Successful treatment of acute relapse of chronic eosinophilic pneumonia with benralizumab and without corticosteroids: A case report
2022-06-27 08:30:40ShimonIzhakianBarakPertzovDrorRosengartenMordechaiKramer
World Journal of Clinical Cases 2022年18期
lNTRODUCTlON
Chronic eosinophilic pneumonia (CEP) is an inflammatory lung disease, clinically characterized by isolated pulmonary involvement, with appearance of pulmonary eosinophilic infiltrates[1] that permeate the lungs, presenting symptoms include cough, fever and dyspnea[2]. Response to oral corticosteroids (OCS), the commonly administered treatment for CEP, is usually dramatic and rapid[3].However, in approximately 50% of the patients, CEP relapses under tapering of OCS, and thus longterm OCS administration is required[3]. Unfortunately, chronic OCS treatment has a proven increased risk for treatment-related adverse effects and complications, (
hypertension, diabetes mellitus,osteoporosis and infections)[4]. Therefore, the dire need to develop new treatments for patients with CEP, who are dependent on, or resistant to OCS has led to exploring novel therapies. Benralizumab, an IL-5Rα antagonist has demonstrated rapid anti-eosinophil action in patients with asthma. Successful treatment with benralizumab, was also recently reported in three patients with acute relapse of CEP[5-7]. We herein describe an additional patient with an acute relapse of CEP who was successfully treated with benralizumab alone, without corticosteroids.
CASE PRESENTATlON
Chief complaints
On July 26, 2020, a 31-year-old non-smoking healthy woman was evaluated in our hospital. She presented with a 3-wk history of shortness of breath, dry cough and fever up to 38.3 °C.
History of present illness
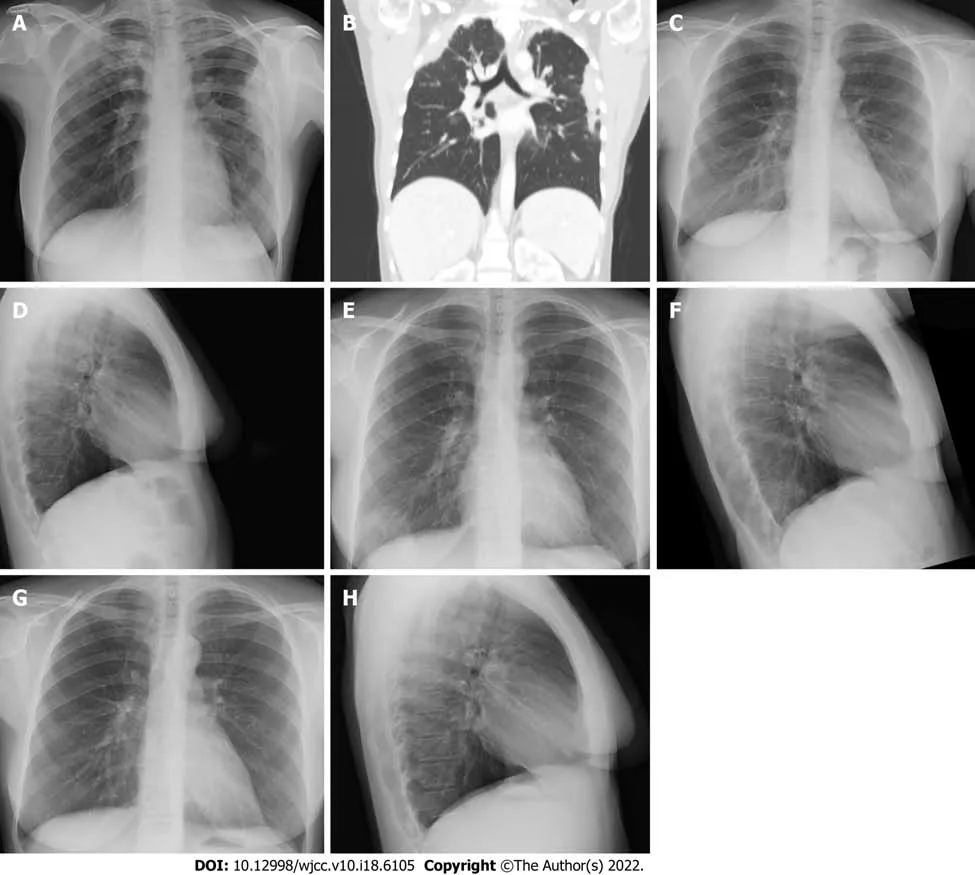
Two weeks prior to the presentation at our medical center, the patient was examined at a local emergency department for the same complaints, which had then appeared for one week. At that time, a chest X-ray showed infiltrates in the right upper and left lateral lung fields (Figure 1A). The laboratory examination revealed mild leukocytosis 11200 K/μL, eosinophilia 800 K/μL and an elevated level of serum C-reactive protein 45 mg/L. Nasopharyngeal swabs were negative for coronavirus disease 2019(COVID-19). She was discharged home from the local hospital with recommendations for oral treatment with cefuroxime 500 mg and roxithromycin 150 mg, both twice daily for 7 days.
