Convulsive-like movements as the first symptom of basilar artery occlusive brainstem infarction: A case report
2022-06-23 06:27:52TingLingWangGangWuSuZhiLiu
World Journal of Clinical Cases 2022年14期
lNTRODUCTlON
Basilar artery occlusive cerebral infarction (BAOCI) is a rare ischaemic cerebrovascular disease that accounts for approximately 1%-4% of all ischaemic stroke[1]. BAOCI carries high morbidity and mortality. For clinical reference, we report a rare case of basilar artery occlusive pontine infarction with convulsive-like movements at the onset.
CASE PRESENTATlON
Chief complaints
A 55-year-old male patient was sent to our hospital because of unconsciousness and limb convulsion for 1 h.
History of present illness
The patient's wife found him vocalizing in his sleep. He was unconscious and presented with a foaming mouth, limb rigidity and urinary incontinence. Paroxysmal convulsions of both lower limbs were observed. Thirty minutes after admission, the patient regained consciousness but remained unable to speak. His right limb was hemiplegic, and he had paroxysmal involuntary twitches of both lower limbs, with no limb ankylosis. An hour after admission, the patient was able to answer some questions and raise his right limbs. The lower limbs were no longer twitching.
It had pillows of silk, and curtains of silk fringed with gold, and everything that was in the room was of gold or silver, but when she had lain down and put out the light a man came and lay down beside her, and behold3 it was the White Bear, who cast off the form of a beast during the night
History of past illness
The patient had a history of right pontine infarction 3 years prior. The clinical manifestation at that time was mild weakness of the left limbs, and there were no sequelae after treatment.
Personal and family history
The patient's right limb weakness worsened on the 3rd day after admission. Physical examination showed that the proximal muscle strength of the right upper limb was grade III, the distal muscle strength was grade 0, and the muscle strength of the right lower limb was grade III. The patient received antiplatelet therapy, lipid regulation, basilar artery balloon dilatation and rehabilitation.
20.Two pearls: Pearls often symbolize innocence53, purity, faith, wealth, health, salvation54, and self-sacrifice (Olderr 1986).Return to place in story.
Physical examination
The patient did not cooperate with the eye movement examination, and no gaze was observed. Physical examination showed vague speech, bilateral symmetry of the nasolabial grooves, grade IV muscle strength in the right limbs, normal limb muscle tension, and positive bilateral pathological signs.
When it is difficult to distinguish Todd’s paralysis from ischaemic stroke in the early stage, both anterior- and posterior-circulation computed tomography perfusion and vascular examination should be performed as early as possible. More active treatment strategies should be adopted, including thrombolysis and mechanical thrombectomy when necessary.
Laboratory examinations
Studies have shown that the prognosis of BAOCI is related to the location, aetiology, vascular anatomy and collateral circulation[10]. The good prognosis of this patient may be due to the patent status of the posterior communicating artery. Because of severe stenosis of the lower basilar artery, the thrombus moved forward to the upper segment, blocking the opening of the paracentral branch. As a result, an infarction occurred on one side of the pons. Due to the patent status of the posterior communicating artery, the blood supply of the midbrain, cerebellum and other posterior circulation areas was guaranteed. The patient’s prognosis was good.
Imaging examinations
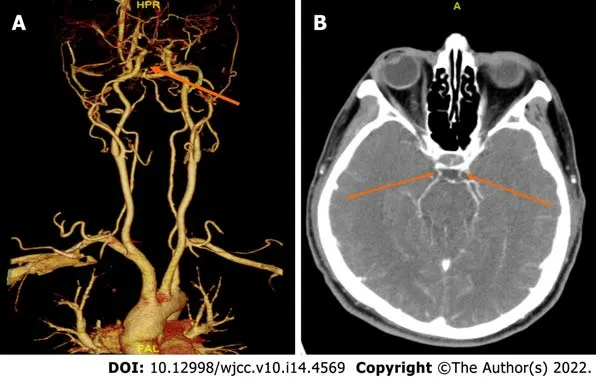
Head computed tomography showed no abnormality. No hypoperfused area was foundcomputed tomography perfusion imaging of the anterior circulation. Computed tomography angiography showed that the basilar artery was occluded and that the posterior communicating artery was patent (Figures 1 and 2). There was no abnormality on video electroencephalogram (EEG) examination during the interictal period. Additionally, 24-h Holter monitoring showed no abnormality.
