不同儀器測量角膜曲率的準確性研究
2015-01-16 07:48:01柏全豪苗雨晴扈月平張戈非
中國醫藥科學 2015年3期
關鍵詞:測量
柏全豪苗雨晴扈月平張戈非
1.大連市友誼醫院眼科,遼寧大連 116001;2.大連市友誼醫院綜合科,遼寧大連116001
不同儀器測量角膜曲率的準確性研究
柏全豪1苗雨晴2扈月平1張戈非1
1.大連市友誼醫院眼科,遼寧大連 116001;2.大連市友誼醫院綜合科,遼寧大連116001
目的研究比較手動角膜曲率計、電腦自動驗光儀、角膜地形圖和光學相干生物測量儀(IOL-Master)四種儀器測量角膜曲率的測量結果準確性。方法應用四種儀器分別測量擬施行白內障超聲乳化摘除及人工晶體植入術的患者86例(124眼)的平均、最大及最小角膜屈光力、角膜散光度數及散光軸位,用SPSS15.0軟件對測量參數進行統計學分析。結果這四種儀器測得的平均、最大及最小角膜屈光力、角膜散光度數無顯著差異(P>0.05),角膜散光軸位測量結果有顯著差異(P<0.01)。結論四種儀器測量角膜曲率的準確性較好。
手動角膜曲率計;電腦自動驗光儀;角膜地形圖;光學相干生物測量儀;人工晶體
白內障是主要的致盲眼病[1],隨著白內障手術技術的提高,尤其是新型人工晶狀體的臨床應用,使人們能夠獲得更好的視覺質量。因此,對所植入人工晶狀體屈光度的正確計算,對于白內障術后屈光質量起到重要作用。本研究的目的是通過探討手動角膜曲率計、電腦驗光儀、角膜地形圖儀和光學相干生物測量儀(IOL-Master)四種儀器測量角膜曲率的差異,以指導其在臨床中的應用。
1 資料與方法
1.1 一般資料
2013年11月~2014年2月在大連市友誼醫院眼科施行白內障超聲乳化摘除及人工晶體植入手術的患者86例(124眼),其中男46例(48眼),女48例(51眼),年齡50~90歲,平均70歲。術前否認眼部手術及外傷史,除外角膜病、青光眼、視網膜脫離等眼病,術前眼壓測量均在正常范圍10~21mm Hg。
1.2 方法
術前測量:利用手動角膜曲率計(YZ33,China)、電腦自動驗光儀(Topcon KR-8500,Japan)、角 膜 地 形 圖 儀(Atlas 9000,USA)、IOL-Master(Version3.01,Carl Zeiss Meditec,Germany)分別于術前測量角膜曲率及其他參數。每種儀器各測量3次,選取平均值作為最后測量值。
1.3 統計學方法
利用SPSS15.0統計軟件,統計分析采用配對t檢驗,方差齊性分析和q檢驗,P<0.05為差異有統計學意義。
