Validity and reliability of the complementary and integrative health assessment for practitioners scale:CIHAPTR
2021-08-03 05:48:50SadHanerllusmailToygarDeryainar
Nursing Communications 2021年2期
Sad?k Han?erl?o?lu, ?smail Toygar, Derya ?inar
1Internal Medicine Nursing Department, Faculty of Nursing, Ege University, Izmir, Turkey; 2Nursing Department, Faculty of Health Sciences, Bak?r?ay University, Izmir, Turkey.
Abstract Objective:This study aimed to evaluate the validity and reliability of the Complementary and Integrative Health Assessment for Practitioners Scale for Turkish society.Methods: This methodological study was conducted between May ~ June 2020.The participants were 132 health care practitioners including nurses, physicians, dietitians, physiotherapists, and psychologists, who were working in 6 different hospitals, and 4 different provinces in Turkey.Content Validity Index, item scale correlations, confirmatory factor analysis were used to evaluate validity.Cronbach’s alpha and test-retest were used to evaluate reliability.Results: CVI was 0.95 (0.81-0.98).Factor loadings ranged from 0.381 to 0.913 and, item scale correlations ranged from 0.302 to 0.837.The Cronbach’s alpha value was found 0.93 in the current study.Intraclass Correlation Coefficient ranged from 0.82 to 0.96. Conclusion: CIHAP was found to be valid and reliable tool for Turkish society.
Keywords: Complementary and integrative health, Health care practitioners, Validity, Reliability
Introduction
In recent years, the use of Complementary and Integrative Practices (CIP) has increased in global proportions [1].World Health Organization (WHO) reported that 88% of the world population tends to use CIP [2].The 2014-2023 traditional medicine strategy report published by WHO has shown a significant increase in the use of CIP in the past decade.It is estimated that more than 100 million CIP is used in Europe and even more in Asia, Australia, and the USA [3].CIP is the coordination of conventional and complementary approaches.It emphasizes a holistic, patient-focused approach to health care.That health care includes mental, emotional, spiritual, social, and community aspects and treating the person as a whole person [4].CIP can be valuable resources for health promotion, with positive impacts on the daily lives of patients, notably by imposing a new understanding of the health-disease process [5].Although, such positive impacts of the CIP, there are still challenges in their implementation, in their access and use.To overcome these challenges, health care practitioners need to be educated about using CIP.Well, educated health care practitioners play a major role in the dissemination activities of CIP [6].Due to close contact with health care practitioners of patients, they can educate the patients, and facilitate access and use of CIP.Healthcare professionals should explain to their patients about CIP methods, and inform about potential effects and contraindications, and evaluate how they use existing CIP [7].Despite the importance of health care practitioners’ knowledge about usage of CIP and interest in CIP, there is no valid and reliable tool for Turkish society to evaluate their knowledge and interest in integrating CIP into their practices.So, there is a need for developing a scale or adapting a valid and reliable scale to Turkish society.Berger and Johnson (2017) developed the Complementary and Integrative Health Assessment for Practitioners (CIHAP) scale and assessed its validity and reliability.In the United States, they reported the scale as valid and reliable to measure the health care practitioners’ knowledge and interest in integrating CIP into their practices.This scale is an important tool with its unique property of measuring both health care practitioners’ knowledge and interest in integrating CIP into their practices [8].This study aims to evaluate the validity and reliability of the CIHAP in Turkish society.
Methods
This methodological study was carried out between May~June 2020.The inclusion criteria of the study were including to be 18 years and older, work in a hospital for more than six months, and agreeing to participate in the study.In the case of missing values, the participants were excluded from the study.Thirteen of 145 participants were excluded from the study due to missing values and the study was completed with 132 health care practitioners including nurses (n = 61), physicians (n = 29), dietitians (n = 17), physiotherapists (n = 14), and psychologists (n = 11), who were working in 6 different hospitals, and 4 different provinces in Turkey.The participant who could communicate in Turkish were working for more than six months at the profession, and accepted to participate in the study were included.The convenience sample was used for the study.
A Participant Identification Form and CIHAP were used as a data collection form in the study.Online surveys (Google forms) were used for data collection.The link for the surveys sent to the WhatsApp groups of the hospitals.Clicking the link and answering the questions, accepted as a confirmation for the participation in the study.