Further diagnostic work-up
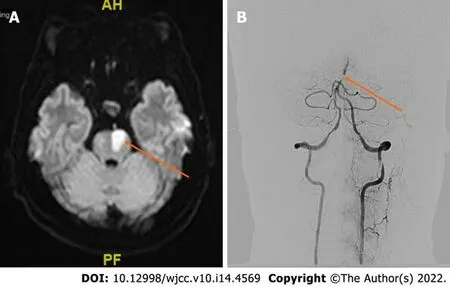
Magnetic resonance imaging revealed left pontine infarction (Figure 2A). Digital subtraction angiography showed that the lower segment of the basilar artery was severely stenosed, the upper segment was occluded, and the bilateral posterior communicating arteries were patent (Figure 2B).
FlNAL DlAGNOSlS
The final diagnosis of the presented case was left pontine infarction and basilar artery occlusion.
TREATMENT
The patient had no personal or family history of epilepsy. Additionally, he had no risk factors for cerebral infarction, such as hypertension, diabetes, smoking, drinking, atrial fibrillation or valvular heart disease.
OUTCOME AND FOLLOW-UP
The fisherman slept well and soundly, for he had done a great deal that day, but his wife could not sleep at all, and turned from one side to another the whole night long, and thought, till she could think no longer, what more she could become
Well, the passengers came up and I had to get busy. I didn t look toward2 the stairs again until nearly time for the 9:18 and I was very surprised to see that the young fellow was still there.
DlSCUSSlON
BAOCI is a rare ischaemic stroke that is life threatening in severe cases. Early diagnosis and treatment can lead to an improved prognosis and an increased survival rate. Therefore, the early diagnosis of basilar artery occlusion (BAO) is very important. However, convulsive movement or epilepsy rarely occurs as the first symptom of BAOCI. A large meta-analysis revealed that the incidence of epilepsy in the early stage of ischaemic stroke was only 3.3%[2]. Studies have shown that cerebral infarction with epilepsy onset mostly occurs in the anterior circulation and cerebral cortex, accounting for approximately three-quarters (75%) of cases. The incidence of posterior circulation infarction is approximately one-quarter (25%)[3].
British Intelligence heard of her arrest. The BBC broadcast the news that the Nazi had put Germany s beloved singer into a concentration camp. This British intervention27 may have helped save her. The Gestapo seemed to lose interest in her, and she slipped away quietly to her grandparents home on a North Sea island, staying there until the war ended.
Convulsive-like movements may be the first symptom of BAO. As early as 1868, there was a description of convulsive movement in brainstem diseases[4]. This phenomenon was often described as epileptic seizure by eyewitnesses, and it was believed to be related to the decerebrate rigidity caused by ischaemia and hypoxia after stroke. Ropper[5] described 8 patients with convulsive-like movements after BAO. They presented with limb rigidity and small-amplitude convulsions. Some patients had limb flexion and large-amplitude convulsions. However, EEG examination during tic-like seizures was not performed. Therefore, it is difficult to judge whether the symptom is an epileptic seizure. Edward[6] reported a case of middle cerebral infarction with BAO. There was no EEG evidence of epileptiform discharge during the patient’s whole-limb twitch and lower-limb twitch. The authors suggested that convulsive-like movements might not be epileptic seizures. However, recently, Bhatt[7] reported a BAO patient with disturbance of consciousness and left limb tonic movement. They found epileptic activity on EEG and recorded the spastic seizure movements of the limb. Therefore, they considered convulsive-like movements to be status epilepticus caused by basilar artery thrombosis.
