不同劑量氨甲環(huán)酸對(duì)老年股骨頸骨折全髖置換術(shù)失血的影響
2023-06-28 20:13:33李傳波鄒阿鵬王青青曲哲付繁剛王京生
上海醫(yī)藥 2023年7期
李傳波 鄒阿鵬 王青青 曲哲 付繁剛 王京生

摘 要 目的:分析術(shù)前靜脈滴注高、低劑量氨甲環(huán)酸(tranexamic acid, TXA)對(duì)老年股骨頸骨折全髖置換術(shù)(total hip arthroplasty, THA)失血的影響。方法:選取THA 患者87例,分為低劑量A組(43例,TXA 15 mg/kg)和高劑量B組(44例,TXA 50 mg/kg)。比較兩組圍手術(shù)期失血量,術(shù)后血紅蛋白減少量,輸血量及下肢深靜脈血栓形成。結(jié)果:兩組間顯性失血量(DBL)、總失血量(TBL)、術(shù)前與術(shù)后24 h測(cè)得的血紅蛋白量差值的比較差異有統(tǒng)計(jì)學(xué)意義,而輸血量及并發(fā)癥差異無統(tǒng)計(jì)學(xué)意義。結(jié)論:術(shù)前0.5 h靜脈滴注50 mg/kg高劑量TXA在減少手術(shù)失血量方面效果好,且不增加血栓等并發(fā)癥形成風(fēng)險(xiǎn)。
關(guān)鍵詞 氨甲環(huán)酸 股骨頸骨折 全髖置換術(shù) 血紅蛋白 輸血
中圖分類號(hào):R973.2; R687.4 文獻(xiàn)標(biāo)志碼:B 文章編號(hào):1006-1533(2023)07-0019-03
引用本文 李傳波, 鄒阿鵬, 王青青, 等. 不同劑量氨甲環(huán)酸對(duì)老年股骨頸骨折全髖置換術(shù)失血的影響[J]. 上海醫(yī)藥, 2023, 44(7): 19-21.
Effects of different doses of tranexamic acid on blood loss in elderly patients with femoral neck fractures undergoing total hip arthroplasty
LI Chuanbo 1, ZOU Apeng 1, WANG Qingqing 2, QU Zhe 3, FU Fangang 1, WANG Jingsheng 1
(1. Department of Bone and Joint; 2. Department of Traumatic Orthopedic; 3. Department of Emergency, Yantai Hospital affiliated to Binzhou Medical University, Yantai 264100, China)
ABSTRACT Objective: To analyze the clinical effect of preoperative intravenous infusion of high- or low-dose tranexamic acid (TXA) on blood loss in elderly patients with femoral neck fracture undergoing total hip arthroplasty (THA). Methods: A total of 87 elderly patients with femoral neck fracture undergoing THA were selected and divided into group A (43 cases, TXA 15 mg/kg) and group B (44 cases, TXA 50 mg/kg). Perioperative blood loss, postoperative hemoglobin reduction, blood transfusion volume, lower limbs deep vein thrombosis were compared between the two groups. Results: There were significant differences between the two groups in dominant blood loss ( DBL), total blood loss (TBL), the difference of hemoglobin content determined between pre-operation and 24 hours after operation, but not in blood transfusion volume and incidence of complications. Conclusion: High-dose TXA (50 mg/kg) given intravenously at 0.5 h before surgery has good effect in reducing blood loss without increasing the risk of complications such as thrombosis.
