Arthroscopic surgery for synovial chondroma of the subacromial bursa with non-traumatic shoulder subluxation complications:Two case reports
2022-03-15 11:59:48XiongFengTangYanGuoQinXianYueShenBoChenYingZhiLi
World Journal of Clinical Cases 2022年5期
lNTRODUCTlON
Synovial chondromatosis is a disease of unknown etiology,originating from the synovium and characterized by the presence of metaplastic cartilaginous nodules in synovial cavities,bursa,or tendon sheaths[1-3].Synovial chondromatosis commonly presents in young to middle-aged men[4],and usually involves large joints,including the knee,hip,and elbow,but can occur in any synovial joint throughout the body.The disease most commonly affects the knee joint,followed by the hip and elbow;however,the occurrence of synovial chondromatosis in either the shoulder or ankle joints is extremely rare[3,5,6].
A diagnosis of synovial chondromatosis is often delayed due to initially mild and nonspecific symptoms[7].If the intra-articular fragments are not adequately calcified,synovial chondromatosis can go undetected for years[8].The complaints associated with synovial chondromatosis typically include joint pain,joint swelling,decreased mobility,and loose bodies[9].However,synovial chondromatosis accompanied by subluxation of the humeral head in the absence of any history of trauma is rare and,to our knowledge,has not yet been reported in the literature,and the mechanism of subluxation has not ever been analyzed.
The most commonly recommended treatment for synovial chondromatosis is the surgical removal of loose bodies to ameliorate the associated symptoms.Currently,an arthroscopic approach is recommended for most shoulder pathologies[10,11].The primary advantages of using arthroscopic approaches include decreased morbidity,synchronous visualization,and the ability to treat both intra- and extra-articular pathologies.Hypertrophic synovia and multiple loose bodies are typical arthroscopic findings[12,13].
In this report,we present two cases of synovial chondromatosis in the shoulder joint accompanied by subluxation of the humeral head treated with arthroscopic management in adult patients and discuss the potential underlying mechanisms involved in disease development.
When the King found the reel at the bottom, he had the Many- furred Creature brought to him, and then he saw the white finger, and the ring which he had put on her hand in the dance
CASE PRESENTATlON
Chief complaints
A 56-year-old woman experienced severe right shoulder pain and decreased range of motion for 3 d without any history of trauma.
A 56-year-old woman experienced severe left shoulder pain with limited mobility for 3 mo,which worsened over the past 4 d,without any history of trauma prior to presence at our hospital.
The patient’s medical history was unremarkable,and she was in generally good health.
History of present illness
Case one:As reported by the patient,the right shoulder pain was accompanied by limited mobility and significant swelling due to slight external force over the previous 3 d.The pain and swelling continued to increase without systemic treatment,and the patient was referred to our hospital for further treatment.After physical examination,imaging examinations,and a review of the patient’s medical history,the patient was diagnosed with right shoulder joint dislocation.
The patient described left shoulder joint pain without an obvious cause and limited joint movement,which started 3 mo prior to presentation.Conservative treatments,such as acupuncture and therapeutic massage at a local hospital,did not provide symptom relief,and the pain had become aggravated over the past 4 d without any trauma.