The mechanism of convulsive-like movements caused by BAO is unclear. Penfield proposed the hypothesis of a centrencephalic system, suggesting that the brainstem was the causative centre of epileptic seizures[8]. It may directly participate in the control of the epileptic threshold through a wide range of forebrain projections. Animal experiments have shown that stimulation of the midbrain, pons or medulla may lead to tonic seizures[4]. Saposnik[4] described a pontine infarction patient with BAO. The patient presented with unconsciousness and convulsions of both upper limbs. However, an EEG showed no cortical discharge. This study suggested that the convulsions may be related to ischaemia of the corticospinal tracts rather than brainstem-originated seizures. Alvarez[9] reported a case of bilateral pontine infarction with ankylosing movement. They held the same opinions as Saposnik. In our case, we could not distinguish whether the convulsive-like movements were secondary to ischemic stroke or caused by epileptic seizures. The patient had no epileptic pathogeny or risk factors for epileptic seizures, such as trauma, tumour, poisoning, infection, metabolic abnormality, or family history of epilepsy. Furthermore, the patient did not undergo EEG examination upon presenting with convulsive-like movements, and no abnormality was observed on EEG during the follow-up treatment. Therefore, we cannot judge whether the phenomenon is epilepsy. However, the patient had basilar artery occlusion, a risk factor for ischemic stroke. We are inclined to believe that the convulsive-like movements were secondary to ischemic stroke.
In our case, the patient presented with epileptic-like symptoms and rapid recovery of limb weakness. The presentation was similar to Todd’s paralysis after seizures. Additionally, the patient seemed to have no other risk factors for cerebral infarction, such as hypertension, diabetes, smoking, or alcohol consumption. Thus, his family members refused thrombolytic therapy. Anterior circulation computed tomography perfusion examination was selected because epilepsy after cerebral infarction is most common in the cortex and anterior circulation. As a result, we failed to identify the cerebral perfusion of the posterior circulation in time. The patient did not receive thrombolysis and thrombectomy. Therefore, when observing convulsive-like movements, clinicians should take the possibility of BAOCI into account.
Routine blood tests, liver function, kidney function, electrolytes, glucose levels and coagulation function were normal.
No, I want to help you, I continued, putting three more shampoo bottles into the cart. The lady peered at me as though I was crazy. Maybe I was, but I knew that I was supposed to help her. She didn t stop me this time so I helped her put away the rest of her items. I was stunned37 by how many people walked by and hopped38 over certain disarrayed39 items in their paths, not even offering a sympathetic word or glance. What astounded40 me even more was when a cute guy whom I had liked for as long as I could remember was one of the uncaring, selfish people who strolled by. I was embarrassed by his reaction when he first saw me in a humiliating situation and then disgusted by his self?centered attitude.
The patient’s muscle strength recovered to grade V. The prognosis was good.
CONCLUSlON
BAOCI is a rare type of ischaemic stroke with high morbidity and mortality. Brainstem infarction with convulsive-like movements as the first symptom is uncommon. When the phenomenon of convulsivelike movements is observed, we should consider the possibility of BAOCI. Early recognition of this phenomenon may reduce the misdiagnosis of BAO and improve the prognosis through early thrombolysis and interventional therapy. If possible, we suggest that an EEG should be performed in time to detect the essential features of the phenomenon.
One day he was in capital spirits because he had made a looking-glass which reflected everything that was good and beautiful in such a way that it dwindled1 almost to nothing, but anything that was bad and ugly stood out very clearly and looked much worse
Then the Baba Yaga sprang up in a fury. Get thee out of my house this moment! she shrieked42. I want no one who bears a blessing to cross my threshold! Get thee gone!
FOOTNOTES
Wang TL collected the clinical data and drafted the initial manuscript; Wu G and Liu SZ revised the article critically; all authors contributed to the intellectual content of this manuscript and approved the final manuscript as submitted.
National Natural Science Foundations of China, No.81903584.
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The authors declare that they have no conflict of interest.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Ting-Ling Wang 0000-0003-4914-0779; Gang Wu 0000-0001-7043-0207; Su-Zhi Liu 0000-0003-1395-4690.
Xing YX
A
Xing YX
 World Journal of Clinical Cases2022年14期
World Journal of Clinical Cases2022年14期
- World Journal of Clinical Cases的其它文章
- Perfectionism and mental health problems: Limitations and directions for future research
- Ovarian growing teratoma syndrome with multiple metastases in the abdominal cavity and liver: A case report
- Development of plasma cell dyscrasias in a patient with chronic myeloid leukemia: A case report
- Suprasellar cistern tuberculoma presenting as unilateral ocular motility disorder and ptosis: A case report
- Rare pattern of Maisonneuve fracture: A case report
- PD-1 inhibitor in combination with fruquintinib therapy for initial unresectable colorectal cancer: A case report