Severe progression of autoimmune hepatitis in a young COVID-19 adult patient: A case report
2022-09-08 07:08:32NeerajKumarSushantSatyapriyaShaikMohammadTahaseenKunalSinghAbhyudayKumar
Journal of Acute Disease 2022年4期
Neeraj Kumar, Sushant Satyapriya, Shaik Mohammad Tahaseen, Kunal Singh, Abhyuday Kumar
1Department of Trauma & Emergency, AIIMS Patna, Bihar, India, 801505
2Department of Anaesthesiology, AIIMS Patna, Bihar, India, 801505
3Department of Medicine, AIIMS Patna, Bihar, India, 801505
ABSTRACT Rationale: The impact of COVID-19 in patients with autoimmune liver disease treated with immunosuppressive therapy has not been described so far. This case report describes the clinical course of a patient with autoimmune hepatitis (AIH) who developed COVID-19 and the features of cytokine syndrome leading to its deterioration in our intensive care unit.Patient’s Concern: A 28-year-old male presented with generalized anasarca for two weeks and chronic liver disease for 8 months.Diagnosis: AIH and Covid-19 with features of cytokine storm syndrome.Interventions: Intravenous furosemide, mannitol, syrup lactulose, steroids (prednisolone 40 mg), azathioprine 1 mg/kg body weight, rifaximin, vitamin K, and blood products.Outcomes: The patient had hepatic encephalopathy and AIH and died on the 10th day after admission despite ventilatory support, sustained low-efficiency hemodialysis, and resuscition.Lessons: The dramatic release of cytokines and the inflammatoryimmune responses not only alter the pathophysiology but also affects the onset and severity of disease progression in patients with AIH.
KEYWORDS: COVID-19; Autoimmune hepatitis; Cytokine storm syndrome; Immunosuppressant drugs; Liver dysfunction
1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection primarily affects the lungs. It has engulfed millions of lives throughout the world. Now with the worldwide epidemiological impact of chronic liver disease, a close analysis of interactions between pre-existing liver disease and COVID-19 is the need of the hour. The clinical impact of COVID-19 on patients with autoimmune liver disease who are treated with immunosuppressive therapy has not been described in the literature. Due to the unpredictable course of SARS-CoV-2 infection, patients with autoimmune hepatitis (AIH) are mainly immunosuppressed because of decompensated liver dysfunction and it raises great concern in clinical management[1]. AIH is an extremely rare autoimmune liver disease and its pathophysiology is still poorly understood, maintaining immunosuppression is required for its management[2]. Cytokine storm is an umbrella term encompassing several disorders of immune dysregulation characterized by constitutional symptoms, systemic inflammation, and multiorgan dysfunction that can lead to multiorgan failure[3]. Considering that cytokine storm syndrome (CSS) due to COVID-19 is associated with liver dysfunction, the use of antiviral (remdesivir), and immunomodulators (tocilizumab) in these patients is clinically controversial. Sudden relapse of AIH is reported following the stoppage of immunosuppressive drugs[4]. There is uncertainty on how to manage cytokine storms in these patients during the SARS-CoV-2 pandemic. This case report describes the clinical course of AIH which developed COVID-19, features of cytokine syndrome, and management in our intensive care unit of the dedicated COVID hospital.
2. Case report
Informed written consent was obtained from the patient for this case report. The patient has given his consent for images and other clinical information to be reported. The ethical approval has been obtained from the Ethical Committee of All India Institute of Medical Sciences Patna, Bihar, India.
A 28-years-old male patient who tested positive for COVID-19 was admitted to our hospital. From background history, our patient presented with generalized anasarca which initially started from the abdominal region, then developed bilateral lower limb followed by face and the whole body for the last 15 days. He had yellowish discoloration of urine, sclera, and the whole body, and all these features gradually increased in severity within the last 15 days of presentation. He was diagnosed with chronic liver disease 8 months ago and also had a 3-year history of alcohol consumption. He was known hypertensive for the last 1.5 years and on irregular medications. The patient was diagnosed with AIH type 1 as he was detected positive for antinuclear antibodies (ANA) and smooth muscle autoantibodies (SMA), with a titer of ANA/SMA antibody>1∶80. He was also perinuclear anti-neutrophil cytoplasmic antibodies (p-ANCA) positive. The serum immunoglobulin G (IgG) levels were normal and initial viral hepatitis markers were negative.
At the time of admission (Day 0), he was semi-conscious and slightly disoriented, with pallor and bilateral pedal edema. Heart rate was 120 beats per minute, blood pressure was 157/117 mm Hg, respiratory rate 21 bpm, random blood sugar (RBS) 124 mg/dL, Glasgow coma score (GCS) 12/15, SpO299% on 7 L/min O2(increasing demand), and initial serum ammonia level was 57.47 micromol/L. The patient tested negative for anti-HBsAg, anti-HCV, and HIV I and Ⅱ.
