Syncope in a 3-year-old male: A case report
2020-05-18 01:19:28NehaGuptaSaurabhTalathiSarikaKalantre
Neha Gupta, Saurabh Talathi, Sarika Kalantre,
1 Department of Pediatrics, Lincoln Medical Center, Bronx, New York, USA
2 Division of Pediatric Cardiology, Department of Pediatrics, Children's Hospital at Montef ore and Albert Einstein College of Medicine, Bronx, New York, USA
Dear editor,
Syncope is a common presenting complaint in pediatric emergency departments. The differential diagnosis of syncope is vast, including various neurological and cardiac conditions. Brugada syndrome (BrS) is a primary inherited arrhythmia which can present with syncope but can lead to sudden cardiac deaths due to ventricular fi brillation. BrS is a rare genetic condition, often diagnosed in the adulthood. BrS presenting in childhood, especially symptomatic BrS, is extremely rare. We present a case of a previously healthy 3-year-old male who presented to the emergency department with syncope and was later diagnosed with BrS.
CASE
A 3-year-old previo usly healthy boy presented to the emergency department with a chief complaint of passing out. He was playing in his day care when he suddenly fell to the ground and became unconscious. The episode lasted about 2 minutes with regain of consciousness, and there was no associated jerking of extremities, cyanosis, eye rolling, and involuntary passage of stool or urine. His foster mother denied any prodromal symptoms.
His initial vitals were temperature 37 °C, pulse 90 beats/minute, blood pressure 82/50 mmHg and respiratory rate 23/minute. His height and weight were 50thpercentile for his age. Physical examination revealed an alert and cooperative child, with normal neurological exam. Serum glucose was 89. Laboratory evaluation including complete blood count and electrolytes was normal. An electrocardiogram (EKG) revealed a type 2 ST-segment elevation in leads V1-V3, concerning for Brugada-like pattern. Given these EKG findings, his syncope was thought to be secondary to an arrhythmia. Pediatric cardiologist was contacted who recommended a follow-up appointment in pediatric cardiology clinic.
He was followed up in the pediatric cardiology clinic one week later. During his visit, his temperature was 37.6 °C, heart rate 110 beats/minute, respiratory rate 26 breaths/minute, and blood pressure 100/56 mmHg. Physical exam was unremarkable. EKG and echocardiogram during this visit were normal. Foster mother was not sure about his family history for sudden death or deafness. Given previous findings on an EKG and inability to obtain a family history, a procainamide challenge with 10 milligram per kilogram of intravenous procainamide was conducted and the classic EKG fi ndings of BrS were revealed (Figure 1). The patient was then diagnosed with BrS. Genetic testing was positive for SCN5A gene mutation on chromosome 3p21, which is by far the most common genetic mutation in BrS. This missense mutation was associated with substitution of guanine to thiamine base at nucleotide 1052 leading to G351V amino acid substitution and thus reduced current density of inward sodium channels. Due to the presence of symptoms, he underwent implantable cardioverterdefi brillator placement and is currently doing well.
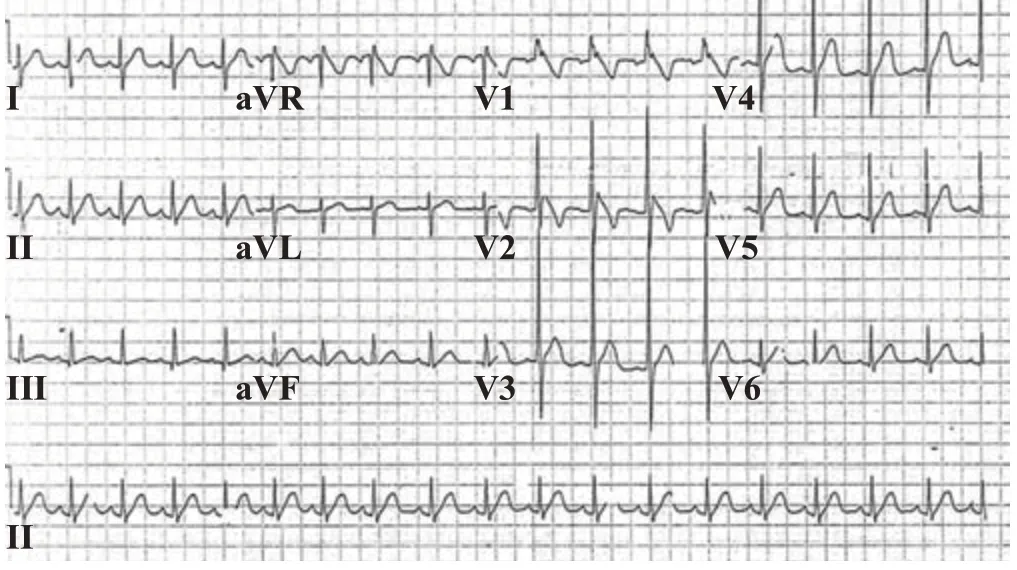
Figure 1. 12 lead electrocardiogram showing the classic features of Brugada syndrome type 1 consisting of ST-segment elevation ≥ 2 mm (0.2 mV), a coved ST-segment followed by a negative T wave in right precordial leads (V1-V2).