History of past illness
Is it possible that Prince Featherhead can have parted with it? He would part with his life sooner, lovely Princess, answered he; I can assure you of that, for I am Prince Featherhead
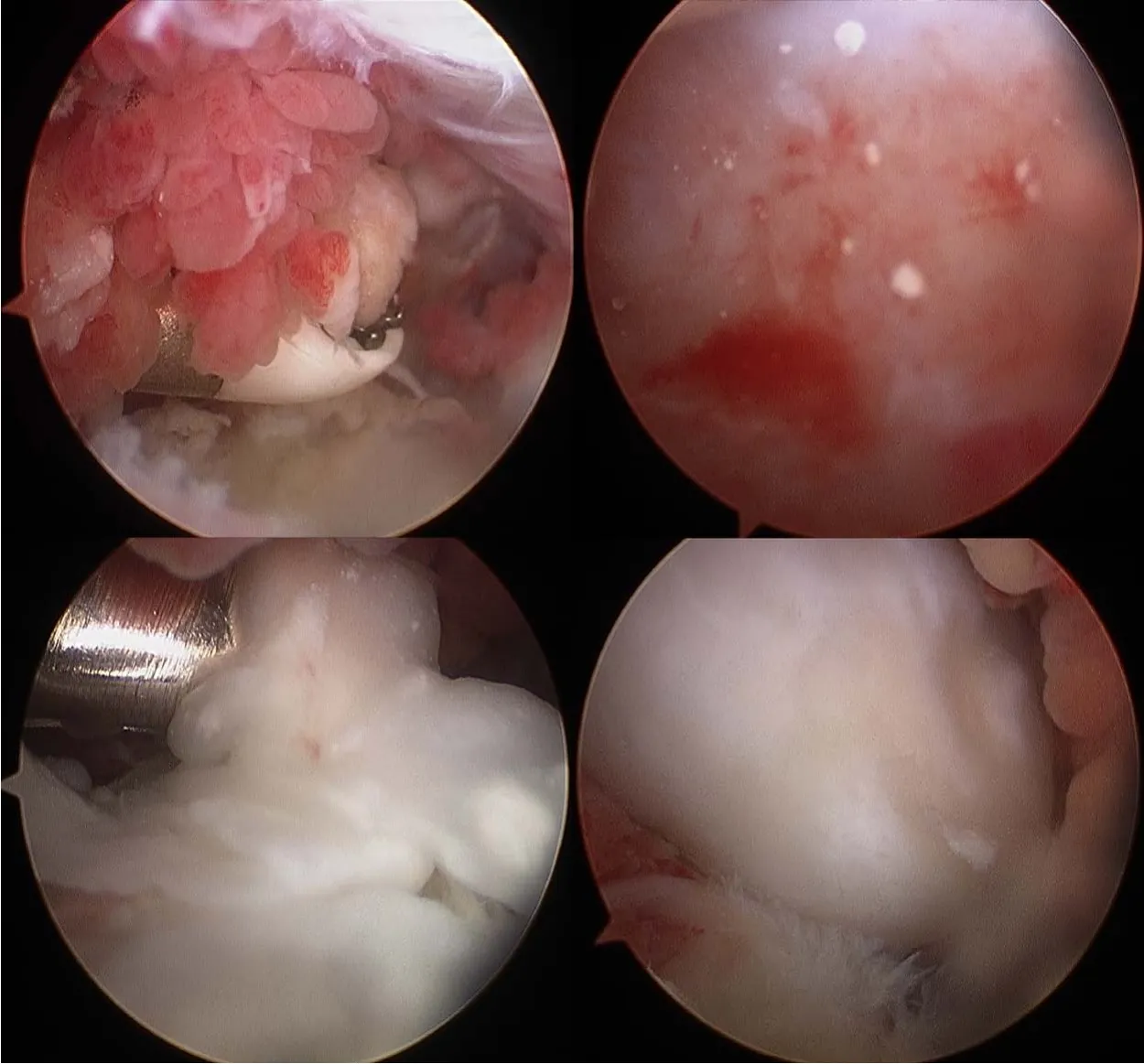
Case one:We performed arthroscopic labrum fixation and removal of the loose body from the shoulder joint.After successful anesthesia induction,the patient was placed in a left-sided lying position,the right limb was placed in an abduction position,and a traction weight of 4 kg was applied.The standard posterior approach was used for glenohumeral arthroscopy,which showed a large quantity of cartilaginous debris in the joint cavity(Figure 6).Arthroscopy revealed a free cartilage sheet,obvious synovial hyperplasia,massive exfoliation of the articular surface of the humeral head,scapular glenoid cartilage,degeneration of the long head of the biceps,an inferior anterior labrum,and separation of the joint capsule from the glenoid.During arthroscopy,both superior and anterior approaches were used to remove all free cartilage and exfoliate the cartilage from the articular head to proliferate the synovium.The anterior inferior joint capsule and labrum were loosened,and 2.9 mm anchors were implanted at the 5:30,4:30,and 3:00 o’clock positions.The anterior inferior joint capsule and labrum were sutured by lifting and repositioning.The humeral head was located in the center of the joint,and the glenoid labrum was reset.The arthroscope was then moved to the subacromial space,which showed large amounts of synovial hyperplasia under the acromion,accompanied by cartilaginous fragments and free loose bodies,the proliferation of the subacromial capsule,and inflammatory changes.The proliferative synovial membrane,cartilage debris,and loose bodies were removed and sent for pathological examination.The joint cavity and subacromial space were washed with a large volume of normal saline.After checking the gauze and instruments,the incision was sutured,and the affected limb was suspended.After hanging and fixation,the operation was complete.
