Sequential sagittal alignment changes in the cervical spine after occipitocervical fusion
2022-03-15 07:11:54CeZhuLinNanWangTaiYongChenLiLiMaoXiYangGanJunFengLiMinLiuYueMingSong
World Journal of Clinical Cases 2022年4期
INTRODUCTION
The cervical spine can be classified into two parts:The upper cervical spine (C0-C2) and lower cervical spine (C3–C7).The sagittal alignments of the two parts are closely interrelated[1].An imbalance in the upper and lower cervical regions of the spine can lead to poor cervical sagittal alignment (CSA),which correlates with headache,neck pain,and poor health-related quality of life (HRQOL)[2].
Several studies have explored the interrelationship between upper and lower CSA.Nojiri[1] and Lee[3] observed a significant negative correlation between the C0-2 and C2–7 angles in asymptomatic individuals.Huang[4] found that postoperative kyphosis in the lower cervical spine is associated with hyperlordotic atlantoaxial fusion.Kim[5] reported that anterior cervical discectomy and fusion in the lower cervical spine can induce improvements in regional lordosis at the surgical level and can subsequently cause changes in the upper cervical segment including upward inclinations of the C1 slope and C2 slope.
Occipitocervical fusion (OCF) was first described in 1927 and was suggested to be an effective and safe procedure for the surgical treatment of craniocervical junction disorders (CJDs) caused by congenital deformities,trauma,rheumatoid arthritis (RA),and degenerative processes[6].Matsubayashi[7] found that the occipital to C7 angle (O-C7a) is regulated by the T1 slope and that the corresponding O-C7a is divided into the occipital to C2 angle (O-C2a) and C2–C7 angle (C2-7a),which have negative correlations with each other and then maintain horizontal gaze.Korovessis[8] demonstrated that postoperative O-C2a,pharyngeal inlet angle (PIA),and T1-slope safely predict HRQOL outcomes following OCF for fresh trauma.
The retainer was greatly shocked and grieved at the king s orders, for which he could discover no reason; but, as he had not the heart to destroy three innocent beings, he had a great fire kindled25, and in this he burned a sheep and two lambs, so as to make people believe that he had carried out the king s commands
However,there are few studies regarding sequential changes in the sagittal alignment of the upper and lower cervical regions of the spine after OCF.In addition,to our knowledge,no comparisons of CSA between patients with CJDs and normal populations have been reported.Thus,this study had two purposes:(1) To compare the CSA of patients with craniocervical disorders with that of a normal control population;and (2) To investigate the sequential changes in and interrelationships of the sagittal alignment of the upper and lower cervical regions of the spine after OCF.
MATERIALS AND METHODS
Previous studies have explored the relations between the alignments of the upper and subaxial cervical regions of the spine in asymptomatic volunteers[1,13,14].Nojiri[1] enrolled 313 asymptomatic individuals in their study and investigated the relationships between the alignments of the upper and lower cervical regions of the spine.They observed significant negative correlations between O-C2a and C2-7a and between C1-2a and C2-7a.The correlation coefficient between O-C2a and C2–7a was larger than that between C1–2a and C2–7a.Sherekar[13] also reported that O-C2a was negatively correlated with C2-7a.Guo[14] found that O-C2a was larger in females than in males,whereas C2–7a was significantly larger in males.Both C2–7a and O-C2a correlated significantly with age.In our study,the mean values of O-C2a and C2-7a in the asymptomatic volunteers were 12.0° and 16.2°,respectively,which were comparable with the results of previous studies[1,13,14].A statistically significant negative correlation was also observed between O-C2a and C2-7a in the control group (=-0.385,<0.05).In addition,the average value of O-EAa in the normal controls in this study was comparable to that in the healthy volunteers included in the study by Morizane[15] (92.2°90.0°),who introduced the concept of O-EAa[15].
