膽紅素水平與急性缺血性腦卒中及其亞型的相關(guān)性
2015-03-04 06:05:31田婷栗靜石正洪關(guān)智媛馮斌
中國康復(fù)理論與實(shí)踐 2015年11期
田婷,栗靜,石正洪,關(guān)智媛,馮斌
膽紅素水平與急性缺血性腦卒中及其亞型的相關(guān)性
田婷1,栗靜1,石正洪1,關(guān)智媛2,馮斌1
[摘要]目的探討膽紅素水平與急性缺血性腦卒中(AIS)發(fā)病、中國缺血性腦卒中亞型(CISS)、卒中嚴(yán)重性及短期預(yù)后的關(guān)系。方法AIS住院患者616例(AIS組),性別和年齡匹配的非腦卒中住院患者664例(對(duì)照組),比較兩組臨床資料并進(jìn)行非條件Logistic回歸分析。對(duì)AIS患者進(jìn)行CISS分型,比較各亞型間膽紅素水平。將AIS患者分為膽紅素升高組和膽紅素正常組,比較兩組入院和出院時(shí)美國國立衛(wèi)生研究院卒中量表(NIHSS)評(píng)分及神經(jīng)功能好轉(zhuǎn)率。結(jié)果AIS組總膽紅素(TBIL)、直接膽紅素(DBIL)、間接膽紅素(IBIL)水平均明顯高于對(duì)照組(P<0.01);Logistic回歸分析顯示,TBIL為AIS的獨(dú)立危險(xiǎn)因素(OR=1.026, 95% CI 1.012~1.041, P<0.001)。CISS各亞型間TBIL、DBIL、IBIL水平均無顯著性差異(P>0.05)。膽紅素升高組入院NIHSS評(píng)分大于正常組(P<0.05);兩組患者出院NIHSS評(píng)分、神經(jīng)功能好轉(zhuǎn)率均無顯著性差異(P>0.05)。結(jié)論AIS患者血清膽紅素升高,與入院時(shí)病情嚴(yán)重程度相關(guān),是AIS發(fā)病的危險(xiǎn)因素;膽紅素水平在CISS亞型間分布無顯著性差異,對(duì)AIS患者短期預(yù)后無明顯影響。
[關(guān)鍵詞]缺血性腦卒中;中國缺血性腦卒中亞型;膽紅素;美國國立衛(wèi)生研究院卒中量表
[本文著錄格式]田婷,栗靜,石正洪,等.膽紅素水平與急性缺血性腦卒中及其亞型的相關(guān)性[J].中國康復(fù)理論與實(shí)踐, 2015, 21(11): 1260-1263.
CITED AS: Tian T, Li J, Shi ZH, et al. Relationship of bilirubin with acuteischemic strokeand Chineseischemic strokesubclassification[J]. Zhongguo Kangfu LilunYu Shijian, 2015, 21(11): 1260-1263.