Participant Identification Form
This form was developed by the researchers.The form included 6 items including age, gender, marital status, education levels, profession, working years in the profession.
Complementary and Integrative Health Assessment for Practitioners Scale (CIHAP)
CIHAP was developed by Berger and Johnson to assess counselors’ and other health-care providers' current knowledge of complementary and integrative health (CIH) and their interest in integrating CIH into their practices.The scale consists of 13 items that utilize 5-point Likert questions.CIHAP contains two subscales, openness to CIH (4,6,7,8,9,10,11) and intentional practices (1,2,3,5,12,13).Items 6 and 11 were coded reversely.Cronbach alpha of scale 0.92 [8].
For the language validation of the scale, steps of WHO guidelines were followed [9].Before starting the validation processes, all necessary permissions were obtained from copyright owners of the scale.The scale was first translated from English to Turkish by the researchers.Subsequently, it was translated from English to Turkish by five independent translators who are fluent in Turkish and English and whose mother tongue is Turkish.As a result of these translations, the most appropriate expressions were determined and the translation of the scale back to English was made by the linguist.The original version of the CIHAP was compared with the translations and appropriate corrections were made following expert opinions.After the final amendments, the translation phases of the scale were completed.
The Turkish version of the form was evaluated by the ten health care practitioners including 3 nurses, 3 physicians, 2 physiotherapists, 1 dietitian, and 1 psychologist.The experts were asked to evaluate the suitability, comprehensibility, and simplicity of each item in the scale.After four panel sessions, the translation process and content validity were completed.The CVI was evaluated for each item (I-CVI) by using the Davis method.
Exploratory Factor Analysis (EFA), Confirmatory Factor Analysis (CFA), and item scale correlations were used to determine to construct validity.Exploratory factor analysis was conducted under original two factor structure of the scale (fixed number of factors).For the assessment of the suitability of data for EFA, Kaiser-Meyer-Olkin and Bartlett’s test of sphericity were evaluated.For the evaluating the model of the CFA, fit indices including the model chi-square, Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), and Standardized Root Mean Square Residual (SRMR) were evaluated before CFA.
In this research, Cronbach’s alpha and test-retest were used to evaluate reliability.For retest analysis, participants choose a nickname for themselves and the forms were reapplied to the 40 health care practitioners after three weeks.It is reported that the number of individuals to be retested should be at least 30 in testing invariance against time [10].
For Cronbach’s alpha reliability coefficient, EFA, and Correlations, IBM SPSS 25.0 (IBM Corp., Armonk, NY, USA) package program was used.For confirmatory factor analysis, AMOS v25 (IBM Corp., Armonk, NY, USA) was used.
Ethical Considerations
To evaluate the validity and reliability of the scale, necessary permissions were obtained from the copyright owner (Berger, C.C.) and the Ethics Committee of Medical Research (Decision no:20-5.1T/60).All directives of the Helsinki Declaration have been followed and informed consent was obtained from the participants.
Results
Of the participants, 66.7% were female, 72% were single, 50.0% were nurse, 62.9% had bachelor’s degrees or higher education and 42.4% had been working in the profession for 3-10 years.The mean age of the participants was 29.52 (± 5.50) years (Table 1).