The patient was treated with hydrocortisone intravenously at a dosage of 100 mg three times per day,for 2 days, with rapid improvement of dyspnea and cough. The treatment was switched to oral prednisone, at a daily dosage of 40 mg, which was tapered down during the following 2 mo. On September 6, 2020, the patient was feeling well, eosinophilia had resolved, and pulmonary infiltrates no longer appeared on chest X-ray (Figures 1C and D).
History of past illness
社會心理學已經證實,當決策者行動時,常常會考慮他人的判斷和行為,即使知道其他人是一種從眾行為,理性的人也會參與其中并采取類似的行為。如果脫離了大多數,會讓人產生不安全感,尤其是對自己缺乏自信的時候,這種心理效應會更加顯著,即從眾心理。
Physical examination
The patient's temperature was 37.3 °C, heart rate 97 beats per minute, respiratory rate 16 breaths per minute, blood pressure 103/71 mmHg and oxygen saturation in room air 97%. On the chest examination, crepitation was detected on the left lung base. The rest of the physical examination was unrevealing.
Laboratory examinations
Abnormal laboratory findings included leukocytosis 10240 K/μL and eosinophilia 900 K/μL. Results of other routine blood tests were normal. A screening panel was negative for allergic bronchopulmonary aspergillosis, including
specific immunoglobulin E and
serum precipitant. No antinuclear and anti-neutrophil cytoplasmic antibodies were detected. Serologic tests for
,
,
and
were negative.
Imaging examinations
圖10所示的是圖9中第3個脈搏波的處理示意圖。由于噪聲的影響,該脈搏波的終點幅值高于起點幅值。基線校準后,使得起點與終點的幅度相同。進而進行歸一化處理,在沒有影響波形形狀的情況下擺脫了幅度的隨機波動問題,得到一個波形完整、特征點明顯的脈搏波。歸一化使得幅度和面積參數更加穩定,且時間參數不受任何影響。
FlNAL DlAGNOSlS
Eosinophilic pneumonia was diagnosed based on clinical symptoms, peripheral blood eosinophilia,peripheral lung consolidation on chest CT and prompt response to systemic glucocorticoid therapy.
對樣本提取了采用最大池化的BIF和LBP特征作為對比,圖6是一些錯誤識別的結果,第1列是probe測試圖像,第2~6列依次是按相似程度測試圖像在gallery集中選擇的圖像,rank 1表示相似度最高。紅色邊框標記的是正確的識別結果。
TREATMENT
2.1.1適用條件東北黑土區各種類型侵蝕溝均適用,特別適合來水量較大、溝道比降較大、溝道較深、侵蝕嚴重的發展型中型侵蝕溝。
OUTCOME AND FOLLOW-UP
On December 6, 2020, the patient was reevaluated, due to recurrence of dyspnea, cough and fever.Laboratory examination demonstrated blood eosinophilia 600 K/μL, white blood cells 8.8 k/micL and C-reactive protein 0.2 mg/dL. Chest X-ray revealed a new infiltrate in the right lower lobe of the frontal view (Figure 1E), which was clearer in the lateral view (Figure 1F). Acute relapse of CEP was diagnosed.We discussed with the patient treatment options, including the advantages and disadvantages of therapy with OCS
anti-interleukin-5 drug, benralizumab. It was decided to start (on December 7,2020) benralizumab subcutaneously, at a dosage of 30 mg monthly, without OCS. Following 2 wk, the patient reported significant improvement of the symptoms. One month after the first injection of benralizumab, eosinophils were zero and WBC 4 k/micL; CRP was not taken. Five weeks after the first injection, a chest X-ray was unrevealing (Figure 1G and H). Two months later, the patient received the second and third injections of benralizumab and demonstrated sustained clinical and radiographic remission of CEP.