腦卒中是目前成人致殘的首位病因,同時(shí)是繼缺血性心臟病之后的全球第二位死因[1]。在我國,缺血性腦卒中約占全部腦卒中的70%[2],嚴(yán)重影響居民的生活質(zhì)量。急性缺血性腦卒中(acute ischemic stroke,AIS)具有高的發(fā)病率、病死率及致殘率[3],早期防治AIS是臨床工作的首要任務(wù)。
膽紅素一直被視為血紅蛋白的毒性代謝廢物[4],病理濃度的膽紅素是診斷肝膽疾病的指標(biāo)[5]。近年研究發(fā)現(xiàn),生理濃度膽紅素具有抗氧化及腦保護(hù)作用[6],其與AIS關(guān)系的研究日益增多。多數(shù)研究集中在卒中前狀態(tài)[7-8],且眾多研究并未得出一致結(jié)論[9-11]。
2011年,高山教授提出中國缺血性腦卒中亞型(Chinese ischemic stroke subclassification, CISS)[12],在病情及預(yù)后評(píng)估方面具有很好的應(yīng)用價(jià)值。膽紅素水平與CISS亞型關(guān)系的研究甚少。
本研究針對(duì)膽紅素水平與AIS及CISS的關(guān)系進(jìn)行探討,以期為腦卒中患者準(zhǔn)確評(píng)估病情及預(yù)后提供科學(xué)依據(jù)。
1 資料與方法
1.1一般資料
收集2014年3月~2015年3月在蘭州大學(xué)第二醫(yī)院神經(jīng)內(nèi)科住院治療的AIS患者616例,其中男性371例,女性245例;年齡36~93歲,平均(65.1±11.4)歲;均符合全國第四屆腦血管病學(xué)術(shù)會(huì)議制定的診斷標(biāo)準(zhǔn)[13],經(jīng)頭顱CT或MRI確診。
納入標(biāo)準(zhǔn):①發(fā)病7 d內(nèi)入院,MRI彌散加權(quán)成像(diffusion-weighted imaging, DWI)有新發(fā)缺血病灶;②首次發(fā)病,或既往有腦卒中史但無遺留神經(jīng)功能缺損;③無意識(shí)障礙及抽搐史;④住院時(shí)間≥10 d;⑤有詳細(xì)的人口學(xué)資料。
排除標(biāo)準(zhǔn):①出血性腦卒中或其他腦血管事件;②顱內(nèi)腫瘤、外傷;③嚴(yán)重的肝膽、血液、腎臟、呼吸、心血管系統(tǒng)疾病;④檢驗(yàn)或檢查項(xiàng)目不全。
對(duì)照組664例,為本院同期住院的非腦卒中患者,其中男性376例,女性288例;年齡35~97歲,平均(65.3±10.6)歲。
納入標(biāo)準(zhǔn):①頭顱CT或MRI顯示正常,排除腦卒中;②既往無腦卒中或短暫性腦缺血發(fā)作病史。排除標(biāo)準(zhǔn)與AIS組相同。