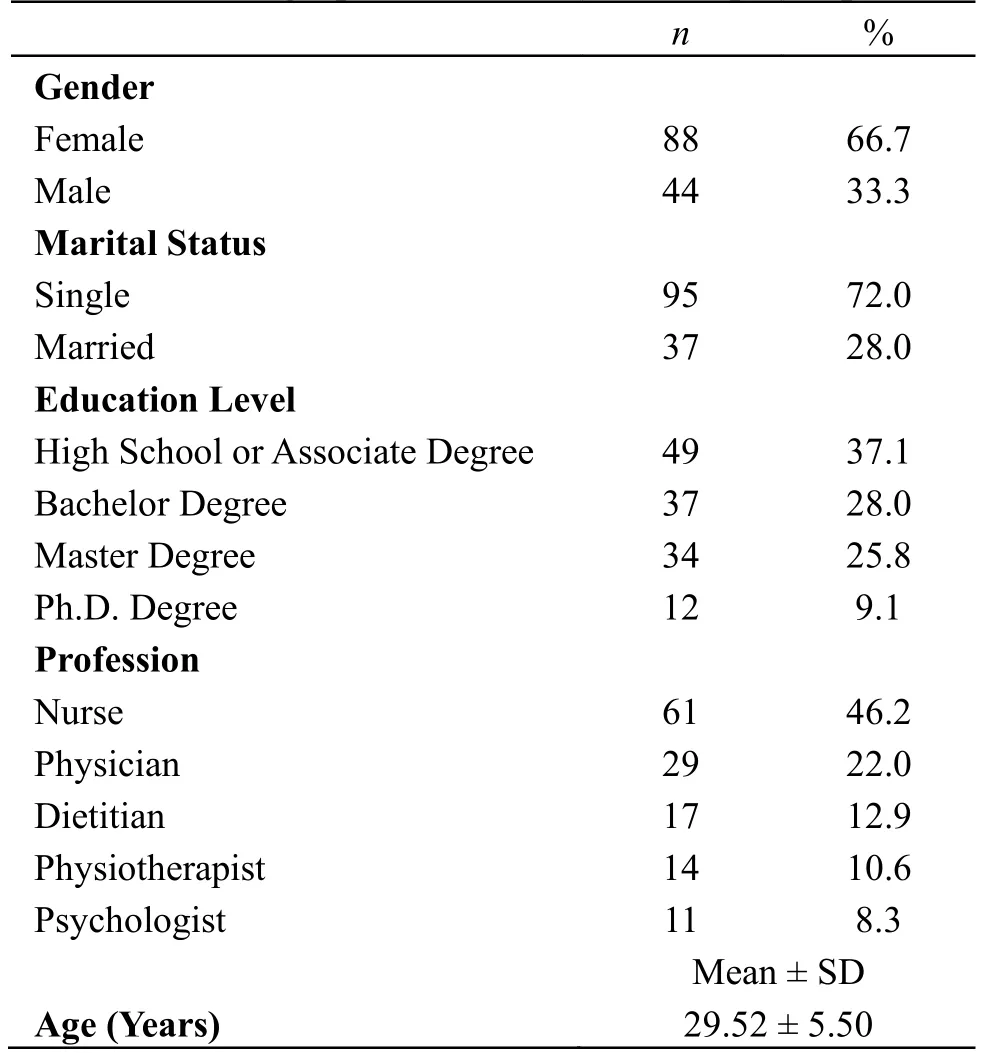
Table 1:Demographic characteristics of participants
After translation of the scale, the CVI of the translated form was calculated.The CVI of the scale was 0.95 (0.81-0.98).The data of the study was found suit for EFA (KMO:0.11, Bartlett’s test of sphericity Chi-square:1282.455,p< 0.001).The scale with its two-factor structure explained 66.41% of total variance according to EFA results.With regard to CFA, factor loadings ranged between 0.044 and 0.914.And, item scale correlations ranged from 0.110 to 0.833.Due to the factor loading and item scale correlation of one item lower than 0.30, we removed that item from the scale and re-asses the CFA and item scale correlations.According to the reassessment of CFA, factor loadings ranged from 0.381 to 0.913 and (Figure 1), item scale correlations ranged from 0.302 to 0.837 (Table 2).