Physical examination
The physical examination revealed obvious swelling in the right shoulder,with an empty glenoid cavity and obvious deformity.Tenderness was detected in the spinous process of the cervical spine and in front of and above the right shoulder.Mobility was limited,and the Dugas sign was positive.
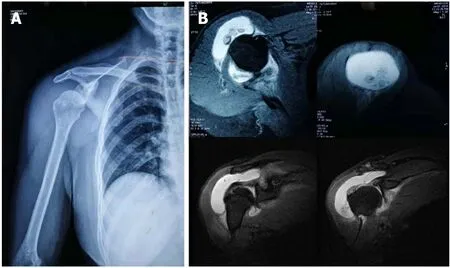
Radiographs showed subluxation of the shoulder joint(Figure 1A).Computed tomography(CT)indicated that the right humerus head was dislocated anteriorly and inferiorly.The joint space was narrowed,the shadow of the surrounding tissue was thick,and the shadow of the fluid density was visible within the joint cavity.A point-striped bone density shadow was observed near the pelvis of the right shoulder.Magnetic resonance imaging(MRI)examination of the shoulder joint indicated a quasi-circular,short T2 weighted signal in the shoulder cavity,with a large area of long T1 and long T2 liquid signals observed in the subacromial bursa(Figure 1B).
Physical examination revealed obvious swelling of the left shoulder joint,mild atrophy of surrounding muscles,positive tenderness in front of and above the left shoulder joint,positive Jobe sign,positive arm drop test,positive pain arc sign,and positive Dugas sign.
Imaging examinations
Sad and lonely do I live like any hermit87 within these walls, avoided by the world and a terror even to animals; the beauties of nature are hidden from me, for I am blind by day, and it is only when the moon sheds her pale light on this spot that the veil falls from my eyes and I can see
So he began to work as a clerk for Tony. We never spoke7 of May anymore and neither of us ever mentioned my theory. But I noticed that Harry always saw every person who came up the stairs.
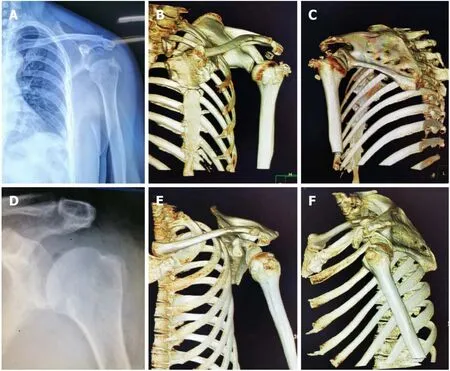
Postoperative radiographic re-examination showed no loose bodies in the subacromial space.The humeral head returned to its normal anatomical relationship(Figure 2D-F).The swelling and pain of the shoulder joint gradually disappeared,and shoulder joint function generally returned to normal.At the 1 mo follow-up,normal shoulder function was restored.