兩組患者在性別、年齡、體質(zhì)量等方面無顯著性差異(P>0.05)。見表1。
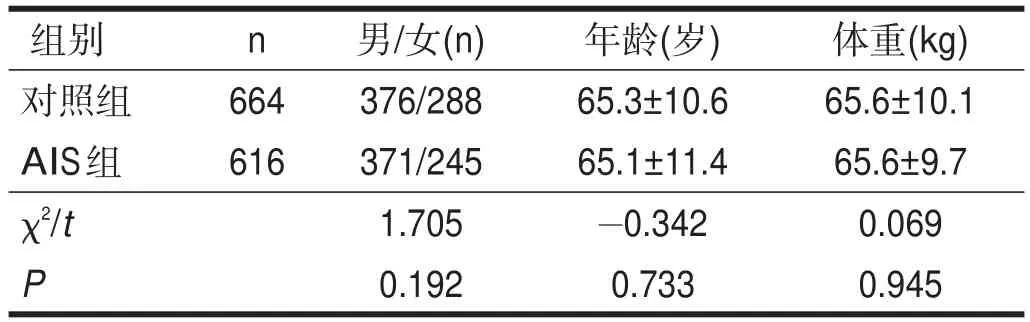
表1 兩組一般資料比較
所有標(biāo)本的收集均經(jīng)患者本人或家屬知情同意。
1.2方法
納入研究的患者入院4 h內(nèi)由專業(yè)神經(jīng)科醫(yī)師詢問病史、記錄人口學(xué)資料,行神經(jīng)系統(tǒng)體格檢查及評(píng)分。
1.2.1樣本采集
所有患者入院當(dāng)天均禁食12 h,于次日清晨空腹肘靜脈采血5 ml,離心后取上層血清,采用Cobas-8000全自動(dòng)生化儀及其配備的試劑(羅氏公司),用釩酸氧化法測(cè)定總膽紅素(total bilirubin, TBIL)和間接膽紅素(indirect bilirubin, IBIL),計(jì)算直接膽紅素(direct bilirubin, DBIL)
DBIL=TBIL-IBIL
線性范圍:1.71~684 μmol/L,批間變異系數(shù)≤5,批內(nèi)變異系數(shù)≤3。
本院TBIL、DBIL、IBIL的正常參考值分別是17.1μmol/L、3.4μmol/L、13.7μmol/L。
1.2.2分組與分型
AIS組患者以TBIL≥17.1 μmol/L,DBIL≥3.4 μmol/L,IBIL≥13.7 μmol/L為界,滿足其中一項(xiàng)者為膽紅素升高組;其余AIS患者為膽紅素正常組。
根據(jù)CISS標(biāo)準(zhǔn),將AIS患者分成5型:大動(dòng)脈粥樣硬化型(largeartery atherosclerosis, LAA)、穿支動(dòng)脈疾病(penetrating artery disease, PAD)、心源性卒中(cardiogenic stroke, CS)、其他病因(other etiology, OE)、病因不確定(undeterminedetiology, UE)。
1.2.3神經(jīng)功能缺損程度及療效評(píng)定
采用美國國立衛(wèi)生研究院卒中量表(National Institute of Health Stroke Scale, NIHSS)評(píng)定AIS患者入院及出院時(shí)神經(jīng)功能缺損程度,NIHSS評(píng)分越高則神經(jīng)功能缺損越嚴(yán)重;計(jì)算AIS患者出院時(shí)神經(jīng)功能好轉(zhuǎn)率。
分型和評(píng)分均由專業(yè)神經(jīng)科醫(yī)師在未知患者膽紅素水平的情況下完成。
1.3統(tǒng)計(jì)學(xué)分析
