阿司匹林聯合雙嘧達莫在缺血性卒中二級預防中療效及安全性的Meta分析
2014-08-10 12:28:25魏崢嶸梅思靜張兆輝
疑難病雜志 2014年2期
魏崢嶸,梅思靜,張兆輝
薈萃分析
阿司匹林聯合雙嘧達莫在缺血性卒中二級預防中療效及安全性的Meta分析
魏崢嶸,梅思靜,張兆輝
目的系統評價聯合應用阿司匹林及雙嘧達莫在缺血性卒中二級預防中的療效及安全性。方法檢索PUBMED、Cochrane Database of Systematic Reviews、EMBASE、中國知網、萬方數據中關于聯合應用阿司匹林及雙嘧達莫進行卒中二級預防的隨機對照試驗,同時對納入文獻的參考文獻進行篩選,根據納入和排除標準嚴格篩選,對符合納入標準的研究采用Revman 5.0軟件進行Meta分析。結果共納入5篇符合標準的RCT,包括腦梗死或TIA患者8 619例,治療組(聯合應用阿司匹林和雙嘧達莫)4 315例,對照組(單用阿司匹林)4 304例。Meta分析結果顯示:聯合應用阿司匹林和雙嘧達莫進行卒中二級預防與單用阿司匹林相比,顯著降低卒中復發率(OR=0.84,95%CI 0.73~0.97,P=0.02)及缺血事件發生率(OR=0.80,95%CI 0.69~0.92,P=0.002),而主要出血發生率(OR=0.91,95%CI 0.73~1.14,P=0.41)和病死率(OR=0.90,95%CI 0.78~1.04,P=0.16)無明顯差異。結論與單用阿司匹林相比,聯合應用阿司匹林及雙嘧達莫進行卒中二級預防,能顯著降低卒中復發率、缺血事件發生率,且不增加出血發生率和病死率。
卒中,缺血性;阿司匹林;雙嘧達莫;二級預防;Meta分析
腦梗死是中老年人的常見病、多發病,其發病率、致死率、致殘率高,嚴重危害中老年人健康。腦梗死后30d病死率約8%,1年病死率22%,5年病死率45%[1]。腦梗死后5年累積復發率約30%,約為正常人群的9倍,其中首次發病后第1年復發率最高,約13%,是正常人群發病率的15倍[2~4]。因此腦梗死或TIA后進行卒中二級預防至關重要。阿司匹林作為抗血小板藥物廣泛用于卒中二級預防,但阿司匹林作用有限,僅能夠預防13%~22%的血管事件[5,6]。多種抗血小板藥物聯用,是否更能減少卒中復發,其安全性如何,是否增加出血風險,未能有明確結果。1996年歐洲卒中預防研究(ESPS2)顯示,與單用阿司匹林相比,聯合應用阿司匹林和雙嘧達莫進行卒中二級預防更有效[7]。為了解阿司匹林、雙嘧達莫聯合應用對比單用阿司匹林預防卒中復發的療效和安全性,筆者檢索相關文獻,應用循證醫學方法進行統計學分析。
1 資料與方法
1.1 檢索方法 以“阿司匹林”“雙嘧達莫”“腦梗死”“TIA”為關鍵詞檢索中國知網、萬方數據庫。以英文關鍵詞“aspirin”“dipyridamole”“cerebral ischemia stroke”“TIA”為關鍵詞檢索PUBMED、Cochrane Database of Systematic Reviews、EMBASE,末次檢索時間為2013年7月,并對納入文獻的參考文獻進行追蹤檢索。
1.2 文獻納入和排除標準
1.2.1 文獻的納入標準:納入研究對象均為腦梗死或TIA患者,應用抗血小板預防卒中復發,試驗組為聯合應用阿司匹林和雙嘧達莫,對照組單用阿司匹林,主要觀察指標包括卒中復發率、缺血事件發生率、主要出血發生率、病死率。符合上述條件的隨機對照試驗(RCTs)均被納入研究。