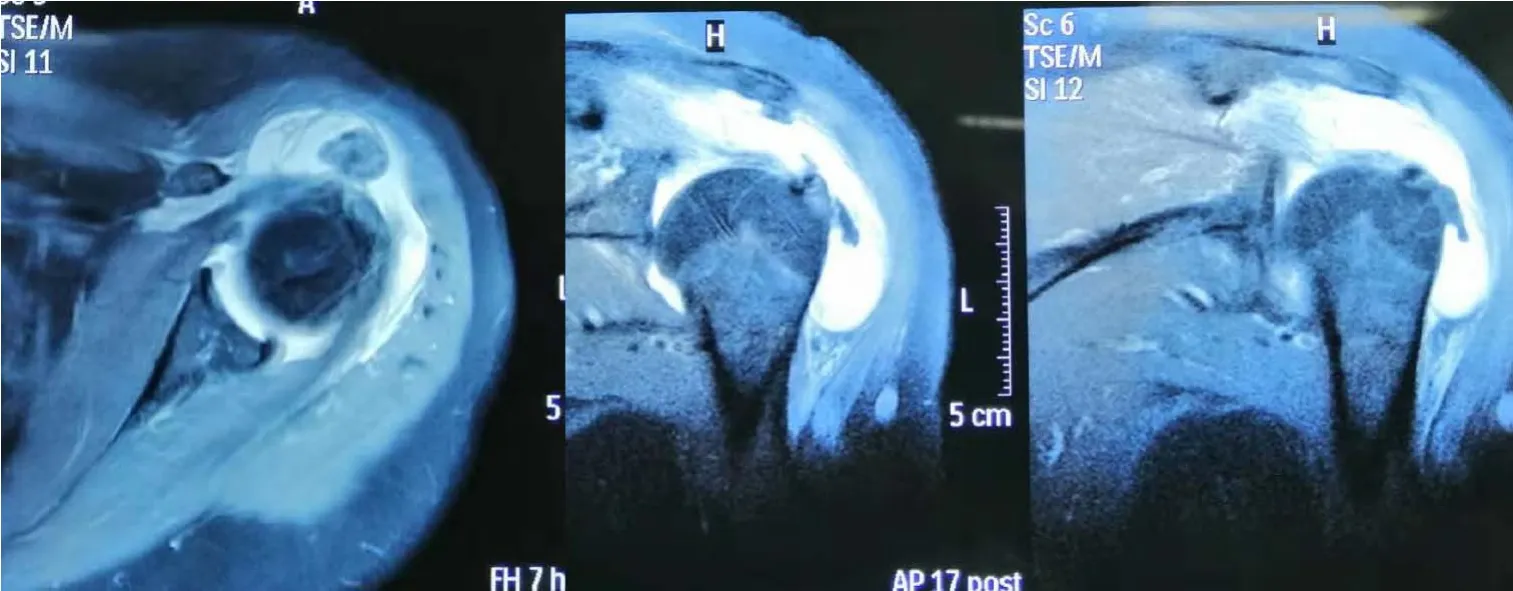
Radiography of the shoulder joint showed a dislocated left shoulder joint and the presence of multiple bone-like loose bodies within the glenohumeral joint space(Figure 2A).On three-dimensional CT,the left humeral head could be observed surrounded by sheet-like,low-density shadows.The CT value was approximately 25 HU,and the surrounding lipolysis remained clear,with multiple sheet-like,bone-like dense shadows visible.The head position was slightly lower than the normal anatomical relationship of the left humerus(Figure 2B and C).MRI examination of the shoulder joint showed a round,short T2-weighted signal,an irregular shape for the supraspinatus muscle,and patchy proton density-weighted image hyperintensity at the attachment point of the supraspinatus tendon in the joint cavity.Sheet-like long T1 and long T2 fluid signals in the subacromial space of the deltoid synovial sac were observed(Figure 3).