采用SPSS19.0軟件進(jìn)行統(tǒng)計(jì)分析。計(jì)量資料以(xˉ±s)表示,兩組間比較采用獨(dú)立樣本t檢驗(yàn),多組間的比較用單因素方差分析。計(jì)數(shù)資料以例數(shù)或百分比表示,組間比較采用χ2檢驗(yàn)。以單因素分析有顯著性差異的項(xiàng)目為自變量,AIS為因變量,進(jìn)行非條件Logistic回歸分析,采用向前法。顯著性水平α=0.05。
2 結(jié)果
2.1單因素分析
對(duì)AIS組和對(duì)照組11項(xiàng)臨床資料進(jìn)行分析,結(jié)果顯示AIS組高血壓、糖尿病、房顫、吸煙、飲酒的發(fā)生率及收縮壓、舒張壓、TBIL、DBIL、IBIL水平均高于對(duì)照組(P<0.05);兩組間冠心病的發(fā)病率無顯著性差異(P>0.05)。見表2。
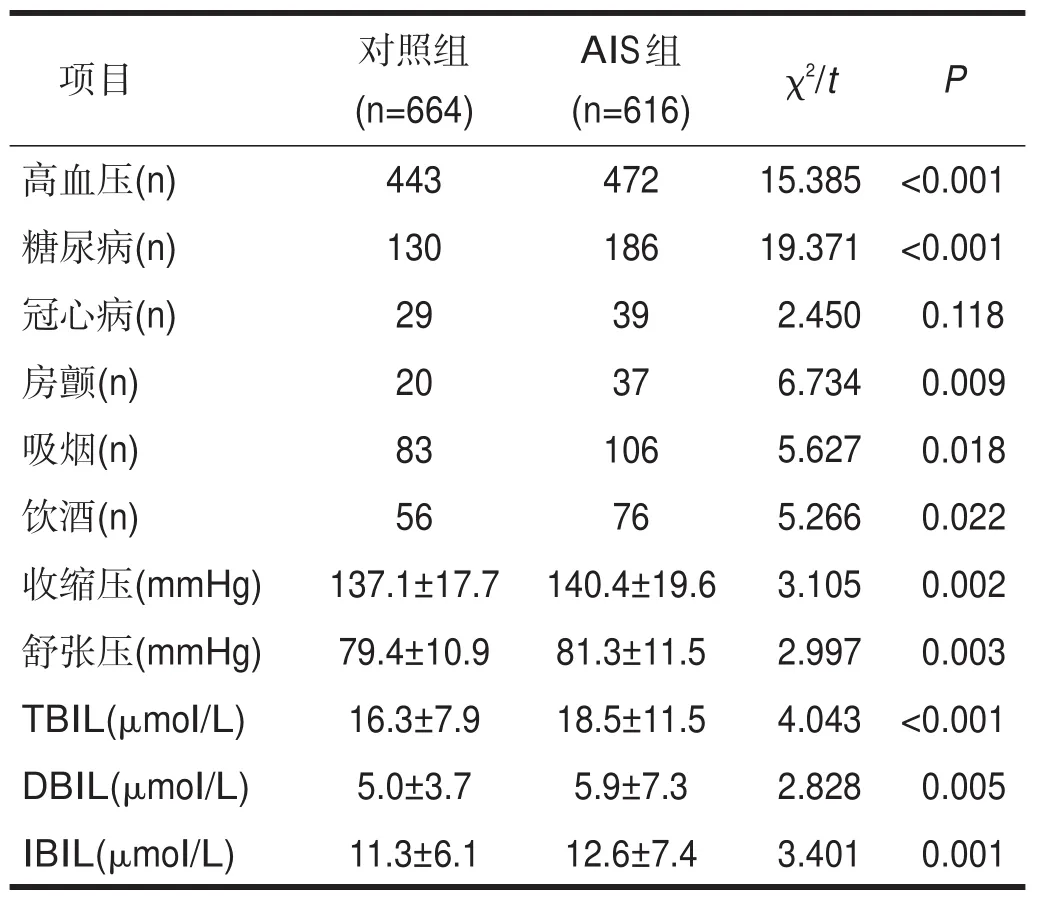
表2 AIS組和對(duì)照組單因素分析結(jié)果
2.2回歸分析
校正吸煙、高血壓、糖尿病、房顫等傳統(tǒng)危險(xiǎn)因素后,TBIL仍為AIS的獨(dú)立危險(xiǎn)因素(P<0.001)。見表3。
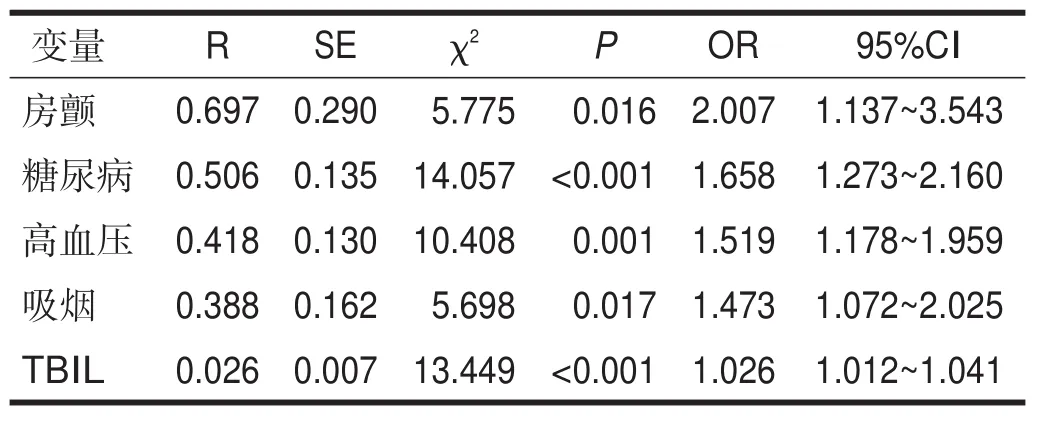
表3 AIS危險(xiǎn)因素的Logistic回歸分析結(jié)果
2.3CISS亞型間膽紅素水平
616例AIS患者中,LAA型304例,PAD型140例,CS型74例,OE型43例,UE型55例。CISS各亞型間TBIL、DBIL、IBIL水平均無顯著性差異(P> 0.05)。見表4。
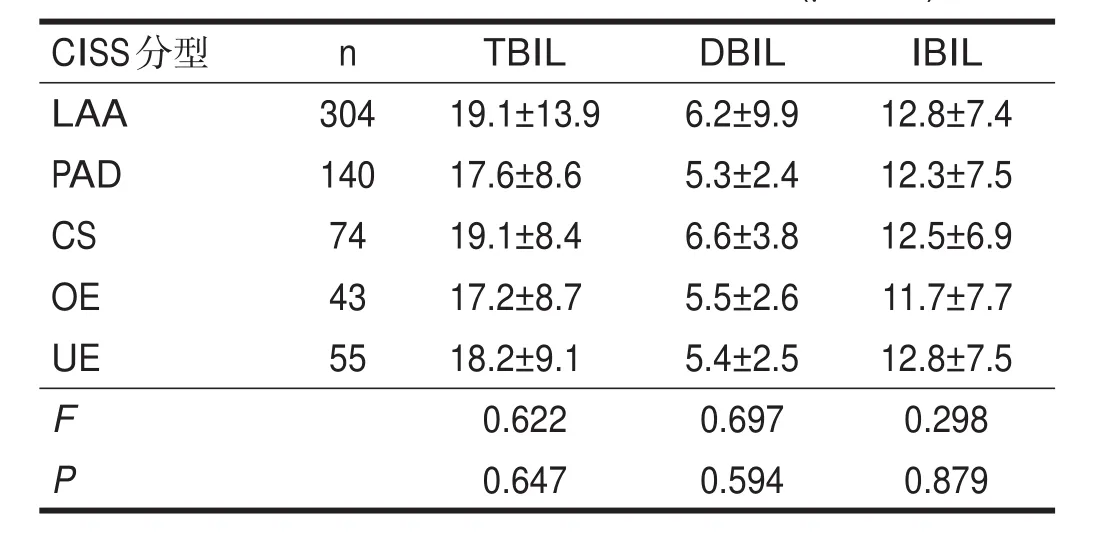
表4 不同CISS亞型間膽紅素水平比較(μmol/L)
2.4不同膽紅素水平NIHSS評(píng)分比較
膽紅素升高組入院NIHSS評(píng)分大于膽紅素正常組(P<0.05);兩組出院NIHSS評(píng)分、神經(jīng)功能好轉(zhuǎn)率均無顯著性差異(P>0.05)。見表5。
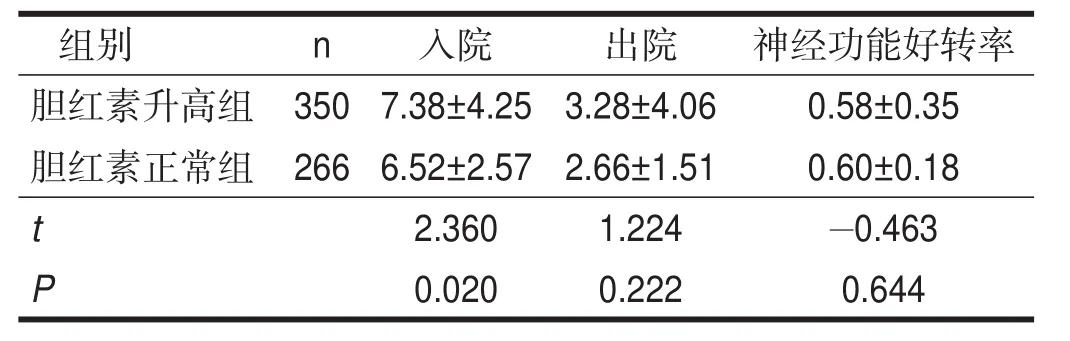
表5 膽紅素升高組與膽紅素正常組NIHSS評(píng)分比較
3 討論
氧化應(yīng)激介導(dǎo)的腦功能和結(jié)構(gòu)損傷貫穿于整個(gè)AIS過程,在早期扮演著重要的病理損傷角色[14]。膽紅素由血紅素加氧酶(heineoxygenase, HO)分解衰老的紅細(xì)胞產(chǎn)生[15]。近年研究發(fā)現(xiàn),不同類型膽紅素均是有效的抗氧化劑,在清除超氧自由基、保護(hù)腦功能方面發(fā)揮重要作用[16]。
本研究發(fā)現(xiàn),高血壓、糖尿病、房顫、吸煙、飲酒、收縮壓、舒張壓、TBIL、DBIL、IBIL是AIS的危險(xiǎn)因素;在調(diào)整傳統(tǒng)的危險(xiǎn)因素高血壓、糖尿病、房顫、吸煙的影響后,TBIL是AIS獨(dú)立的危險(xiǎn)因素。