2 結果
2.1 測量角膜屈光度的比較
四種儀器測量平均、最大及最小角膜屈光力的結果經配對t檢驗及方差分析,差異無統計學意義(P>0.05)。見表1。
表1 四種檢查方法測得的角膜屈光力的統計結果()
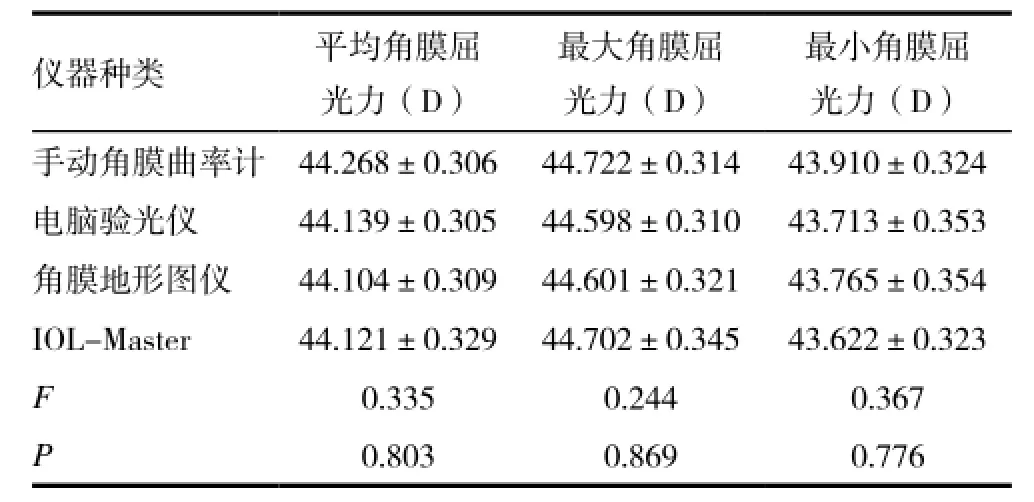
表1 四種檢查方法測得的角膜屈光力的統計結果()
儀器種類 平均角膜屈光力(D)最大角膜屈光力(D)最小角膜屈光力(D)手動角膜曲率計 44.268±0.306 44.722±0.314 43.910±0.324電腦驗光儀 44.139±0.305 44.598±0.310 43.713±0.353角膜地形圖儀 44.104±0.309 44.601±0.321 43.765±0.354 IOL-Master 44.121±0.329 44.702±0.345 43.622±0.323F0.335 0.244 0.367P0.803 0.869 0.776
2.2 測量角膜散光度數及散光軸位的比較
四種儀器對角膜散光度數的測量經統計學分析,差異無統計學意義(P>0.05);測量角膜散光軸位結果,經統計學分析測量結果差異有統計學意義(P<0.01)。見表2。
四種儀器對散光軸位測量的差值,差異均有統計學意義(P<0.01);而后三者儀器間對散光軸位測量結果,兩兩比較均無統計學意義(P>0.05)。見表3。
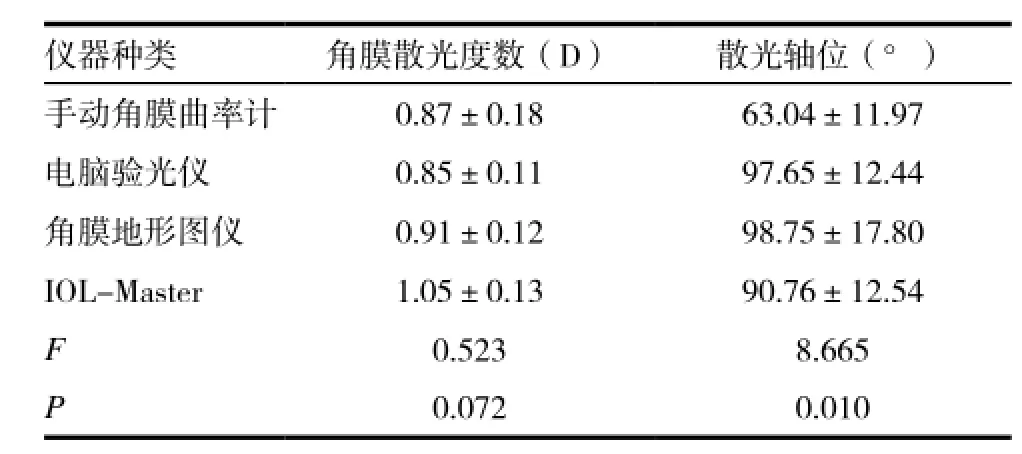
表2 四種檢查方法測得的角膜散光度數及軸位的統計結果
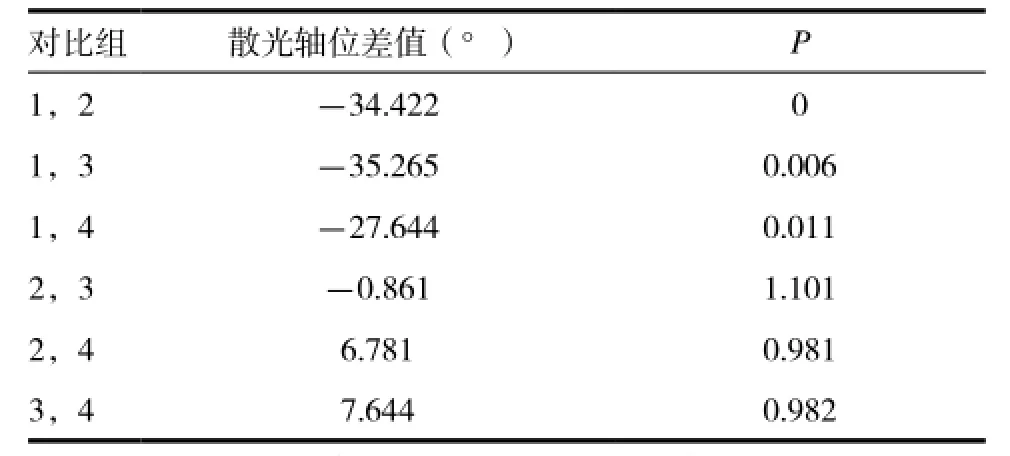
表3 四種檢查方法測得的散光軸位兩兩比較的統計結果
3 討論
角膜曲率檢查是反映眼部屈光狀態的一項重要檢查項目,在臨床應用中起到重要作用[2]。角膜曲率計是用于測量眼球角膜前表面即中心約3mm區域的各條子午線的彎曲度,即曲率半徑及曲率,從而可確定角膜有無散光及散光度和軸向。可以用角膜曲率計檢測散光的度數,軸向及判別散光的類型。對于人工晶體植入術前植入度數的測定以及各種屈光手術的設計與結果分析都需要角膜曲率計的測定。因此對角膜曲率準確測量是保證人工晶體屈光度正確計算的關鍵[3]。