On initial ultrasound abdominal scan, it revealed a diffuse coarse and heterogenous hepatic echotexture throughout with nodular contour with no discrete mass and abnormal hepatic parenchyma, and presence of mild gallbladder wall thickening with sludge in the lumen, splenomegaly, and prominent porta hepatis lymph nodes with moderate ascites. The detailed day-wise clinical progression with laboratory values such as pathological, inflammatory parameters, and patient’s clinical progress is shown in Table 1. We made our diagnosis as AIH with chronic liver disease with features of CSS. On day 3 after admission, he was in severe respiratory distress with PaO2/FiO2ratio<150, respiratory rate was 45 rates per minute and SpO2measured was 88% and GCS was 9/15. Immediately he was intubated and put on mechanical ventilation on pressure control (PC) mode with the following ventilatory settings: FiO2=100, PC=19 cm H2O, positive end-expiratory pressure (PEEP)=9 cm H2O, I∶E=1∶2. All standard intensive COVID care management protocols were followed as per our institutional policy.
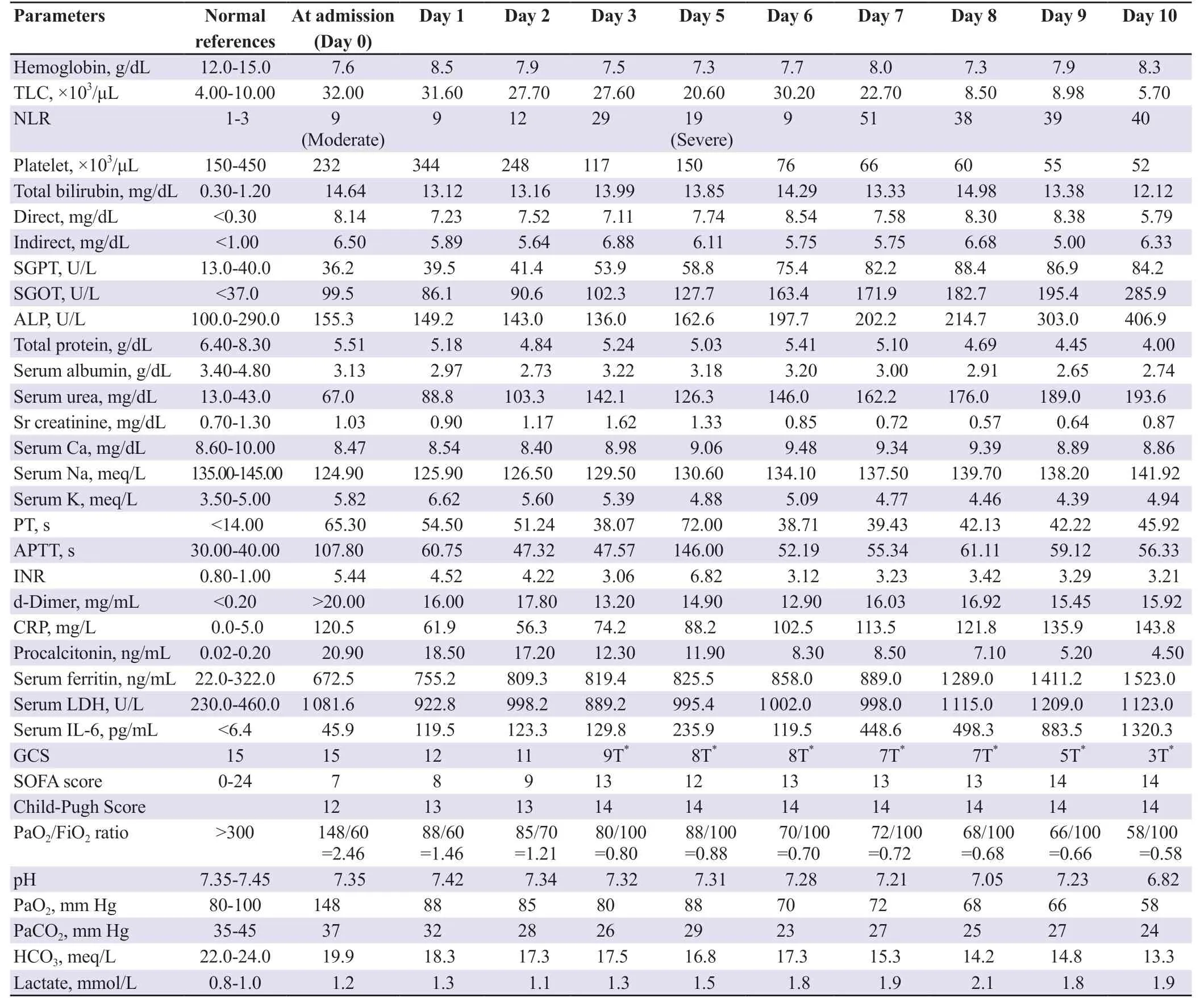
Table 1. Day-wise parameters of autoimmune hepatitis with COVID-19.