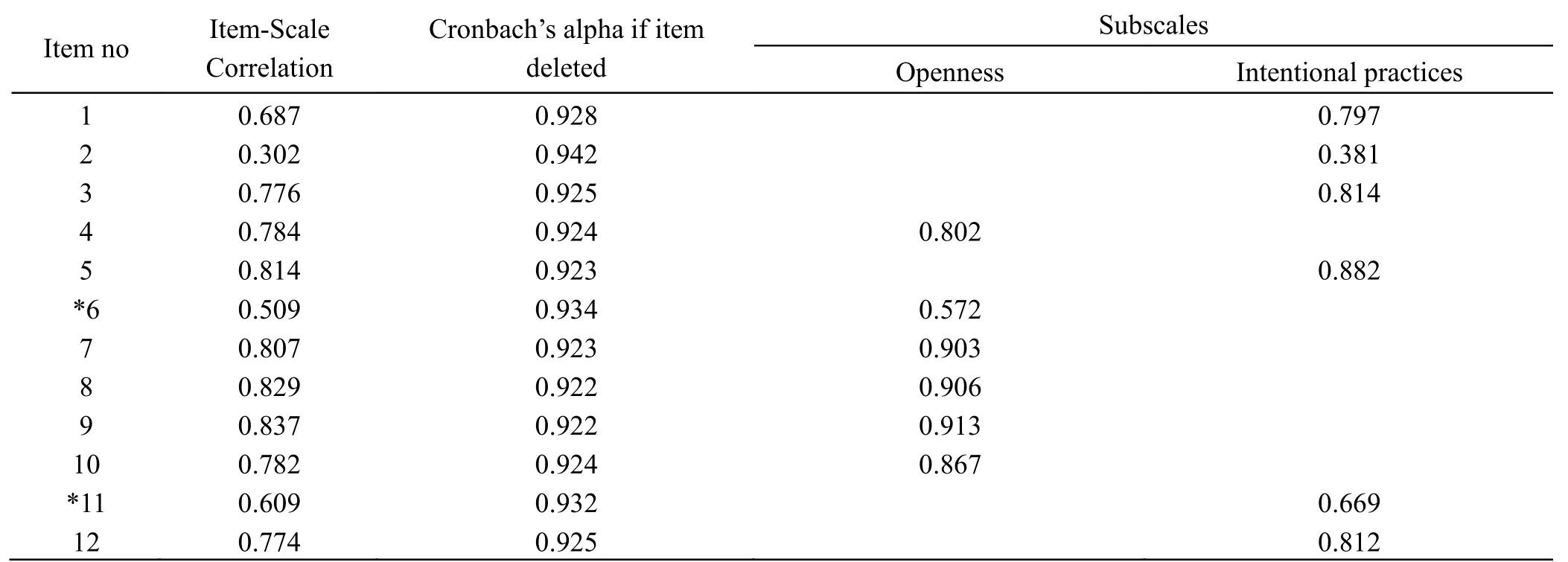
Table 2:Findings on item-scale correlation and CFA
The Cronbach’s alpha value was 0.93 (Table 3).ICC results of the first and second application of the Scale was 0.88 (Table 3).
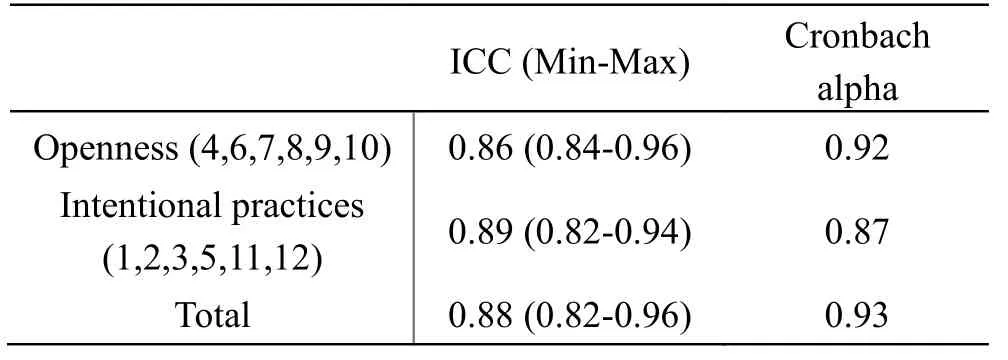
Table 3:Test-Retest and Cronbach alpha reliability of CIHAPTR
Discussion
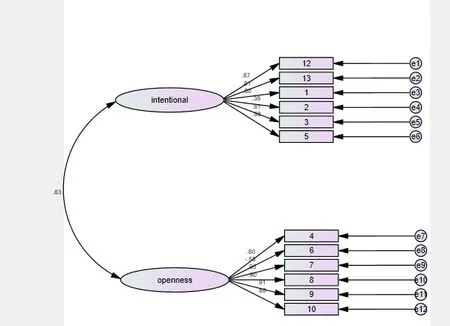
Figure 1:The final structure of the model presented by the CFA diagram
Linguistic validation is the first step in the process called cultural adaptation which has two validation phases:linguistic and psychometric [11-13].The language validation of the scale was done according to the World Health Organization (WHO) guidelines [9].After linguistic validation CVI was calculated.CVI is the degree to which an instrument has an appropriate sample of items for the construct being measured [14].It is reported that CVI should be 0.83 or higher with at least six experts, 0.78 with at least nine experts [15].In our study, 10 experts evaluated the scale, and CVI was 0.95.Concerning the literatüre, CVI was at an acceptable level in our study.To determine the construct of the scale, EFA, CFA, and item scale correlations were used.According to EFA, the scale with its two-factors structure explained the 66.41% of total variance.It was reported in the literature that the structure of the scale should explain more than 50% of the total variance [16].So, we continue to other analysis with the original two-factors structure of the scale.There are fit statistics researchers use to assess whether the data is suitable for confirmatory factor analysis or not.Kline [17] suggests that the model chi-square, Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), and Standardized Root Mean Square Residual (SRMR) should be used for fit analysis.To indicate a good fit, the recommended cut-off values are > 0.05 for p-value, < 0.08 for RMSEA, ≥ 0.90 for CFI, and < 0.08 for SRM.In our study, we determined 0.07 forp-value, 0.06 for RMSEA, 0.92 for CFI, and 0.05 for SRMR.These values are acceptable values for CFA according to literature.In CFA, the item factor loadings ranged between 0.044 and 0.914 under the two-factor structure.Item scale correlations ranged from 0.110 to 0.833.It was reported in the literature that the item with factor loadings and item scale correlation < 0.30 should be excluded from the scale [16].Therefore, we removed the item whose factor loading and item scale correlation were under 0.30.After the exclusion of this item, we re-assessed the factor structure and item scale correlations for construct validity.For this new 12 item version of the scale, results of the fit analyses were acceptable (p> 0.05, RMSEA < 0.08, CFI ≥ 0.90, SRMR < 0.08).Reassessment of CFA showed that factor loadings and item scale correlations were higher than 0.30.So, we conducted the remaining analyses on this 12 items version of the scale.