Patients with CJDs who underwent OCF (OCF group) between April 2010 and May 2019 were included in the study.The inclusion criteria were as follows:(1) Age≥18 years;(2) Surgical treatment with OCF;(3) No history of spine surgery;and (4) At least 1 year of radiographic follow-up data with adequate visualization of the cervical spine on pre-and postoperative films.The exclusion criteria included a history of spine surgery or oropharyngeal surgery,and the presence of preoperative dysphagia,and dysphagia resulting from esophageal disease.For comparison,asymptomatic volunteers with no history of cervical disease or trauma and no neck,shoulder,or arm symptoms were also included in the study as a control group.These people were matched by age and sex with the patients in the OCF group.
All surgical procedures were performed by two senior surgeons from one medical team.We routinely used autologous iliac bones for fusion.The patients in the OCF group were divided into dysphagia and nondysphagia subgroups according to whether they had suffered postoperative dysphagia,as determined by face-to-face questioning or telephone interviews.Patients were defined as having dysphagia if they needed swallowing agents or pureed foods to avoid choking[9].
He took the precaution of surrounding the palace with a dense32 cloud, and then hastened to his Court, where his prolonged absence was causing much anxiety
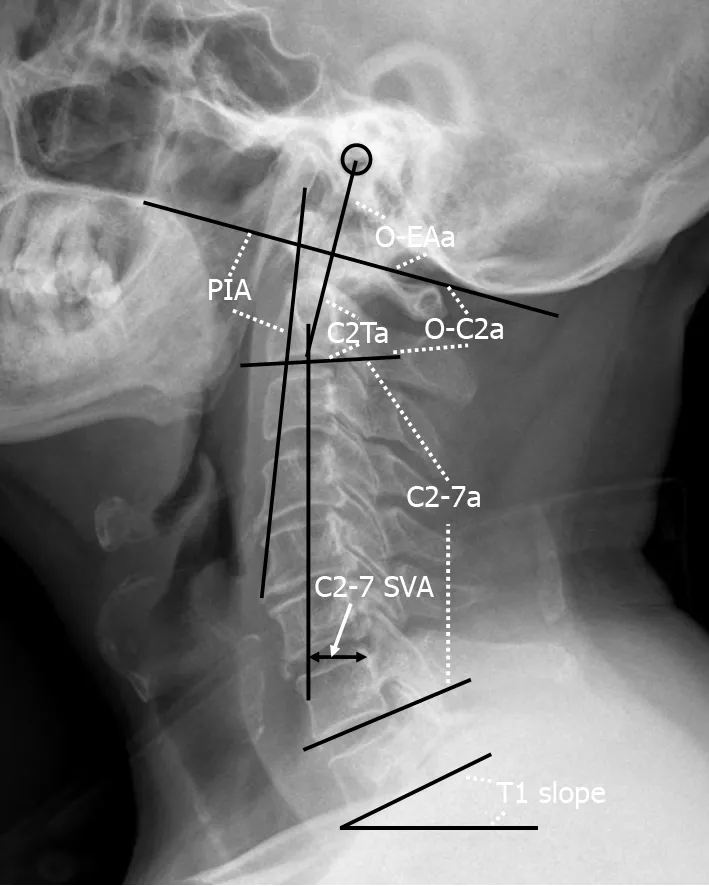
A lateral radiograph of the cervical spine was obtained at baseline,1 mo,and the last follow-up after OCF surgery.The radiographic parameters assessed (Figure 1) were as follows based on previous studies[9-11]:O-C2a,which is the angle between the inferior end plate of C2 and the McGregor line that connects the hard palate and opisthion;the occipital and external acoustic meatus to axis angle (O-EAa),which is the angle formed by the McGregor line and the EA-line and connects the midpoint of the external acoustic meatuses and the midpoint of the inferior endplate of C2;the C2 tilting angle (C2Ta),which is the angle formed by the inferior endplate of C2 and the EA-line;C2-7a,which is the Cobb angle between the lower endplate of C2 and C7;the T1 slope,which is the angle between the horizontal and the T1 superior endplate;the C2-7 sagittal vertical axis (C2-7 SVA),which is the horizontal distance between the C2 plumb line and the posterior corner of C7;and the PIA[10],which is the angle between McGregor line and the line that links the center of the C1 anterior arch and the apex of the cervical sagittal curvature (or bottom when the cervical alignment is kyphotic).Positive values indicated lordosis,while negative values indicated kyphosis.The C2-7 SVA value was considered to be positive if the C2 plumb line was located in front of the posterior upper corner of the C7 vertebral body,and it was considered to be negative if the C2 plumb line was behind the posterior upper corner of the C7 vertebral body[12].To avoid intraobserver bias,all radiological parameters were measured by two attending spinal surgeons who were not involved in the surgery,and the average value of their measurements was used for analysis.