KEY WORDS tranexamic acid; femoral neck fracture; total hip arthroplasty; hemoglobin; blood transfusion
全世界老年患者骨質(zhì)疏松性髖部骨折的發(fā)生率持續(xù)增長(zhǎng),股骨頸骨折是老年人群中最常見的髖部骨折類型,用全髖置換術(shù)(total hip arthroplasty,THA)治療有較好的療效[1]。隨著圍手術(shù)期管理和康復(fù)技術(shù)的提高,大大降低了髖部骨折術(shù)后的死亡率。老年患者往往罹患多種疾病,術(shù)前貧血也很常見,而THA術(shù)中及術(shù)后出血也在所難免,因此,臨床常使用氨甲環(huán)酸(tranexamic acid,TXA)減少圍手術(shù)期出血。國(guó)內(nèi)外文獻(xiàn)[2-3]報(bào)道的其靜脈常用劑量為10 mg/kg或15 mg/kg。在本研究中,于術(shù)前0.5 h分別靜脈滴注TXA 15 mg/kg或50 mg/kg 1次,分析其對(duì)初次THA手術(shù)失血量的影響,現(xiàn)報(bào)告如下。
1 資料與方法
1.1 研究對(duì)象
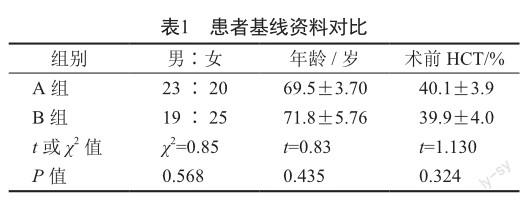
根據(jù)納入與排除標(biāo)準(zhǔn),收集本院2020年1月至2021年3月共87例股骨頸骨折患者,由同一位醫(yī)生為患者進(jìn)行THA手術(shù),根據(jù)TXA用藥劑量不同分為低劑量A組(15 mg/kg)43例,男23例,女20例;高劑量B組(50 mg/kg)44例,男19例,女25例。
1.2 納入標(biāo)準(zhǔn)
①低能量損傷的單側(cè)股骨頸骨折,無其他部位合并傷;②年齡大于65歲;受傷前能夠自主行走,生活自理;③術(shù)前評(píng)估顯示患者身體狀況能夠耐受手術(shù)和麻醉。本研究經(jīng)醫(yī)院倫理審查委員會(huì)審查通過,手術(shù)前簽訂知情同意書。
1.3 排除標(biāo)準(zhǔn)
①病理性股骨頸骨折;②既往有深靜脈血栓、肺栓塞、腦栓塞和腦梗死史的患者;③凝血功能障礙的患者,國(guó)際標(biāo)準(zhǔn)化比值(INR)以及活化部分凝血活酶時(shí)間(activated partial thromboplastin time,APTT)高于正常范圍1倍以上者;④對(duì)TXA過敏;⑤嚴(yán)重的心肺肝腎功能不全,不能耐受手術(shù)和麻醉;⑥術(shù)前血紅蛋白(Hb)量低于100 g/L,預(yù)計(jì)圍手術(shù)期需要輸血者。
1.4 治療方法
所有手術(shù)均由科內(nèi)同一位高資歷醫(yī)生完成,手術(shù)入路均采用后外側(cè)入路,假體同為生物型髖關(guān)節(jié)假體(德國(guó)LINK),切皮前0.5 h給予靜脈滴注TXA,術(shù)后均放置引流管,于24 h后拔除。住院期間兩組患者均按術(shù)后12 h開始給予依諾肝素預(yù)防量每日1次皮下注射抗凝,出院后口服利伐沙班片至35 d預(yù)防下肢深靜脈血栓形成。
1.5 評(píng)價(jià)方法
測(cè)定術(shù)前Hb、術(shù)后24 h Hb含量及計(jì)算其差值。一般根據(jù)Gross[4]提出的公式來計(jì)算總失血量(total blood loss,TBL)及基于紅細(xì)胞壓積來計(jì)算失血量,包括組織外滲的失血量。公式為:TBL=EBV×(Ho-HF)÷HAV,其中EBV(總循環(huán)血容量)用Nadler[5]方法來計(jì)算,總血容量=k1×身高(m)3+k2×體質(zhì)量(kg)+k3(男性k1=0.366 9,k2=0.032 19,k3=0.604 1;女性k1=0.356 1,k2=0.033 08,k3=0.183 3),Ho為患者術(shù)前的紅細(xì)胞比容(hematocrit value,HCT),HF為患者術(shù)后HCT,HAV為患者術(shù)前術(shù)后HCT的均值。