本研究排除嚴(yán)重肝膽、血液系統(tǒng)疾病對(duì)膽紅素水平的影響,可以認(rèn)為膽紅素升高是由于腦卒中發(fā)生后,為對(duì)抗其損傷而激活一系列抗氧化應(yīng)激級(jí)聯(lián)反應(yīng)的結(jié)果,是機(jī)體對(duì)卒中的一種防御反應(yīng)。與以往研究基本一致[10,17-18]。
AIS患者血清膽紅素水平高于對(duì)照組,可能的機(jī)制考慮如下。①膽紅素是人體內(nèi)最強(qiáng)的內(nèi)源性抗氧化劑[19],應(yīng)激狀態(tài)下,HO的表達(dá)增加,其誘導(dǎo)產(chǎn)生的膽紅素含量增加[15]。②膽紅素能減少脂類生成自由基;也能直接與氧自由基結(jié)合,進(jìn)而清除自由基,保護(hù)血管內(nèi)皮細(xì)胞免受氧化應(yīng)激損傷[16]。③膽紅素能增強(qiáng)其他抗氧化劑的功能,達(dá)到保護(hù)組織和器官的作用[20]。④升高的膽紅素對(duì)其限速酶HO具有正性調(diào)節(jié)作用,使HO含量增加,而HO本身具有抗氧化及腦保護(hù)作用[21]。⑤膽紅素能上調(diào)細(xì)胞攝取糖的能力,增加腦組織對(duì)糖的利用,從而起到保護(hù)腦功能的作用[22]。
本研究顯示,CISS各型間TBIL、DBIL、IBIL水平無顯著性差異,盡管CS型和LAA型膽紅素水平有升高的趨勢(shì)。提示AIS后膽紅素的升高與CISS分型無顯著相關(guān)性。
為進(jìn)一步研究膽紅素水平與AIS患者病情及預(yù)后的關(guān)系,對(duì)AIS膽紅素升高組與膽紅素正常組NIHSS評(píng)分進(jìn)行分析,結(jié)果顯示,高膽紅素水平與AIS患者入院時(shí)神經(jīng)功能缺損的嚴(yán)重程度相關(guān),而與AIS的短期預(yù)后無關(guān)。Xu等[10]、Pineda等[18]的研究結(jié)果也證實(shí)這一點(diǎn)。這可能是由于在應(yīng)激狀態(tài)下,膽紅素水平處于正性調(diào)節(jié)的范圍[23],腦損傷越嚴(yán)重,神經(jīng)功能缺損越嚴(yán)重,氧化應(yīng)激越強(qiáng)烈,誘導(dǎo)機(jī)體產(chǎn)生的膽紅素水平越高;此外,氧化應(yīng)激減少體內(nèi)抗氧化物質(zhì)的含量,促使膽紅素的合成增加[24]。應(yīng)激性激素的分泌也可促使膽紅素水平升高[25]。以上研究表明,膽紅素水平在一定程度上與氧化應(yīng)激的程度相關(guān),也反映卒中的嚴(yán)重性。因此,對(duì)膽紅素升高的患者應(yīng)盡早開展積極治療,預(yù)防卒中進(jìn)展,改善卒中預(yù)后。