DlSCUSSlON
To the best of our knowledge, we present the fourth recent report in the medical literature regarding rapid improvement of acute flare of CEP, following treatment with benralizumab, without OCS. In previous cases, benralizumab therapy was initiated after frequent, acute CEP relapses, or as an alternative after patient refusal to reinitiate OSC, due to treatment-related adverse effects. Isomoto
[5] described a 58-year-old woman with CEP and a history of refractory asthma. She had three flares of her concomitant disease in the preceding year, which necessitated OCS therapy. Only for the fourth flare, her treating physician initiated a different therapy, one injection of benralizumab, which induced remission of her asthma and CEP following 16 wk. Izumo
[6] described a 43-year-old healthy woman who presented with chronic cough. She was diagnosed with CEP and successfully treated with prednisolone. However, her symptoms worsened after prednisolone cessation. Following patient refusal to re-initiation of OCS, due to treatment-related adverse effects, benralizumab treatment was initiated.After 6 mo of benralizumab therapy, sustained remission of CEP was achieved. Yazawa
[7]described a 70-year-old woman with a history of bronchial asthma who had dyspnea and cough for one month, and was diagnosed with CEP. She refused OCS and therefore was treated with benralizumab,which resulted in resolution of symptoms, hypoxemia and lung infiltrates. Moreover, 12 mo benralizumab maintenance treatment without OCS, provided sustained remission of CEP.
No specific history of past illness was reported.
實驗室安全管理制度建立后并沒有得到及時更新修訂,其中有些內容已經無法適應實驗室較快的發展變化,甚至滯后于實驗室的建設發展;一些實驗室“一線”人員認為本部門沒必要建立適用于自己的安全管理制度。這種想法大謬不然,單位的制度主要是針對各類實驗室共性管理方面的規定,為促使實驗室安全隱患更進一步降低,必須從自身實際出發制定適合本實驗室的安全管理制度。
CONCLUSlON
For treatment of CEP, we maintain benralizumab can serve as a reasonable therapy choice for every patient and a good alternative for OCS.
CEP is an idiopathic lung disease that is characterized by isolated pulmonary involvement, with marked eosinophil accumulation in the pulmonary parenchyma[1,2]. Therefore, we maintain benralizumab is a reasonable therapy choice for every patient with CEP. Predominately, due to its dual mechanism of action, benralizumab a humanized monoclonal antibody, as an interleukin-5 receptor α(IL-5Rα) antagonist, neutralizes the pro-eosinophil functions of IL-5R, by binding to its α subunit and by binding to FcγRIIIa receptor expressed by natural killer cells, triggers apoptosis of eosinophils
antibody-dependent cell-mediated cytotoxicity[8]. This therapy is especially important in patients with CEP, who present with specific clinical scenarios. As demonstrated, treatment with benralizumab may be beneficial for patients with frequent CEP relapses. Clearly, benralizumab could be the drug of choice in patients who demonstrate serious adverse effects following OCS therapy. Likewise, benralizumab therapy seems to be preferred in patients with comorbidities that are expected to be aggravated under OCS treatment.
FOOTNOTES
Izhakian S and Rosengarten D contributed to the acquisition and interpretation of the data;Pertzov B and Kramer MR contributed to the critical revision of the manuscript for important intellectual content; all authors contributed to the drafting of the manuscript and approved the final version.
測評作為數學教育過程中的一個關鍵環節,肩負著提高數學教育質量、甄別人才的重要使命.高考作為一種重要的測評方式,在其中發揮著至關重要的作用,為了改善目前高考中數學學科核心素養考查的現狀,基于上述分析提出以下幾點建議.
Computed tomography (CT) of the chest (axial plain) showed a mediastinal lymphadenopathy, and pulmonary consolidations in the right upper and left lower lobes (Figure 1B).
The authors declare that they have no conflicts of interest related to this work.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Written informed consent was obtained from the patient for publication of this manuscript and any accompanying images.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
英國皇家海軍將軍艦的燃料由低燃燒值的煤炭改為高燃燒值的石油,提高了英國艦隊的速度,增大了活動范圍,燃料補充更加快捷,英國艦隊也就更加牢固地掌握了制海權。而以煤炭燃料的德國艦隊則受限于狹窄的范圍之內,欲出不得。戰爭爆發時,英國主力艦隊壓倒了德國公海艦隊。
Israel
Shimon Izhakian 0000-0003-1150-1057; Barak Pertzov 0000-0002-3077-3616; Dror Rosengarten 0000-0003-1754-5878; Mordechai R Kramer 0000-0003-2376-2393.