顯性失血量(dominant blood loss,DBL)可認(rèn)為是術(shù)中出血量和術(shù)后總引流量之和。術(shù)中出血量=術(shù)中引流瓶總量-沖洗的液體量+紗布上的血液量。隱性失血量= TBL-DBL+總輸血量。采用統(tǒng)一的輸血方案,即術(shù)后Hb量低于70 g/L或Hb量低于80 g/L且伴有明顯貧血癥狀(頭暈,惡心,心率大于100次/min,血壓低于90/60 mmHg,并有下降趨勢(shì))則給予術(shù)后輸血。術(shù)后注意觀察患肢腫脹情況,彩超復(fù)查下肢靜脈有無深靜脈血栓。
1.6 統(tǒng)計(jì)學(xué)方法
應(yīng)用SPSS 23.0統(tǒng)計(jì)學(xué)軟件進(jìn)行數(shù)據(jù)分析。兩組計(jì)數(shù)資料的比較采用χ2檢驗(yàn)。兩組計(jì)量資料以x±s表示,組間的比較采用兩獨(dú)立樣本t檢驗(yàn)。P<0.05提示差異有統(tǒng)計(jì)學(xué)意義。
2 結(jié)果
組間性別分布、年齡、術(shù)前HCT差異無統(tǒng)計(jì)學(xué)意義(表1,P>0.05)。
術(shù)前0.5 h靜脈應(yīng)用高劑量TXA,DBL、TBL均顯著低于低劑量組,術(shù)前與術(shù)后24 h Hb測(cè)量差值對(duì)比有統(tǒng)計(jì)學(xué)意義(表2,P<0.05);術(shù)前高劑量TXA靜脈滴注較低劑量能夠明顯提高術(shù)后Hb量,但在輸血率方面差異無統(tǒng)計(jì)學(xué)意義(表2,P>0.05)。
3 討論
全髖關(guān)節(jié)置換的手術(shù)量隨老年股骨頸骨折的增加而逐漸增多,應(yīng)用氨甲環(huán)酸減少出血是圍手術(shù)期的重要組成部分[6]。孫朝軍等[7]在研究中證實(shí)了TXA在THA中減少失血方面的效果。多數(shù)研究者[8-9]支持在切皮前0.5 h給予TXA能減少失血,對(duì)保持術(shù)后Hb量有益,并且降低了住院費(fèi)用以及輸血和貧血的風(fēng)險(xiǎn)。
TXA的止血作用已被很多文獻(xiàn)證實(shí)有效,故本研究中未再設(shè)置空白對(duì)照組。Reina等[10]報(bào)道在THA中按照30 mg/kg單次應(yīng)用TXA能夠顯著減少出血。Lin等[11]報(bào)道術(shù)前應(yīng)用高劑量TXA較低劑量的出血更少。有關(guān)TXA的隨機(jī)雙盲安慰劑對(duì)照試驗(yàn)證實(shí)其半衰期為3.1 h[12],所以本研究術(shù)后12 h開始抗凝時(shí)不會(huì)影響TXA作用結(jié)果和并發(fā)癥發(fā)生率。
本研究結(jié)果表明,TXA能減少出血,且在一定劑量范圍內(nèi)效果隨其劑量增大而增強(qiáng),但并沒有很顯著的提高。研究中兩組患者均未發(fā)現(xiàn)肺栓塞、下肢靜脈血栓及其他并發(fā)癥發(fā)生,說明TXA 50 mg/kg高劑量應(yīng)用的安全性有保障,且未發(fā)現(xiàn)并發(fā)癥發(fā)生率的增加。這些與崔丹荔等[13]和其他一些學(xué)者[14-15]在他們類似研究中所報(bào)道的結(jié)果基本一致。
本研究也存在一些局限性,如排除了高危患者;未考慮在手術(shù)技術(shù)和輸血方案上的差異及術(shù)中止血類型及技巧對(duì)出血量的影響。因此,應(yīng)該繼續(xù)前瞻性研究監(jiān)測(cè)高劑量TXA報(bào)告的不良事件的發(fā)生率。
參考文獻(xiàn)
[1] Wood GC, Mclauchlan GJ. Outcome assessment in the elderly after total hip arthroplasty[J]. J Arthroplasty, 2006, 21(3): 398-404.