1.2.2 文獻的排除標準:非隨機對照研究,觀察性研究,試驗組為單用阿司匹林、雙嘧達莫、或其他抗血小板藥物聯用,或對照組為空白對照,文獻數據不全或無法獲得全文均被排除。
1.3 文獻質量和評價 根據Cochrane Handbook for Systematic Reviews of Interventions推薦的文獻質量評價標準[8],對每篇RCT質量進行獨立評價:(1)隨機序列的產生是否充分;(2)是否分配隱藏;(3)是否采用雙盲;(4)是否報道退出或失訪及其原因;(5)是否采用意向治療分析;(6)是否分析基線可比性。根據上述標準,文獻質量分3級:A級,完全滿足上述標準,發生各種偏移可能性小;B級,部分滿足上述標準,發生偏移可能性為中度;C級,完全不滿足上述標準,發生偏移可能性大。
1.4 資料提取 仔細閱讀納入研究全文后提取數據,即研究的基本資料,包括樣本的入選標準和樣本量、研究對象基本資料、分配方法、干預措施、結局的觀察指標等。
1.5 統計學分析 采用Revman 5.0軟件對提取的納入文獻進行Meta分析。首先采用χ2檢驗對納入研究進行異質性分析:若P>0.1,I2<50%,即多個納入研究具有同質性,則選用固定效應模型分析,統計方法選用Mantel-Haenszel法[9];若P<0.1,I2≥50%,各研究存在統計學異質性,但無臨床異質性或無臨床意義,則選用隨機效應模型,統計方法選用DerSimonian-Laird法[10]。
2 結 果
2.1 納入文獻 本研究初步檢索出相關文獻591篇,均為英文文獻,瀏覽文獻摘要后選出大致符合納入標準的全文文獻45篇,仔細閱讀全文,排除不符合條件者,最終納入5篇符合標準的RCT文獻。
2.2 質量評價 5篇納入文獻的質量評價均為A級,具有評價指標和結果。見表1。

表1 納入研究質量評價
2.3 研究特征 綜合5篇納入RCTs,共包括8 619例腦梗死或TIA患者,治療組(聯合應用阿司匹林和雙嘧達莫,簡稱AD組)4 315例,對照組(單用阿司匹林,簡稱A組)4 304例。見表2。
2.4 聯用阿司匹林及雙嘧達莫在缺血性卒中二級預防中療效和安全性
2.4.1 卒中復發率:5篇RCTs共8 619例,AD組4 315例,其中卒中復發369例;A組4 304例,卒中復發431例。各研究間無異質性(P=0.17,I2=38%),選擇固定效應模式進行Meta分析,結果顯示:AD組卒中復發率低于A組,差異有統計學意義(OR=0.84,95%CI 0.73~0.97,P=0.02)。見圖1。

表2 納入研究特征 (例)
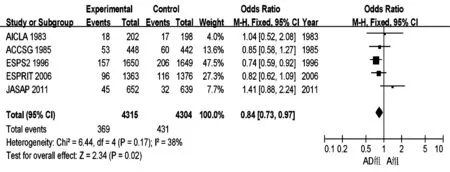
圖1 AD組與A組卒中復發率的Meta分析
2.4.2 缺血事件發生率:3篇RCTs共7 329例,AD組3 665例,其中缺血事件發生403例;A組3 664例,缺血事件491例。各研究間無異質性(P=0.21,I2=36%),選擇固定效應模式進行Meta分析,結果顯示:AD組卒中缺血事件發生率低于A組,差異有統計學意義(OR=0.80,95%CI 0.69~0.92,P=0.002)。見圖2。
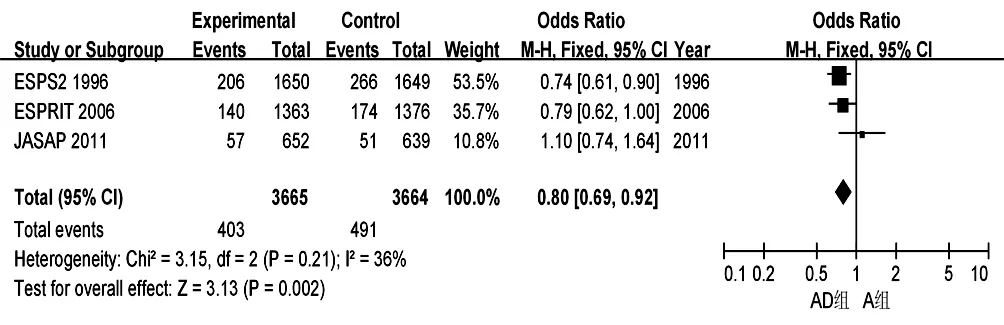
圖2 AD組與A組缺血事件發生率的Meta分析
2.4.3 主要出血發生率:5篇RCTs共8 619例,AD組4 315例,其中主要出血159例;A組4 304例,主要出血173例。各研究間無異質性(P=0.39,I2=4%),選擇固定效應模式進行Meta分析,結果顯示:AD組與A組出血發生率無明顯差異(OR=0.91,95%CI 0.73~1.14,P=0.41)。見圖3。