DISCUSSION
BrS is an inherited autosomal dominant heart disease with highly variable penetration.[1]It accounts for roughly 4%-12% of all sudden deaths globally. It is a channelopathy marked by inactivation of sodium channels and increase in outward potassium currents.[2,3]Various mutations in the cardiac voltage-gated sodium channels have been identified, the most common being in the SCN5A gene, as seen in our patient, which encodes the alpha subunit of these channels, and is seen in about a third of patients with BrS.[3,4]
Two mechanisms for the pathophysiology of this syndrome have been hypothesized, the repolarization versus the depolarization hypothesis. The repolarization hypothesis suggests that a reduction in sodium channel function in the epicardium leads to an increased transmural voltage gradient, producing an elevated J-wave on the EKG. It can also lead to transmural and epicardial dispersion of repolarization and a phase II reentry leading to ventricular fibrillations. Furthermore, prolonged repolarization leads to T-wave inversion.[5]On the contrary, the depolarization hypothesis suggests that a conduction delay within the right ventricular outflow tract leads to an elevation of ST segment. Further delayed repolarization of right ventricular outfl ow tract is the cause of T wave inversion.[6]
The recently published HRS consensus statement on primary inherited arrhythmias recommends that BrS be diagnosed in patients with EKG findings of type 1 STsegment elevation ≥2 mm in ≥1 right precordial lead.[7]When the diagnosis is unclear as in our patient, sodium or calcium channel blockers to unmask the EKG fi ndings of BrS may be used.[8,9]Our patient presented with a history of syncope with an EKG finding concerning for BrS. However, his repeat EKG in the cardiology clinic was normal. Given his presentation with syncope, lack of family history and previous concerning EKG, we pursued additional testing with sodium blocker, wherein his EKG showed classic Type 1 pattern. Sodium channel blockers, like procainamide, unmask the syndrome by rebalancing the currents at the end of phase 1 of the epicardial action potential.[10]The decrease in the inward sodium current can lead to slowing of the second upstroke of the epicardial action potential and thus, the loss of the right ventricular epicardial action dome as a consequence of all-or-none repolarization. This loss of the dome in right ventricular epicardium but not endocardium creates a transmural voltage gradient that presents as an ST- segment elevation in the right precordial leads on the EKG. A transmural dispersion of refractoriness can lead to the development of phase 2 reentry and ventricular arrhythmias.[10]
Symptoms of BrS vary from asymptomatic to sudden cardiac death.[5]Most common presentations include syncope and seizures followed by nocturnal agonal respiration, mostly because of episodes of ventricular fibrillation.[5,11]Usually, the symptoms appear around the age of 40 years. BrS is very rare in children and often unmasks in the presence of fever. The diagnosis in our patient was at the age of 3 years, and he presented with syncope without any history of febrile illness. This syndrome occurs more commonly and more severely in males, possibly due to the gender distribution of ion channels across the heart and the infl uence of hormones.[11]
Differential diagnosis of syncope is vast, the most common one being vasovagal syncope. This condition should be diagnosed only after all the treatable and life-threatening causes of syncope have been ruled out. Other conditions include electrolyte imbalance, hypotension and cardiac anomalies. When the history is not suggestive of any condition and physical exam is normal, it can be a diagnostic dilemma. It becomes pertinent to do a complete evaluation to rule out any underlying etiology (neurologic or cardiologic) in order to reduce the morbidity and mortality. Syncope needs to be distinguished from a seizure, which can be done by a careful history, for example, abnormal movements with abnormal gaze, loss of bladder or bowel control, tongue biting and post-ictal stage point to the possibility of a seizure. However, many times the episode is unwitnessed, or a proper history is not available. Long QT syndrome has a potential to cause fatal ventricular arrhythmias and should also be in the differential diagnosis. Other causes of syncope are dilated cardiomyopathy, coarctation of aorta, aortic stenosis wherein the syncope is seen after exertion due to reduced systemic blood flow. Any abnormality in EKG needs to be addressed immediately and a cardiologist needs to be consulted.
All symptomatic patients and those asymptomatic ones with inducible ventricular arrhythmias on electrophysiological studies are treated with implantable cardioverter-defi brillator whereas asymptomatic patients are followed periodically. Prognostic factors for this syndrome are previous history of syncope, a spontaneous type 1 EKG pattern and the inducibility of ventricular arrhythmias in electrophysiology study.[12]
CONCLUSION
This case emphasizes that a high index of suspicion for primary inherited arrhythmias is required in children presenting with syncope and additional diagnostic modalities should be considered, especially in those with inadequate family history or abnormal EKG fi ndings.
Funding:None.
Ethical approval:Not needed.
Conflicts of interests:The authors declare that they have no competing interests. The funders had no role in the design, conduct, analysis, or interpretation of data or in writing the manuscript.
Contributors:NG wrote the first draft of this paper. All authors approved the fi nal version.
 World journal of emergency medicine2020年3期
World journal of emergency medicine2020年3期
- World journal of emergency medicine的其它文章
- Information for Readers
- Myalgia may not be associated with severity of coronavirus disease 2019 (COVID-19)
- Do PaCO2 and peripheral venous PCO2 become comparable when the peripheral venous oxygen saturation is above a certain critical value?
- A case of rhabdomyolysis with compartment syndrome in the right upper extremity
- A case of diffuse alveolar hemorrhage following synthetic cathinone inhalation
- Evaluation of gastric lavage eff ciency and utility using a rapid quantitative method in a swine paraquat poisoning model