OCF can provide immediate rigidity and fusion in the treatment of CJDs.Although the best result that surgeons expect from OCF surgery is the restoration of normal physiologic occipitocervical alignment in patients,optimal craniocervical alignment has not been confirmed until now.Matsunaga[16] suggested that the position of fixation of the occipital bone and the axis should be within the range of 0-30° according to the O-C2a measurements of 240 healthy volunteers.Inada[17] indicated that excessive O–C2a lordotic correction should be avoided because it might induce a mid-to-lower cervical compensatory decrease in lordosis.Bagley[18] suggested that preoperative halo immobilization before OCF can guarantee physiologic craniocervical neutrality and prevent related complications.This method allows patients to be in a comfortable position when they are awake and allows surgeons to adjust the craniocervical alignment before final fixation and fusion.
RESULTS
A total of 84 patients were included in the OCF group.The average patient age was 50.5 ± 15.0 years,and 45.2% (38/84) of patients were male.CJDs were caused by deformities (=63),trauma (=12),and RA (=9).The fusion levels were O-C2 (=28),O-C3 (=31),O-C4 (=18),and O-C5 (=7).The postoperative follow-up period in the OCF group ranged from 12 to 78 mo (mean,22.8 ± 16.6 mo).
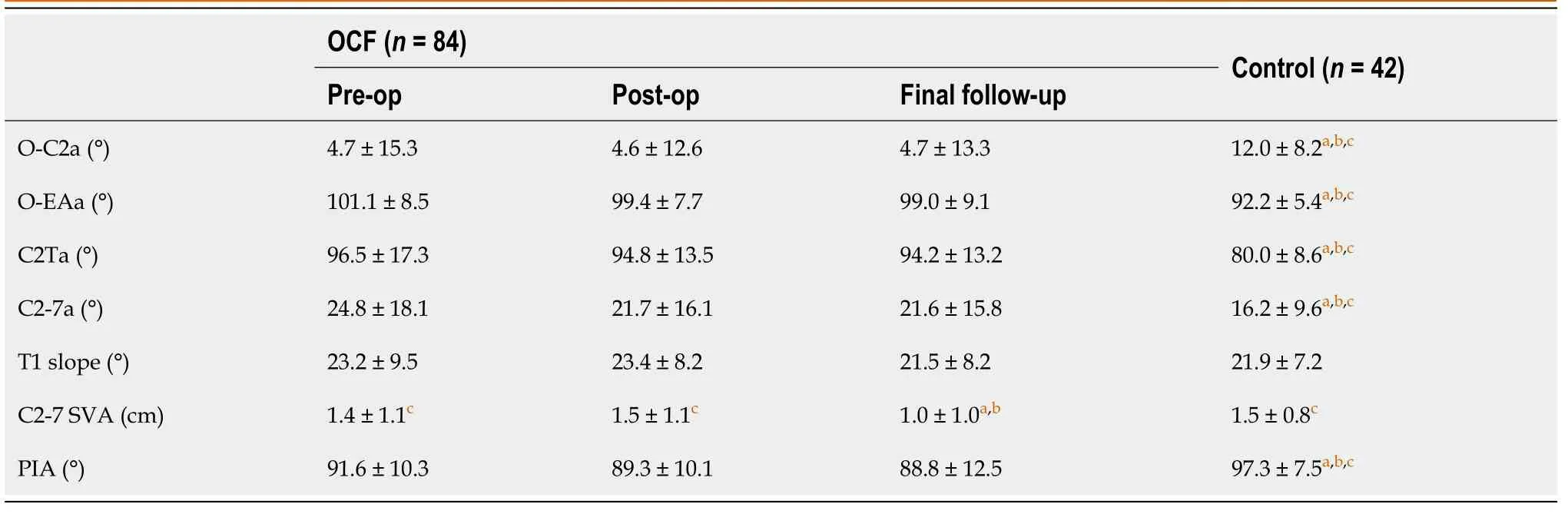
For comparison,42 asymptomatic volunteers were enrolled in the control group.The average age was 51.4 ± 12.4 years,and 47.6% (20/42) of patients were male.The differences in age and sex between the OCF group and control group were not significant (=0.738 and=0.851,respectively).The radiographic parameters in these two groups are listed in Table 1.The O-C2a and PIA of patients in the OCF group were significantly smaller than those of the patients in the control group (<0.05),while the O-EAa,C2Ta,and C2-7a of the OCF patients were significantly larger than those of the normal controls (<0.05).Significant correlations were found between O-C2a and C2Ta (=-0.872),C2-7a (=-0.585),and PIA (=0.757) in the OCF group and between O-C2a and O-EAa (=0.309),C2Ta (=-0.802),C2-7a (=-0.385),C2-7 SVA (=0.331),and PIA (=0.579) in the control group (Table 2).
The Mayoress, a long thin stick of a woman, enraged17 at the insult done to her husband, seized his free arm and tore at it with all her might, with the only result that she too was forced to swell18 the procession
The radiological parameters of patients in the OCF group before surgery,1 mo after surgery,and at the last follow-up after OCF surgery are reported in Table 1.There were no significant differences in O-C2a,C2-7a,or PIA at baseline,1 mo after surgery,or the final follow-up after surgery (>0.05).Compared with the asymptomatic volunteers in the control group,the patients in the OCF group had significantly smaller O-C2a and PIA values after OCF surgery (<0.05) and significantly larger OEAa,C2Ta,and C2-7a values (<0.05).The results of the Pearson’s correlation analysis of O-C2a and the other parameters showed that there were significant correlations between O-C2a and C2Ta (=-0.840,=0.000),C2-7a (=-0.333,=0.002),C2-7 SVA (=0.218,=0.046),and PIA (=0.744,=0.000) at 1 mo after OCF surgery and between O-C2a and-EAa (=0.346,=0.001),C2Ta (r=-0.764,=0.000),C2-7a (=-0.314,=0.004),C2-7 SVA (=0.293,=0.007),and PIA (=0.495,=0.000) at the final follow-up.