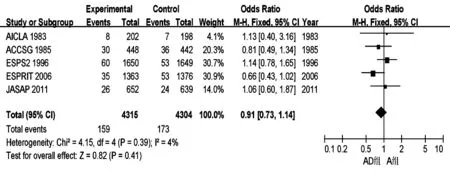
圖3 AD組與A組主要出血發生率的Meta分析
2.4.4 病死率:5篇RCTs共8 619例,AD組4 315例,其中病死416例;A組4 304例,病死456例。各研究間無異質性(P=0.15,I2=40%),選擇固定效應模式進行Meta分析,結果顯示:AD組與A組病死率無明顯差異(OR=0.90,95%CI 0.78~1.04,P=0.16)。見圖4。
3 討 論
目前已有多個研究阿司匹林、雙嘧達莫聯用預防卒中復發的試驗,其中:1983年的AICLA研究和1985年的ACCOGS研究顯示兩藥聯用并不優于單用阿司匹林[11,12];1996年Diener等[7]研究顯示兩藥聯用明顯優于安慰劑;2006年Halkes等[13]研究顯示阿司匹林、雙嘧達莫優于阿司匹林或雙嘧達莫任何一種藥物的單用;Bath等[16]研究顯示阿司匹林與雙嘧達莫聯用效果等同于氯吡格雷。2011年在日本完成的JASAP研究顯示,阿司匹林與雙嘧達莫聯用在減少卒中復發方面并不明顯優于單用阿司匹林[14]。關于其他抗血小板藥物的聯用方式,如MATCH研究,結果顯示阿司匹林與氯吡格雷聯用,在減少卒中復發方面并無明顯優勢,且長期服用還增加出血事件發生率[17],所以本研究未納入此兩藥聯用。
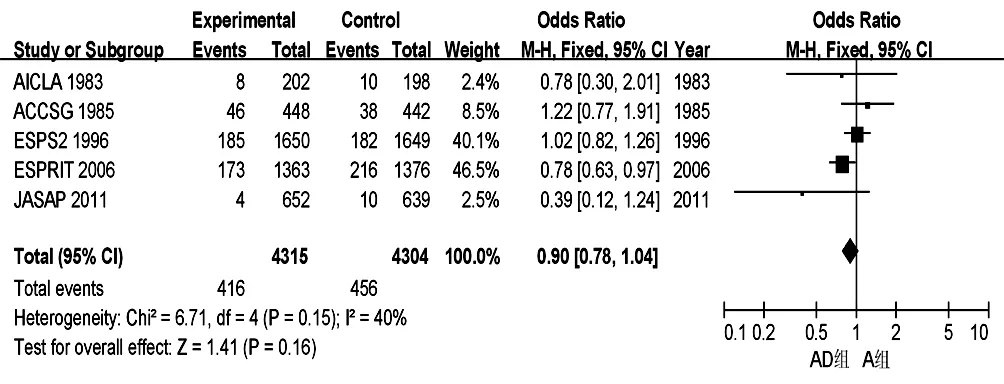
圖4 AD組與A組病死率的Meta分析
本Meta分析結果表明:阿司匹林、雙嘧達莫聯用與單用阿司匹林相比,能顯著降低卒中復發率、缺血事件發生率,且當口服抗血小板治療達1年以上時,主要出血事件發生率無明顯差異,但聯用在降低病死率方面亦與單用阿司匹林相似。在一些國家,已有指南推薦緩釋雙嘧達莫+阿司匹林聯用作為腦卒中二級預防的有效治療藥物,如2010年AHA/ASA更新的腦梗死或TIA后卒中二級預防推薦阿司匹林、雙嘧達莫聯用優于單用阿司匹林[18]。然而中國的卒中預防指南并未推薦阿司匹林、雙嘧達莫聯用作為有腦梗死或TIA病史患者的常規治療。所以本Meta分析旨在判定阿司匹林、雙嘧達莫聯用成為卒中預防的另一選擇。
5個納入研究中,2個研究均得出阿司匹林、雙嘧達聯用優于單用阿司匹林,其卒中復發率、缺血事件發生率均低于后者,且出血事件兩者差異不顯著[7,13]。3個研究未得出類似結果,可能是由于這些研究樣本量較少,權重低導致[11,12,14]。各研究中使用的雙嘧達莫劑型不同,其藥物效果亦不同,亦能影響研究結果。各研究中阿司匹林、雙嘧達莫的用量不同,也能影響研究結果。由于雙嘧達莫的頭痛不良反應發生率高,患者依從性低,未能完成研究,也能影響結果。因此,盡管本研究得出阿司匹林、雙嘧達莫聯用優于單用阿司匹林的結果,但未來仍需進行大樣本、藥物劑型用法規范的臨床試驗。
1 Sacco RL,Shi T,Zamanillo MC,et al. Predictors of mortality and recurrence after hospitalized cerebral infarction in an urban community: the Northern Manhattan Stroke Study[J].Neurology,1994,44(4): 626-634.
2 Sacco RL,Wolf PA,Kannel WB,et al. Survival and recurrence following stroke: the Framingham study[J].Stroke,1982,13(3): 290-295.