另外,研究不支持以膽紅素水平預(yù)測(cè)卒中預(yù)后,這與Xu等的研究結(jié)果一致[10]。其機(jī)制可能是該濃度下,膽紅素的保護(hù)作用難以扭轉(zhuǎn)卒中對(duì)神經(jīng)功能造成的損傷,加之過于強(qiáng)烈的氧化應(yīng)激對(duì)機(jī)體也有損害作用,致使急性期腦卒中患者的神經(jīng)功能缺損并未見明顯改善。Kurzepa等研究發(fā)現(xiàn),血清膽紅素升高是AIS急性期及卒中3個(gè)月后預(yù)后不良的因素[9]。而Perlstein等的大樣本回顧性研究顯示,膽紅素水平與AIS患者預(yù)后良好呈正相關(guān),并指出TBIL每升高0.1 mg/dl,預(yù)后不良的概率減少10%[11]。以上研究結(jié)果不同的原因可能與樣本的選取、卒中發(fā)生時(shí)神經(jīng)功能缺損程度、評(píng)估預(yù)后的時(shí)間及人口構(gòu)成差異有關(guān)。
本研究顯示,AIS患者膽紅素水平升高,且與入院時(shí)腦卒中嚴(yán)重性呈正相關(guān);在CISS亞型間的分布無顯著差異,對(duì)短期神經(jīng)功能好轉(zhuǎn)率無明顯影響。
膽紅素作為一種快速、有效的檢測(cè)指標(biāo),在一定程度上可以預(yù)測(cè)AIS的發(fā)生及嚴(yán)重程度。但目前對(duì)于不同類型膽紅素發(fā)揮抗氧化作用的具體機(jī)制及強(qiáng)弱程度尚未完全闡明,膽紅素的臨床意義仍需多中心、大樣本、前瞻性研究進(jìn)一步探索。
[參考文獻(xiàn)]
[1] WHO. The Top 10 Causes of Death [R]. Geneva, Switzerland: World Healthorganization, 2008.
[2]中華醫(yī)學(xué)會(huì)神經(jīng)病學(xué)分會(huì)腦血管病學(xué)組急性缺血性腦卒中診治指南撰寫組.中國急性缺血性腦卒中診治指南2010[J].中華神經(jīng)科雜志, 2010, 43(2): 1-8.
[3] Linfante I, Walker GR, Castonguay AC, et al. Predictorsof mortality in acuteischemic strokeintervention: analysisof theNorthAmerican SolitaireAcuteStrokeRegistry [J]. Stroke, 2015, 46(8): 2305-2308.