角膜曲率測量儀器品種繁多,其工作原理各具特點:電腦驗光屬于客觀驗光法,其原理與視網膜檢影法基本相同,采用紅外線光源及自動霧視裝置達到放松眼球調節的目的,采用光電技術及自動控制技術檢查屈光度。電腦驗光儀源及自動霧視裝置達到放松眼球調節的目的,采用光電技術及自動控制技術檢查屈光度。能準確測出患者的屈光度數和散光的軸向[4-5]。角膜地形圖是對整個角膜表面進行分析,其中每一投射環上均有256個點計入處理系統,因此,整個角膜就有約7000多個數據點進入分析系統,具有系統性、準確性和精確性。在臨床應用于診斷角膜散光,定量地分析角膜性狀,將角膜屈度以數據或不同的顏色顯示出來,其兩軸屈度之差為角膜散光[6-7]。IOL-Master是利用光學相干原理設計的一種非接觸式的生物測量儀,可用于測量人工晶狀體度數計算需要的角膜曲率、眼軸長度、前房深度和角膜直徑等參數的測量[8-9]。
本研究中,角膜屈光度的測量結果,四種測量儀測得的平均角膜屈光力及最大角膜屈光力、最小角膜屈光力均無顯著差異,可見四種儀器本身具有良好的可重復性[10-11],手動角膜曲率計與電腦自動驗光儀、角膜地形圖儀、IOL-Master三種自動角膜測量儀相比也具有良好的準確性、穩定性,在臨床應用中可以相互替代測量角膜屈光度[12-13]。因此四種角膜曲率測量儀均可用于白內障手術術前測量,在人工晶體屈光度計算中,數據可靠,準確性好。可根據患者眼部的不同情況選擇不同的測量儀器,以求達到準確的測量結果。
[1] Wolffsohn JS,Peterson RC.Anterior ophthalmic imaging[J]. Clin Exp Optom,2006,89(4):205-214.
[2] Lyall DA,Srinivasan S,Ng J,et al.Changes in corneal astigmatism among patients with visually significant cataract[J].Can J Ophthalmol,2014,49(3):297-303.
[3] Ale Magar JB,Cunningham F,Brian G.Comparison of automated and partial coherence keratometry and resulting choice of toric IOL[J].Optom Vis Sci,2013,90(4):385-391.
[4] Chong RS,Sakata LM,Narayanaswamy AK,et al.Relationship between intraocular pressure and angle configuration: an anterior segment OCT study[J].Invest Ophthalmol Vis Sci,2013,54(3):1650-1655.