3 Burn J,Dennis M,Bamford J,et al. Long-term risk of recurrent stroke after a first-ever stroke: the Oxfordshire Community Stroke Project[J]. Stroke,1994,25(9): 333-337.
4 Petty GW,Brown RD Jr,Whisnant JP,et al. Survival and recurrence after first cerebral infarction: a population-based study in Rochester, Minnesota, 1975through 1989[J]. Neurology,1998,50(1): 208-216.
5 Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death,myocardial infarction,and stroke in high risk patients[J]. BMJ,2002,324(7329): 71-86.
6 Algra A,van Gijn. Cumulative meta-analysis of aspirin efficacy after cerebral ischaemia of arterial origin[J]. J Neurol Neurosurg Psychiatry,1999,66(2): 255.
7 Diener HC,Cunha L,Forbes C,et al. European stroke prevention study.2. Dipyridamole and acetylsalicylic acid in the secondary prevention of stroke[J].J Neurol Sci,1996,143(1-2): 1-13.
8 Higgins JP,Green S. Cochrane Handbook for Systematic Reviews of Interventions version 5.0.2 [M].The Cochrane Collaboration,2009:201-203.
9 Mantel N,Haenszel W. Statistical aspects of the analysis of data from restrospective studies of disease[J].J Natl Cancer Inst,1959,22(4):719-748.
10 DerSimonian R,Laird N. Meta-analysis in clinical trials[J].Controlled Clinical Trials,1986,7(3):177-188.
11 Bousser MG,Eschwege E,Haguenau M,et al. AICLA controlled trial of aspirin and dipyridamole in the secondary prevention of atherothrombotic cerebral ischemia[J]. Stroke,1983,14(1):5-14.