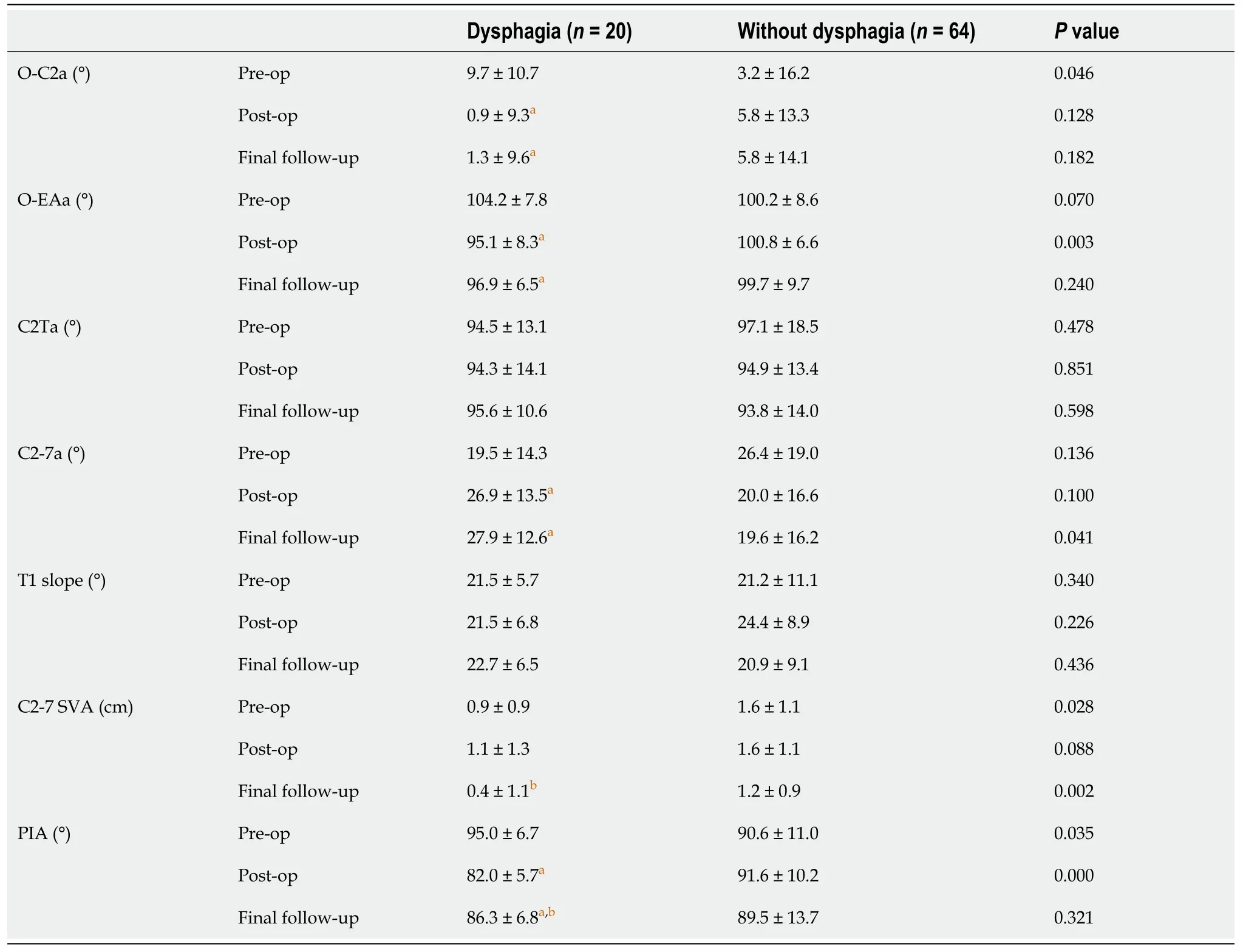
There were 20 patients with dysphagia and 64 patients without dysphagia in the OCF group.No significant intergroup differences were found in terms of age (52.2 ± 12.849.9 ± 15.7,=0.555),fusion level (≤ C3/>C3:16/444/20,=0.405),the proportion of patients with RA (4/206/64,=0.185),or the proportion of patients with AS (13/2040/60,=0.840).However,the proportion of female patients was significantly higher in the patients with dysphagia (16/20) than in the patients without (30/64) (=0.019).The details of the radiological parameters of the patients with and without dysphagia at baseline,1 mo after the surgery,and the final follow-up after OCF surgery are shown in Table 3.

DISCUSSION
This was a retrospective study that was approved by the ethics committee of West China Hospital of Sichuan University and informed consent was obtained from all the patients.All methods were carried out in accordance with relevant guidelines and regulations.
Finally, Susan decided6 that she was ready to try the trip on her own. Monday morning arrived. Before she left, she embraced her husband tightly. Her eyes filled with tears of gratitude7 for his loyalty8, his patience, and his love. She said good-bye and, for the first time, they went their separate ways. Monday, Tuesday, Wednesday, Thursday... Each day on her own went perfectly9, and a wild gaiety() took hold of Susan. She was doing it! She was going to work all by herself!