The patient was managed meticulously with intravenous fluid normal saline and dextrose-containing solution, diuretics (furosemide, mannitol) syrup lactulose, steroids (prednisolone 40 mg), azathioprine 1 mg/kg body weight, antimicrobial piperacillin plus tazobactam, doxycycline, rifaximin, metronidazole, vitamin K injection, and antihypertensive carvedilol. Gradually the patient developed renal deterioration with a rising trend of urea and creatinine with decreased urine output for which one session of sustained low efficacy hemodialysis was done every alternate day for three days. The total blood product like packed red blood cells (4 units), fresh frozen plasma (16 units), aphaeretic platelet (4 units), and cryoprecipitate (5 units) were transfused to correct falling hematocrit and deranged coagulation parameters. The patient had hepatic encephalopathy and AIH and died on the 10th day after admission despite ventilatory support, sustained low-efficiency hemodialysis, and efforts to resuscitate him.
3. Discussion
As per literature, the SARS-CoV-2 coronavirus is mainly characterized by inducing a respiratory disease, various studies have reported that up to 50% of patients present abnormal liver tests (transaminases). Interleukin 6 (IL-6) is believed to be an important inducer of the acute phase response and infection defense in the liver[5]. The hyperactivated inflammatory-immune mediated responses, lymphopenia, and CSS occurring in SARS-CoV-2 infection can impair the gut and liver[6]. The cytokine storm is mainly controlled by interrupting the signal transduction pathway of IL-6 with tocilizumab, which may be an effective drug for patients with severe COVID-19[7]. But in our case, the supposed beneficial effects of using immunomodulators (tocilizumab) were not utilized because of deranged liver enzymes and creatinine clearance. The cut-off for normal values of alanine aminotransferase (ALT) was considered 25 U/L for women and 35 U/L for men[8].Any patients with a new-onset ALT value greater than 2×upper limit normal has been defined as acute liver injury[9]. However, in our case, the ALT values at admission were 36.2 U/L and it increased to 75.4 U/L on day-6 and further increased to 86.9 U/L on Day-8 which was greater than 2×upper limit normal, making it a diagnosis of acute liver injury. Neutrophil lymphocyte ratio was initially 9 and then increased to 38; serum C reactive protein level was increased from 102.5 mg/L to 143.8 mg/L; serum ferritin increased from 672.5 ng/mL to 1 523 ng/mL and IL-6 from 45.9 pg/mL to 1 320.3 pg/mL on day-10, suggesting that the CSS may play a major prominent role in liver injury in our patient leading to clinical deterioration and death. Due to COVID-19 and stress, the normal homeostasis of the liver for maintaining immune balance through the intestine-liver axis is altered, the liver may act as a chief cytokine producer because it has the largest macrophage (Kupffer cells) in the body. The pre-existing liver disease may dysregulate the entire liver’s innate immune status and it might play a critical role in the COVID-19 outcome. The emphasis should be given to vaccination against influenza and Streptococcus pneumonia in immunosuppressed patients. The effect of immunosuppression on the severity of COVID-19 is still unclear. However, several reports suggested that even in highly endemic areas, patients with AIH are not at increased risk of adverse outcomes. There are high chances of relapse of AIH if the immunosuppressant’s medication is stopped or the dose is reduced thus it should be continued with an unchanged dose. We continued azathioprine in our case but his biochemical parameters, as well as clinical condition, rapidly deteriorated within 8-10 d. There is evidence that morbidity in COVID-19 may be due to hyper inflammation and cytokine storms with high levels of IL-6[10]. The dramatic release of cytokines and the inflammatoryimmune responses not only alter the pathophysiology but also affects the onset and severity of disease progression. So rapid and appropriate diagnostic tests and accurate prognosis are much needed.
COVID-19 pandemic greatly affects liver-related mortality, although it is hidden, delayed, and not much reported. Every AIH patient should strictly follow the protective guidelines issued in the COVID-19 pandemic. The immunosuppressive treatment should be continued during the COVID-19 pandemic and preventive measures always remain crucial and life-saving in these patients.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Authors’ contributions
N.K.: concept and design of the study, acquisition of data, drafting the article; S.S. and S.M.T.: acquisition of data, revising the article critically for important intellectual content; K.S. and A.K.: revising the article critically for important intellectual content.
 Journal of Acute Disease2022年4期
Journal of Acute Disease2022年4期
- Journal of Acute Disease的其它文章
- Challenges of COVID-19 prevention and control: A narrative review
- Delayed post-hypoxic leukoencephalopathy following barbiturate overdose: A case report
- Associated risk factors for post-COVID-19 mucormycosis at a tertiary care centre: A cross-sectional study
- Hematological indices as predictors of mortality in dengue shock syndrome: A retrospective study
- Different routine laboratory tests in assessment of COVID-19: A casecontrol study
- Effect of oral premedication of midazolam, ketamine, and dexmedetomidine on pediatric sedation and ease of parental separation in anesthesia induction for elective surgery: A randomized clinical trial