[2] 施林軍, 曹揚(yáng), 姜丹生. 不同劑量氨甲環(huán)酸對(duì)初次全髖關(guān)節(jié)置換失血量的影響[J]. 臨床骨科雜志, 2015, 18(4): 437-439.
[3] Wind TC, Barfield WR, Moskal JT. The effect of tranexamic acid on transfusion rate in primary total hip arthroplasty[J]. J Arthroplasty, 2014, 29(2): 387-389.
[4] Gross JB. Estimating allowable blood loss: corrected for dilution[J]. Anesthesiology, 1983, 58(3): 277-280.
[5] Nadler SB, Hidalgo JH, Bloch T. Prediction of blood volume in normal human adults[J]. Surgery, 1962, 51(2): 224-232.
[6] Hare GM, Freedman J, David Mazer C. Review article: risks of anemia and related management strategies: can perioperative blood management improve patient safety?[J]. Can J Anaesth, 2013, 60(2): 168-175.
[7] 孫朝軍, 李紅, 胡志富, 等. 短期多次使用氨甲環(huán)酸對(duì)人工膝關(guān)節(jié)置換術(shù)后出血量的影響[J]. 云南醫(yī)藥, 2013, 34(6): 487-489.
[8] Xu S, Chen JY, Zheng Q, et al. The safest and most efficacious route of tranexamic acid administration in total joint arthroplasty: a systemic review and network metaanalysis[J]. Thromb Res, 2019, 176: 61-66.
[9] Maalouly J, Tawk A, Ayoubi R, et al. Efficacy of the combined administration of systemic and intra-articular tranexamic acid in total hip arthroplasty secondary to femoral neck fracture: a retrospective study[J]. Adv Orthop, 2020, 2020: 9130462.
[10] Reina N, Fennema P, Hourlier H. The impact of mild perioperative hypothermia on the effectiveness of tranexamic acid in total hip arthroplasty[J]. Int Orthop, 2017, 41(1): 55-60.
[11] Lin Jd, Lenke Lg, Shillingford JN, et al. Safety of a high-dose tranexamic acid protocol in complex adult spinal deformity: analysis of 100 consecutive cases[J]. Spine Deform, 2018, 6(2): 189-194.
[12] CRASH-2 collaborators, Roberts I, Shakur H, et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial[J]. Lancet, 2011, 377(9771): 1096-1101.
[13] 崔丹荔, 雷一霆, 許宏, 等. 人工全髖關(guān)節(jié)置換術(shù)中首次大劑量聯(lián)合術(shù)后五次靜脈應(yīng)用氨甲環(huán)酸的前瞻性臨床研究[J]. 中國(guó)修復(fù)重建外科雜志, 2019, 33(8): 935-939.
[14] Wang D, Luo ZY, Yu ZP, et al. The antifibrinolytic and antiinflammatory effects of multiple doses of oral tranexamic acid in total knee arthroplasty patients: a randomized controlled trial[J]. J Thromb Haemost, 2018, 16(12): 2442-2453.
[15] 劉艦. 氨甲環(huán)酸不同用法在初次全髖關(guān)節(jié)置換圍手術(shù)期臨床療效比較分析[D]. 長(zhǎng)春: 吉林大學(xué), 2017.