In the morning the old woman gave him milk and bread for his breakfast, which he ate contentedly41, rejoicing that there was nothing to be gathered, or counted, or cooked, and when he had finished he begged her to tell him who she was
Analyses were performed with SPSS software (version 22.0;IBM Corp.,Armonk,NY,United States).Values are presented as the mean ± SD.Quantitative data were analyzed using the Student’s t test or Mann–Whitneytest,as appropriate.Categorical data were analyzed by thetest or Fisher’s exact test.The relationships between variables were assessed using the Pearson’s correlation test.<0.05 indicated statistical significance.
However,the results of our study showed that there were no significant changes in O-C2a or C2-7a from before to after OCF surgery.The O-C2a of the patients with craniocervical disorders at the last follow-up was still significantly smaller than that of the asymptomatic volunteers,while the C2-7a of those patients was larger.We considered the main reason to be that we focused on decompression,reduction,and fusion for the treatment of craniocervical disorders but neglected the importance of restoring craniocervical sagittal alignment.
The studies regarding sequential changes of cervical sagittal alignment (CSA) after occipitocervical fusion (OCF) were limited.
Then she set to work, cutting out and sewing as best she could, and by the end of six days she had turned it into an elegant robe with a long train and a mantle21
Life whispers in your soul and speaks to your heart. Sometimes,when you don t have the time to listen,it s your choice: Listen to the whispers of your soul or wait for the brick!
Compared to the patients with CJDs,the normal controls had a larger OC2a (12.0°4.7°),while the O-EAa,C2Ta,and C2-7a were smaller (92.2°101.1°,80.0°96.5°,16.2°24.8°,respectively).Based on these results,we speculated that the degree of lordosis of the upper cervical spine was markedly lower in the patients with these disorders because of weaknesses in vertebrae,muscles,and ligaments caused by craniocervical lesions (OC2a↓).Hypolordosis in the upper cervical spine caused the center of gravity of the cranium to move forward (C2Ta↑).Finally,the degree of lordosis of the lower cervical spine increased to compensate for this change (C2-7a↑) so that the individuals could maintain a horizontal gaze and normal C2–7 SVA.
Our study has limitations.Although we found that the O-C2a,C2-7a,and PIA could not be corrected to the normal range by OCF while neglecting craniocervical realignment,we did not find a good method of restoring physiologic occipitocervical alignment in patients with CJDs.To date,there is no consensus on the best method to reestablish occipitocervical sagittal alignment because of its complexity.Many factors should be taken into account to restore optimal alignment,such as the duration of the craniocervical disease,cervical motions in different directions,the influence of the intraoperative position,variations across different techniques,and the impact on adjacent segments[19].Therefore,more studies focusing on the basic biomechanics of the occipitocervical junction,the development of new instrumentations and techniques,and individualized treatment to restore ideal occipitocervical alignment are needed in the future.Moreover,our study was also limited by the retrospective nature and short follow-up period.Therefore,additional prospective studies with more patients and longer follow-up periods are needed to investigate both the clinical and radiographic outcomes of OCF patients.
Previous studies evaluated many factors that might lead to postoperative dysphagia,such as O-C2a,fused segments,age,pathologies,and subaxial cervical positioning[19,21].However,O-C2a was the only significant independent variable correlated with dysphagia.Consequently,operative positioning of O-C2 is the most effective way to avoid postoperative dysphagia.Bagley[18] advocated that preoperative halo immobilization might allow patients to have their head fixed in a particular position and prevent dysphagia.Wang[9] and Meng[11] recommended that surgeons avoid O-C2a reductions greater than 5° during OCF surgery to prevent postoperative dysphagia.Huang and Gonda[21,22] attempted to maintain patients’ head and neck neutrality by an algorithm based on the comparison of pre-and intraoperative X-rays and CT scans.
CONCLUSION
Compared to a normal age-matched control population,patients with CJDs have a more kyphotic upper CSA and a more lordotic lower CSA.The effectiveness of the restoration of CSA provided by OCF surgery may be limited by the realignment of the craniocervical junction being neglected.The reduction in O-C2a after OCF surgery may increase C2-7a and decrease PIA.