[5] Engren AL,Behndig A.Anterior chamber depth,intraocular lens position,and refractive outcomes after cataract surgery[J]. J Cataract Refract Surg,2013,39(4):572-577.
[6] Huang J,McAlinden C,Su B,et al.The effect of cycloplegia on the lenstar and the IOLMaster biometry[J]. Optom Vis Sci,2012,89(12):1691-1696.
[7] Hsieh YT,Wang IJ.Intraocular lens power measured by partial coherence interferometry[J]. Optom Vis Sci,2012,89(12):1697-1701.
[8] Ishida Y,Yanai R,Sagara T,et al.Decrease in intraocular pressure following orthokeratology measured with a noncontact tonometer[J].Jpn J Ophthalmol,2011,55(3):190-195.
[9] Hirnschall N,Hoffmann PC,Draschl P,et al.Evaluation of factors influencing the remaining astigmatism after toric intraocular lens implantation[J].J Refract Surg,2014,30(6):394-400.
[10] Ma LW,Xuan D,Li XY,et al.Corneal astigmatism correction with scleral flaps in trans-scleral suture-fixed posterior chamber lens implantation:a preliminary clinical observation[J].Int J Ophthalmol,2011,4(5):502-507.
[11] 柏全豪.眼前節成像與生物測量分析系統的最新進展[J].眼科新進展,2008,28(6):153-156.
[12] Savini G,Barboni P,Carbonelli M,et al.Accuracy of a dual Scheimpflug analyzer and a corneal topography system for intraocular lens power calculation in unoperated eyes[J].J Cataract Refract Surg,2011,37(1):72-76.
[13] Norrby S,Hirnschall N,Nishi Y,et al.Fluctuations in corneal curvature limit predictability of intraocular lens power calculations[J].J Cataract Refract Surg,2013,39(2):174-179.
The accuracy of corneal curvature measured by different types of keratometry
BAI Quanhao1MIAO Yuqing2HU Yueping1ZHANG Gefei1
1. Department of Ophthalmology, the Dalian Municipal Friendship Hospital, Dalian 116001, China; 2. Department of Geriatric Medicine, the Dalian Municipal Friendship Hospital, Dalian 116001, China
ObjectiveWe compared and evaluated the accuracy of the four types of keratometry: manual keratometer, auto-refractometer, corneal topography and IOL-Master for measurement the corneal curvature.MethodsPreoperative measurement of corneal curvature was prospectively obtained in 124 eyes of 86 subjects that underwent phacoemusification with intraocular lens implantation with four types of keratometry. Corneal refractive powers in mean values, corneal refractive powers in maximum axis, corneal refractive powers in minimum axis and the degree of axis were analysized by using SPSS 15.0 in one way ANOVA for statistics.ResultsThere was no significant difference in measuring of the mean corneal refractive powers by using four different types of keratometry (P>0.05). There were also no significant differences in measuring degrees of the corneal refractive powers in maximum axis, corneal refractive powers in minimum axis and corneal astigmatism degree(P> 0.05). But there was significant difference in measuring of the axis values of corneal astigmatism (P<0.01).ConclusionThe accuracy of corneal curvature measured by different types of keratometry is perfect.
Manual keratometer; Auto-refractometer; Corneal topography; IOL-Master; Intraocular lens
R779.66
B
2095-0616(2015)03-211-03
2014-09-29)
猜你喜歡
小學科學(學生版)(2021年5期)2021-07-22 02:40:06
中學生數理化·八年級物理人教版(2019年9期)2019-11-25 07:33:02
中學生數理化·八年級物理人教版(2019年3期)2019-04-25 06:20:54
中學生數理化·八年級物理人教版(2018年3期)2018-05-31 08:52:45
數學小靈通(1-2年級)(2017年10期)2017-11-08 08:39:45
軍事文摘·科學少年(2017年4期)2017-06-20 23:25:16
軍事文摘·科學少年(2017年2期)2017-04-26 21:58:43
中學生數理化·八年級物理人教版(2016年3期)2016-04-07 04:49:32
少兒科學周刊·兒童版(2016年1期)2016-03-14 03:52:21
閱讀與作文(小學低年級版)(2015年4期)2015-04-29 00:00:00