Cronbach’s alpha is the most widely used internal consistency method.It is a measure of how closely related a set of items are as a group.It ranges from 0 to 1.Higher values are considered more reliable.Values between 0.60-0.79 are considered as very reliable and over 0.80 is highly reliable [18].Cronbach’s alpha of the scale was reported to be 0.92 in a development study [8].We found that the Cronbach’s alpha value of the CIHAP was 0.93 in the current study.This shows that the Cronbach alpha value of the Turkish version of the CIHAP is higher than the original version and highly reliable.
When the same measurement tool is applied to individuals at different times, the similarity and consistency of the responses show the invariance against the time of that measurement tool.Invariance against time is evaluated by test-retest measurements and is one of the most commonly used reliability analyzes [19].In test-retest, intraclass correlation coefficient (ICC) is a widely used reliability index [20].The ICC values range from 0.00 to 1.00, the values between 0.60 and 0.80 accepted as good, and values above 0.80 indicate that an excellent degree of reliability [19].In our study, it was found to be 0.88 (0.82-0.96).This value shows that the test-retest values of the scale indicate that an excellent degree of reliability.
Conclusion
This Turkish version of the scale consists of 12 items that utilize 5-point Likert questions.Scale contain two subscales, openness to CIH (4,6,7,8,9,10) and intentional practices (1,2,3,5,11,12).Item 6 was coded reversely.The scores that can be obtained in the subscales vary from 6 to 30, and the lowest score in the scale is 12 and the highest score is 60 in the scale.
According to the results of all statistical analyzes conducted to evaluate the validity and reliability of the CIHAP, it was concluded that the CIHAP was a high valid and reliable tool for Turkish society.
We recommend using this scale to evaluate the attitudes and perceptions of health care practitioners toward complementary and integrative health.We also recommend evaluating the validity and reliability of the scale for different professions in the health care sector.
The study has some limitations:the study was carried out with 132 health care practitioners including nurses, physicians, dietitians, physiotherapists, and psychologists.So, the results are limited to these professions.
- Nursing Communications的其它文章
- Real experience among undergraduate nursing students in learning the course of geriatric nursing:a qualitative study
- The relationship between academic adjustment and emotional intelligence among undergraduate students in Oman
- An investigation on hand hygiene cognition status and influencing factors of nursing workers in a third-grade a hospital during COVID-19 epidemic
- Analysis on the status quo and influencing factors of fear of disease progress in 120 patients’spouse after bladder cancer surgery