12 The ACCOSG. Persantine aspirin trial in cerebral ischemia. Part II: Endpoint results.The American-Canadian Co-Operative Study group[J].Stroke,1985,16(3): 406-415.
13 Halkes PH,van Gijn J,Kappelle LJ,et al. Aspirin plus dipyridamole versus aspirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomized controlled trial[J]. Lancet,2006,367(9523): 1665-1673.
14 Uchiyama S,Ikeda Y,Urano Y,et al. The Japanese aggrenox (extended-release dipyridamole plus aspirin) stroke prevention versus aspirin programme (JASAP) study: a randomized,double-blind,controlled trial[J]. Cerebrovasc Dis,2011,31(6): 601-613.
15 No al. The European Stroke Prevention Study (ESPS). Principal end-points. The ESPS Group[J]. Lancet,1987,12(2):1351-1354.
16 Bath PM,Cotton D,Martin RH,et al. Effect of combined aspirin and extended-release dipyridamole versus clopidogrel on functional outcome andrecurrence in acute,mild ischemic stroke: PRoFESS subgroup analysis[J]. Stroke,2010,41(4): 732-738.
17 Diener HC,Boqpusslavsky J,Brass LM,et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients(MATCH): randomised,double-blind,placebo-controlled trial[J]. Lancent,2004,364(9431): 331-337.
18 Adams RJ,Albers G,Alberts MJ,et al. Update to the AHA/ASA recommendations for the prevention of stroke in patients with stroke and transient ischemic attack[J]. Stroke,2008,39(5): 1647-1652.
Meta-analysisofefficacyandsafetyofaspirinanddipyridamoleinthesecondarypreventionofischemicstroke
WEIZhengrong,MEISijing,ZHANGZhaohui.
DepartmentofNeurology,People'sHospitalofWuhanUniversity,Wuhan430060,ChinaCorrespondingauthor:ZHANGZhaohui,E-mail:weizr0106@163.com
ObjectiveTo evaluate the efficacy and safety of combination therapy of aspirin and dipyridamole in secondary prevention of ischemia stroke.MethodsRetrieval PUBMED, Cochrane Database of Systematic Reviews, EMBASE, CNKI, found articles about conducted randomized controlled trials of combination of aspirin and dipyridamole in the secondary prevention of stroke, while the included literature references were screened according to inclusion rigorous screening and exclusion criteria, the study met the inclusion criteria for the use of Revman 5.0Meta-analysis software.ResultsA total of five sub-standard RCT, including 8 619patients with cerebral infarction or TIA, treated group (combination of aspirin and dipyridamole) of 4 315patients, 4 304 cases in the control group (aspirin alone). Meta-analysis showed that: the combination of aspirin and dipyridamole conduct secondary prevention of stroke compared with aspirin alone, significantly reduces the recurrence rate of stroke (OR = 0.84, 95% CI 0.73-0.97,P=0.02) and lack of blood event rate (OR= 0.80, 95% CI 0.69-0.92,P= 0.002), whereas the incidence of major bleeding (OR = 0.91, 95% CI 0.73-1.14,P=0.41) and mortality (OR = 0.90, 95% CI 0.78-1.04,P=0.16) showed no significant difference.ConclusionCompared with aspirin alone, the combination of aspirin and dipyridamole conduct secondary prevention of stroke, can significantly reduce the recurrence rate of stroke and the incidence of ischemic events without increasing the incidence of bleeding and mortality.
Cerebral stroke,ischemic; Aspirin; Dipyridamole; Secondary prevention; Meta-analysis
430060 武漢大學人民醫院神經內科
張兆輝,E-mail:weizr0106@163.com
10.3969/ j.issn.1671-6450.2014.02.028
2013-10-15)
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
天津外國語大學學報(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
科技傳播(2019年22期)2020-01-14 03:06:54
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
電子制作(2018年18期)2018-11-14 01:48:24
汽車工程學報(2017年2期)2017-07-05 08:13:02
山東工業技術(2016年15期)2016-12-01 05:31:22
中國中醫藥現代遠程教育(2014年11期)2014-08-08 13:23:44