Pathological diagnosis
So the tailor gave him some more pebbles, and the bear bit and gnawed10 away as hard as he could, but I need hardly say that he did not succeed in cracking one of them
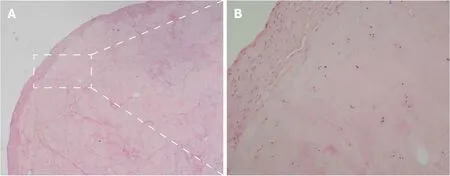
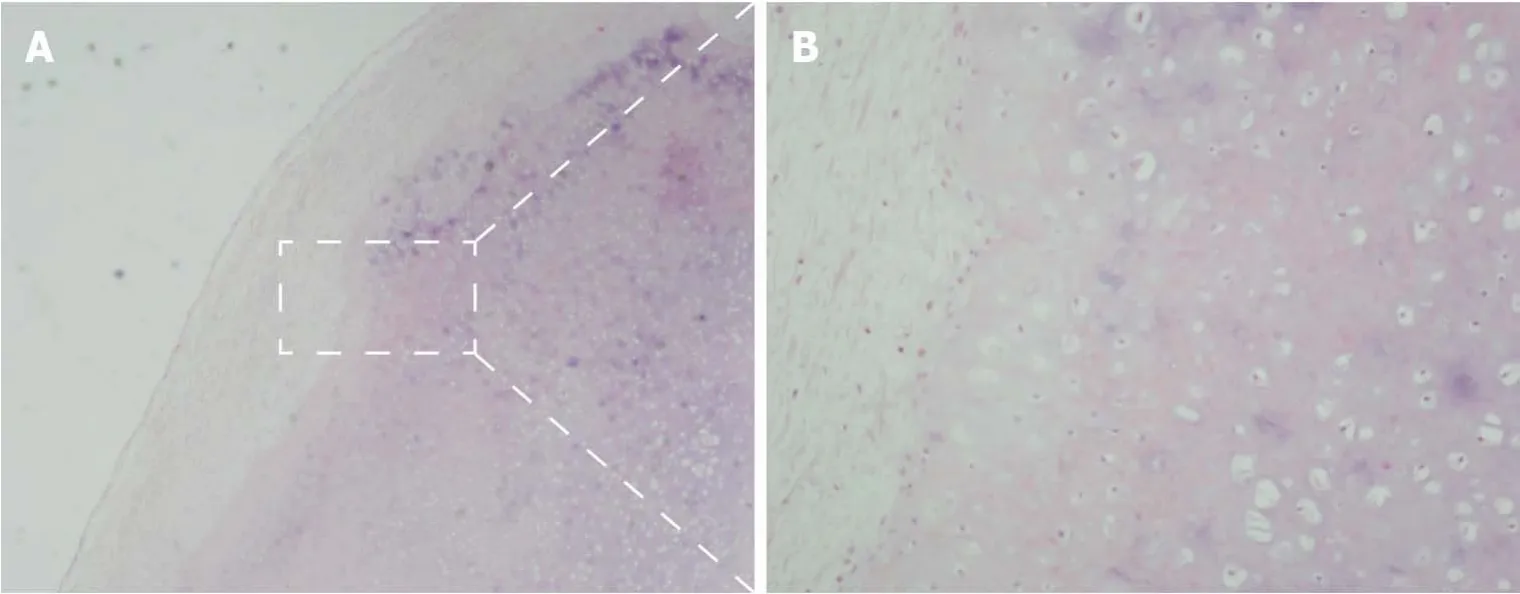
Upon pathological examination,the specimen was identified as a cartilaginous nodule surrounded by fibrous tissue with local calcification.Fragments of articular cartilage or subchondral lamellar bone were observed(Figure 5).

FlNAL DlAGNOSlS
The final diagnosis was subluxation and synovial chondroma of the right shoulder joint.
Subluxation and synovial chondroma,along with calcified tendinitis of the left shoulder joint.
The pathological analysis showed right shoulder joint disease of the synovium and exfoliated cartilage.Hyperplastic cartilage tissue was submitted for inspection,which revealed degenerative local necrosis and ossification in some areas;the subacromial lesion synovium and loose bodies were submitted for inspection as suspected hyperplastic cartilage.The surface of the tissue was covered in a small amount of synovial membrane,consistent with synovial chondroma(Figure 4).
