrhythmia syndromes is quite large. Nowadays, we recognize more than 20 genes involved in Brugada syndrome, 17 in long QT syndrome, 6 in CPVT/VF, 3 in short QT syndrome, 2 in ERS/IVF and 3 in PCCD.
1 The yield of molecular screening
The yield of molecular screening for inherited arrhythmia syndromes was studied by Hofman et al[2]and published in 2013 based on over 15 years of experiences(1996-2010). They found a gene method for predicting and preventing future SCD events in a family. Genetic counselling program was launched in 1996 briefly after the first description of long QT syndromes. According to genetic counselling data from American Medical Center (AMC), the yield of finding a mutation in patients with long QT syndrome is 50%-60%. In this study, the number is 50%. The yield of CPVT is about 40% and Brugada syndrome is about 30%. The yield of molecular diagnosis is clearly associated with family history. The definition of “family history” in this paper was that there is a second individual clearly affected in the same family or suffering from SCD before the age of 40. And then the yield of finding a mutation in those with a positive family history is very high. In patients with long QT syndrome, the probability is over 80%; in individual cases, only 25% have positive results. In patients with Brugada syndrome, it is over 40%vs. 20%. And in CPVT, the proportion is about 75%vs. 20%.
2 Family screening after sudden cardiac death
How often do we find these diseases as causes of sudden death? We investigated 140 families with at least one sudden death before the age of 50. There was no diagnosis on the deceased individuals or family members to start with. We investigated the family members just by routine cardiological examination methods such as ECG, treadmill exercise testing ECG, echocardiogram, blood testing for cholesterol level and magnetic resonance imaging (MRI) if necessary. We revised the available patho-anatomical specimens and did molecular genetic screening[3]. Pathology anatomy was not mandatory. Only half of the deceased individuals had pathology results. The yield of mutation by just analyzing families of the sudden death victims was 33%, which meant one third of the victims had genetic causes traceable on their family members. The cause of death depends on the age of the deceased individuals. When they are very young children between 1 and 14 years old, causes are all primary arrhythmia syndromes; between 15 and 29 years old, some cardiomyopathy pops in and occasionally there is premature coronary artery disease; when they are older between 30 and 49, primary arrhythmia syndromes are still responsible for 2/3 of the cases, but cardiomyopathies and coronary artery diseases also become important causes. Dividing the patients by decades, the yield is extremely high in victims between 1 and 10, and genetic causes were found in 70% of investigated families. The rate drops to 20% in the highest age category.
SADS is a very common cause of SCD with structurally normal hearts which includes all the primary arrhythmia syndromes. In the summary of the literatures[4-10]between 2004 and the very recent years, it accounts for 20%-30% and sometimes even up to 40% of SCD.
It is very important to recognize that autopsy data with uncertain significance should not be considered as cardiomyopathy but primary arrhythmia syndromes. An article published in 2013 by Papadakis et al[11]included 368 SCD victims whose families were referred for cardiac evaluation. There was a group with definite cardiac pathology and another with normal autopsy, but this paper focused on the group with autopsy of uncertain significance(n=41, 12%). Family screening results were positive in 21 out of the 41 victims. Importantly, arrhythmogenic syndrome almost accounted for all of the cases with positive family screening. Specifi-cally, there were 14 cases with Brugada syndrome, four cases with long QT syndrome and one with CPVT. The composition of the group with uncertain autopsy is very similar to that of the cohort with SADS. Therefore, individuals with normal pathology or with uncer tainly significant pathology should be treated in the very same way, so are their family members.
3 Genetic diagnosis for individual diseases
Returning to the primary arrhythmia syndromes list, the related genes have already been discussed by Dr. Brugada. They all affect ion channels in the cell membrane of the heart, including the potassium channel, the sodium channel and the calcium channel. RyR2 receptor and CASQ2 are responsible for CPVT. The Ifchannel is responsible for sick sinus syndrome.
4 Long QT syndrome
Long QT syndrome(LQTS) is autosomal dominant, rarely autosomal recessive and is usually associated with deafness. It is genetically heterogeneous with 17 involved genes(LQTS1-17). Over 60% of the LQTS patients are genotyped. In families, over 90% are genotyped. There are mainly five influenced ion channels, most of which are sodium channels. Three most important types are taken as examples: IKsin LQTS1, IKrin LQTS2 and INain LQTS3. Genetic findings are very important for LQTS diagnosis, risk stratification, treatment choices and life style adjustments.
5 Brugada syndrome
Brugada syndrome type 1 should be considered in a patient with this ECG(Fig.1). Typical Brugada ECG fits these profiles: (ⅰ) with or without drugs; (ⅱ) with precordial leads placed in the 4th intercostal space, or might be higher in 3rd or 2nd intercostal space. A typical Brugada syndrome patient is a 40-year-old male with a family history of nocturnal sudden death; his ECGs may vary from day to day and cardiac events usually occur at rest(but may also occur at exercise). Patients are at risk during fever. And rarely are children with Brugada syndrome reported.
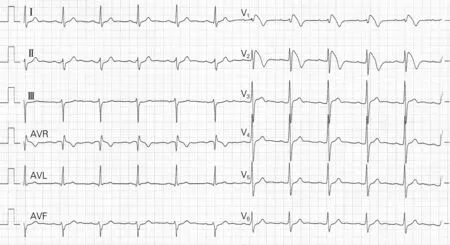
Fig.1 ECG of a 39-year-old male with type 1 Brugada syndrome
The genetic basis of Brugada syndrome is very wide with more than 20 genes involved, and these genes all impact the action potential. But nowadays we regard that onlySCN5Agene which is primarily responsible for phase 0 of the action potential is the major gene involved. All the rest might not be pathogenic in Brugada syndrome itself. In the patients with Brugada syndrome, genetics is not important for the diagnosis. Brugada syndrome is a clinical diagnosis but is not based on the genetics. Genetics may be helpful for risk stratification. There are some evidences showing that certain mutations increase the risk. It is not important for treatment choice but important for life style adjustments.
6 Catecholaminergic ventricular tachycardia/ventricular fibrillation
Catecholaminergic ventricular tachycardia(CPVT)/ventricular fibrillation(VF) is autosomal dominant, genetic heterogeneous(6 genes involved) and triggered by exercise, emotion, etc. It usually starts at young age and importantly, the baseline of ECG is normal. Abnormal ECGs are recorded from those during exercises. Its genetic substrate is in the ryanodine receptor(RyR2) which is located on the sarcoplasmic reticulum and responsible for calcium release into the cytoplasm. When the RyR2 receptor has a mutation, calcium release is increased leading to calcium overload, then delayed after-depolarization, and finally the substrate of CPVT.
However, genetics is not important for the diagnosis of CPVT. CPVT is clinically diagnosed based on the exercise ECG. Genetics is also not important for risk stratification or treatment choice. But it is important for life style adjustments because carriers of a mutation in this gene should be treated with β-blockers.
7 Conclusion
Inherited arrhythmia syndromes are important to recognize because they can be treated very effectively. Genetic testing is mandatory in some cases, particularly in long QT syndromes. And inherent gene specific treatment is particularly carried out on patients with long QT syndrome.
Genetic testing post SCD has significant yield, and significant impact on both family members and therapy choices. It needs a multidisciplinary approach. Geneticists, genetic counselors and sometimes psychologists are required to deal with these patients.