ARTICLE HIGHLIGHTS
Research background
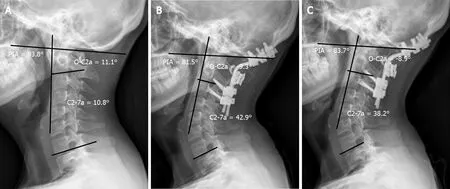
Dysphagia was reported to be one of the most common complications caused by cervical sagittal malalignment after OCF,with an incidence ranging from 9.4% to 26.6%[9,10,19,20].The mechanisms of postoperative dysphagia after OCF remain unclear and are speculated to be multifactorial.In the present study,O-C2a and PIA decreased significantly in the patients with dysphagia from before surgery to 1 mo after surgery,and the effect remained at the final follow-up,while C2-7a increased 1 mo postoperatively and remained the same at the last follow-up.However,the O-C2a,C2-7a,and PIA of the patients without dysphagia were comparable pre-and postoperatively.Pearson’s correlation test showed that postoperative O-C2a values correlated significantly with C2-7a and PIA values.Our results were consistent with those of previous reports describing the relationship between CSA and postoperative dysphagia after OCF[10,19,20].Based on these results,we assume that the mechanism by which postoperative dysphagia is caused by a reduction in O-C2a is as follows:When O-C2a decreases after OCF surgery,the degree of subaxial lordosis (C2-7a) increases to compensate for the decrease in occipitocervical lordosis so that the individual can maintain a horizontal gaze.Then,the apex of cervical spine lordosis protrudes anteriorly (PIA↓),which can compress and narrow the oropharyngeal space directly and lead to dysphagia (Figure 2).
Research motivation
The comprehension of sequential changes of CSA after OCF can help surgeons prevent postoperative complications after OCF.
Research objectives
To compare the CSA of patients with craniocervical junction disorders (CJDs) with that of normal controls and investigate the sequential changes in the CSA of the upper and lower cervical spine after OCF.
Research methods
Radiographic parameters including the occipital to C2 angle (O-C2a),occipital and external acoustic meatus to axis angle (O-EAa),C2–7 angle (C2-7a),and pharyngeal inlet angle (PIA) of the selected patients were measured and compared pre-and postoperatively.
Research results
The O-C2a and PIA of the OCF group were smaller than those of the control group,while their O-EAa and C2-7a values were larger than those of the normal controls.There were significant correlations between the O-C2a and C2Ta,C2-7a,C2-7 sagittal vertical axis (SVA),and PIA at 1 mo after OCF surgery and between O-C2a and OEAa,C2Ta,C2-7a,C2-7 SVA,and PIA at the final follow-up.
A few minutes later he came back and said, I m sorry ma am. Someone made a mistake on the sale tag. It s supposed to be $4,750 for the whole package. I just talked to my Dad who is running the close-out. He said it was worth more than $8,000 regular price so it s still a real good deal.
Research conclusions
Patients with CJDs have a more kyphotic upper CSA and a more lordotic lower CSA than normal controls.The effectiveness of OCF surgery in restoring CSA may be limited by the realignment of the craniocervical junction being neglected.The reduction in O-C2a after OCF surgery may increase C2-7a and decrease PIA.
Research perspectives
This study provides novel insights for sequential changes of CSA after OCF.
We are grateful to Yi Zhu from McMaster University for his kind help in editing the language in this paper.
 World Journal of Clinical Cases2022年4期
World Journal of Clinical Cases2022年4期
- World Journal of Clinical Cases的其它文章
- Surgical treatment of acute cholecystitis in patients with confirmed COVID-19:Ten case reports and review of literature
- Rituximab as a treatment for human immunodeficiency virusassociated nemaline myopathy:What does the literature have to tell us?
- Eustachian tube involvement in a patient with relapsing polychondritis detected by magnetic resonance imaging:A case report
- Endoscopic clipping for the secondary prophylaxis of bleeding gastric varices in a patient with cirrhosis:A case report
- Inflammatory myofibroblastic tumor after breast prosthesis:A case report and literature review
- Langerhans cell histiocytosis presenting as an isolated brain tumour:A case report