TREATMENT
The patient’s medical history showed a 3-year history of hypertension,reaching as high as 160/100 mmHg,without regular oral antihypertensive medication,resulting in poorly controlled hypertension.
The loose bodies were removed from the shoulder joint under arthroscopic guidance through the following steps.After successful anesthesia induction,the patient was placed in the right decubitus and left limb abduction position,and a traction weight of 4 kg was applied.A standard posterior approach was utilized for glenohumeral arthroscopy after routine disinfection and draping were performed.Under arthroscopic guidance(Figure 7),the synovia of the joints were observed,featuring hyperplasia,with degeneration of the articular surface of the humeral head,scapula,biceps,and long head muscles;intact subscapularis,supraspinatus,and small round muscles;and degenerative lesions detected on the subspinal muscles.Two loose bodies were observed in the joint space,which were removed using nucleus pulposus forceps.An arthroscopic anterior approach was established to remove the synovial hyperplasia.The arthroscope was repositioned to the subacromial space,which revealed the hyperplasia of the outer edge of the front shoulder bone and subacromial bursa and inflammatory changes.After establishing a posterolateral approach,a synovial resection line was determined,and acromioplasty was performed.The joint cavity was washed with a large volume of physiological saline.After checking the gauze and instrument inventory,the incisions were sutured,covered with sterile dressing,and the limb was suspended.
OUTCOME AND FOLLOW-UP
Re-examination by postoperative radiography showed no loose bodies in the subacromial space.The humeral head returned to a normal anatomical relationship.The swelling and pain of the shoulder joint gradually disappeared,and shoulder joint function returned to normal.Range of movement exercises were started as soon as the patient was comfortable.At the 1-mo follow-up,the patient had painfree range of movement in the right shoulder that was comparable to that in the left shoulder,with no remaining preoperative symptoms.
The kingdom was left in the charge of the Prime Minister, who answered Ditto to everything; but the choice was better than it seemed, for the worthy7 man was much beloved by the people, as he agreed with all they said, and they left him feeling very pleased with themselves and their own wisdom
DlSCUSSlON
Synovial chondromatosis of the joints is a rare clinical condition with an unclear definition and diagnostic criteria[14],resulting in limited available knowledge regarding this condition.Synovial chondromatosis can be divided into primary and secondary categories[15].Primary synovial chondromatosis involves no prior basic bone or joint lesions and is generally regarded as a benign neoplastic disease rather than synovial metaplasia,with a reported incidence of approximately 5%[16].By contrast,secondary membrane chondromatosis typically occurs secondary to trauma,osteoarthritis,or rheumatoid arthritis[17,18].Clinically,the signs and symptoms are nonspecific and may be suggestive of several pathological conditions.In most cases,the symptoms comprise pain or range of motion loss.Shoulder pain is one of the first symptoms,followed by the locking of the joint in some cases[18,19].However,dislocation is not a typical feature.Both of our patients experienced a painful range of motion,with signs and symptoms typical of shoulder joint subluxation.
Grannonia, when she learnt that they were talking of her lover, asked at once whose son he was, and if there was any hope of his recovery; to which the fox made answer that the birds had said he was the son of the King of Vallone Grosso, and that the only thing that could cure him was to rub the wounds on his head with the blood of the very birds who had told the tale
Most previously reported investigations have not described synovial chondromatosis accompanied by subluxation,and no previous literature reports have reported any clinical manifestations of joint subluxation;despite the presence of many loose bodies,no cases of joint dislocation have been reported.Koichiretrieved more than 200 loose bodies from a young female patient with a rare condition of secondary synovial chondromatosis in her right shoulder[20].Hiroyuki extracted 17 free bodies from the subscapularis bursa of a confirmed case of synovial chondromatosis in a 12-year-old boy[21].Therefore,we questioned the occurrence of shoulder dislocation in our patients,who were characterized by the presence of relatively few loose bodies.To our knowledge,previous case reports and studies have focused on the characteristic symptoms caused by loose bodies,such as joint pain,swelling,and limited mobility,without examining the biomechanical function of the shoulder joint.The emergence of loose bodies,such as those observed with synovial chondroma in unusual locations,disrupts the stabilization mechanism of the shoulder joint.The lever effect occurs during specific movements,resulting in shoulder joint dislocation.