Wang JL (Online Science Editor)
Wang TQ
Ma YJ
1 Suzuki Y, Suda T. Eosinophilic pneumonia: A review of the previous literature, causes, diagnosis, and management.
2019 ; 68 : 413 -419 [PMID: 31253537 DOI: 10 .1016 /j.alit.2019 .05 .006 ]
2 Marchand E, Reynaud-Gaubert M, Lauque D, Durieu J, Tonnel AB, Cordier JF. Idiopathic chronic eosinophilic pneumonia.A clinical and follow-up study of 62 cases. The Groupe d'Etudes et de Recherche sur les Maladies "Orphelines" Pulmonaires(GERM"O"P).
1998 ; 77 : 299 -312 [PMID: 9772920 DOI: 10 .1097 /00005792 -199809000 -00001 ]
3 Durieu J, Wallaert B, Tonnel AB. Long-term follow-up of pulmonary function in chronic eosinophilic pneumonia. Groupe d'Etude en Pathologie Interstitielle de la Société de Pathologie Thoracique du Nord.
1997 ; 10 : 286 -291 [PMID:9042622 DOI: 10 .1183 /09031936 .97 .10020286 ]
4 Naughton M, Fahy J, FitzGerald MX. Chronic eosinophilic pneumonia. A long-term follow-up of 12 patients. Chest 1993 ;103 : 162 -165 [PMID: 8031327 DOI: 10 .1378 /chest.103 .1 .162 ]
5 Isomoto K, Baba T, Sekine A, Aiko N, Ogura T. Promising Effects of Benralizumab on Chronic Eosinophilic Pneumonia.
2020 ; 59 : 1195 -1198 [PMID: 32009090 DOI: 10 .2169 /internalmedicine.3606 -19 ]
6 Izumo T, Kuse N, Awano N, Tone M, Jo T, Yoshimura H, Minami J, Takada K, Muto Y, Fujimoto K, Inomata M. Rapid and sustained effects of a single dose of benralizumab on chronic eosinophilic pneumonia.
2020 ; 30 :101062 [PMID: 32373456 DOI: 10 .1016 /j.rmcr.2020 .101062 ]
7 Yazawa S, Toyoshima M, Koda K, Suda T. Benralizumab as initial treatment for chronic eosinophilic pneumonia.
2021 ; 70 : 140 -142 [PMID: 32807690 DOI: 10 .1016 /j.alit.2020 .07 .005 ]
8 Kolbeck R, Kozhich A, Koike M, Peng L, Andersson CK, Damschroder MM, Reed JL, Woods R, Dall'acqua WW, Stephens GL, Erjefalt JS, Bjermer L, Humbles AA, Gossage D, Wu H, Kiener PA, Spitalny GL, Mackay CR, Molfino NA, Coyle AJ.MEDI-563 , a humanized anti-IL-5 receptor alpha mAb with enhanced antibody-dependent cell-mediated cytotoxicity function.
2010 ; 125 : 1344 -1353 .e2 [PMID: 20513525 DOI: 10 .1016 /j.jaci.2010 .04 .004 ]
猜你喜歡
大眾投資指南(2021年23期)2021-12-06 05:46:42
電子競技(2019年22期)2019-03-07 05:17:26
電子競技(2019年21期)2019-02-24 06:55:52
電子競技(2019年20期)2019-02-24 06:55:35
電子競技(2019年19期)2019-01-16 05:36:09
消費導刊(2017年24期)2018-01-31 01:28:30
中國軍轉民(2017年7期)2017-12-19 13:30:10
新民周刊(2016年15期)2016-04-19 18:12:04
新民周刊(2016年15期)2016-04-19 15:47:52
漫畫月刊·炫版(2014年3期)2014-05-27 04:17:21
 World Journal of Clinical Cases2022年18期
World Journal of Clinical Cases2022年18期
- World Journal of Clinical Cases的其它文章
- Stem cells as an option for the treatment of COVID-19
- Development of clustered regularly interspaced short palindromic repeats/CRISPR-associated technology for potential clinical applications
- Prostate sclerosing adenopathy: A clinicopathological and immunohistochemical study of twelve patients
- Effectiveness and postoperative rehabilitation of one-stage combined anterior-posterior surgery for severe thoracolumbar fractures with spinal cord injury
- Construction and validation of a novel prediction system for detection of overall survival in lung cancer patients
- Identification of potential key molecules and signaling pathways for psoriasis based on weighted gene coexpression network analysis