The biomechanics of the glenohumeral joints depend on interactions between both static and dynamic stabilizing structures[22].Static stabilizers include the bony anatomy,negative intra-articular pressure,glenoid labrum,and the glenohumeral ligaments,along with the joint capsule.The dynamic stabilizing structures include the rotator cuff muscles and other muscular structures surrounding the shoulder joint.The combined functions of these stabilizers serve to support multiple degrees of motion within the glenohumeral joint.When any one of these mechanisms fails,shoulder joint pathology,such as subluxation or dislocation,can occur[22,23].
Whether the observed synovial cartilage tumors observed in our patients represent primary or secondary hyperplasias and the order in which dislocation and synovial chondroma developed are other concerns.Histopathological identification is needed to differentiate between primary and secondary synovial chondromatosis[18].According to Villacin[24],who delineated the histologic criteria for differentiating between primary and secondary synovial chondromatosis,in primary lesions,the chondrometaplasia foci in the synovium and loose bodies are characterized by a markedly disorganized pattern,with many binucleate,plump chondrocytes,and patchy,diffuse calcification.By contrast,in secondary lesions,fragments of articular cartilage or subchondral lamellar bone may be present in the loose bodies,and the pattern of calcification is zonal and ring-like,with uniform,evenly distributed chondrocytes[20,24].Milgram suggested that primary synovial chondromatosis has three phases:(1)Active intrasynovial disease,without loose bodies;(2)transitional lesions,characterized by both active intrasynovial proliferation and loose bodies;and(3)multiple free bodies,without intrasynovial disease[25].Combined with the operative findings of multiple loose bodies and the histologic absence of intrasynovial disease,patient 1 in our case report may have had phase 3 primary synovial chondromatosis,whereas patient 2 may have had a secondary synovial chondromatosis.
Oh, how long have I waited for thee! Never, never must you leave me any more! When the old king heard the news he welcomed him as a son, and made ready a feast, and all the court sat down
The treatment decision is made according to the patient’s age,symptoms,and the disease stage[6].Preventing missed diagnoses and misdiagnoses and performing a differential diagnosis when loose bodies are detected are important concerns,especially when rotator cuff injuries are suspected.The differentiation between a loose body and an avulsion fracture is also necessary.If the intra-articular fragments are not adequately calcified,synovial chondromatosis can go undetected for years[26].Obtaining a detailed medical history and performing complete physical examinations and MRI scans can contribute to the accurate diagnosis and treatment of synovial chondromatosis.
CONCLUSlON
We believe that the biomechanical function of the shoulder joint should be considered,especially when loose bodies are detected,as observed with synovial chondroma occurring in rare sites.Arthroscopic management was successful in two patients with synovial chondromatosis combined with shoulder subluxation.In such conditions,subluxation is usually transient,and the humeral head returns spontaneously to its normal position after the operation.
 World Journal of Clinical Cases2022年5期
World Journal of Clinical Cases2022年5期
- World Journal of Clinical Cases的其它文章
- Subclavian artery stenting via ilateral radial artery access:Four case reports
- Neurothekeoma located in the hallux and axilla:Two case reports
- Diffuse invasive signet ring cell carcinoma in total colorectum caused by ulcerative colitis:A case report and review of literature
- Tacrolimus treatment for relapsing-remitting chronic inflammatory demyelinating polyradiculoneuropathy:Two case reports
- Aseptic abscess in the abdominal wall accompanied by monoclonal gammopathy simulating the local recurrence of rectal cancer:A case report
- Unusual magnetic resonance imaging findings of brain and leptomeningeal metastasis in lung adenocarcinoma:A case report