[4] Zahir F, Rabbani G, Khan RH, et al. The pharmacological features of bilirubin: the question of the century [J]. Cell Mol Biol Lett, 2015, 20 (3): 418-447.
[5] Lee M, Kim W, Choi Y, et al. Spontaneousevolution in bilirubin levels predicts liver-related mortality in patients with alcoholic hepatitis [J]. PLoSOne, 2014, 9(7): e100870.
[6] Dennery PA. Evaluating the beneficial and detrimental effects of bile pigmentsinearly andlater life[J]. Front Pharmacol, 2012, 3: 115.
[7] Oda E, Kawai R. A possible cross-sectional association of serum total bilirubin with coronary heart disease and stroke in a Japanese health screeningpopulation[J]. Heart Vessels, 2012, 27(1): 29-36.
[8] Kimm H, Yun JE, Jo J, et al. Low serum bilirubin level as an independent predictor of stroke incidence: a prospective study in Korean men andwomen[J]. Stroke, 2009, 40(11): 3422-3427.
[9] Kurzepa J, Bielewicz J, Stelmasiak Z, et al. Serum bilirubin and acid levelsasthebad prognostic factorsin theischemic stroke[J]. Int JNeurosci, 2009, 119(12): 2243-2249.
[10] Xu T, Zhang J, Xu T, et al. Association of serum bilirubin with stroke severity andclinical outcomes[J]. Can JNeurol Sci, 2013, 40(1): 80-84.
[11] Perlstein TS, Pande RL, Creager MA, et al. Serum total bilirubin level, prevalent stroke, and stroke outcomes: NHANES 1999-2004 [J]. Am J Med, 2008, 121(9): 781-788.
[12] Gao S, Wang YJ, Xu AD, et al. Chineseischemic strokesubclassification[J]. Front Neurol,2011, 2: 6.
[13]中華神經(jīng)科學(xué)會(huì),中華神經(jīng)外科學(xué)會(huì).各類腦血管疾病診斷要點(diǎn)[J].中華神經(jīng)科雜志, 1996, 29(6): 379-381.
[14] NiizumaK, Endo H, Chan PH. Oxidativestressand mitochondrial dysfunction as determinants of ischemic neuronal death and survival [J]. J Neurochem, 2009, 109(Suppl 1): 133-138.
[15] Müllebner A, Moldzio R, Redl H, et al. Hemedegradation by hemeoxygenase protects mitochondria but induces ER stress via formed bilirubin[J]. Biomolecules, 2015, 5(2): 679-701.
[16] Fereshtehnejad SM, Poorsattar Bejeh Mir K, Poorsattar Bejeh Mir A, et al. Evaluation of the possible antioxidative role of bilirubin protecting from free radical related illnesses in neonates [J]. Acta Med Iran, 2012, 50(3): 153-163.
[17] Luo Y, Li J, Zhang J, et al. Elevated bilirubin after acute ischemic strokelinked to thestrokeseverity [J]. Int JDev Neurosci, 2013, 31(7): 634-638.
[18] Pineda S, Bang OY, Saver JL, et al. Association of serum bilirubin with ischemic stroke outcomes [J]. J Stroke Cerebrovasc Dis, 2008, 17 (3): 147-152.
[19] Liao SL. The role of bilirubin and phototherapy in the oxidative/antioxidant balance[J]. Pediatr Neonatol, 2015, 56(2): 77-78.
[20] Siow RC, Sato H, Leake DS, et al. Vitamin C protects human arterial smooth musclecellsagainst atherogenic lipoproteins: effectsof antioxidant vitamins C and E on oxidized LDL-induced adaptive increases in cystine transport and glutathione [J]. Arterioscler Thromb Vasc Bio, 1998, 18(10): 1662-1670.
[21] Qi D, Ouyang C, Wang Y, et al. HO-1 attenuateshippocampal neurons injury viatheactivation of BDNF-TrkB-PI3K/Akt signaling pathway in stroke[J]. Brain Res, 2014, 1577: 69-76.
[22] Cohen G, Livovsky DM, Kapitulnik J, et al. Bilirubin increasestheexpression of glucose transporter-1 and the rate of glucose uptake in vascular endothelial cells[J]. Rev Diabet Stud, 2006, 3(3): 127-133.
[23] Vítek L. Relationship of bilirubin to diseasescaused by increased oxidativestress[J]. Vnitr Lek, 2013, 59(7): 618-621.
[24] Cui W, Fu G, Wu H, et al. Cadmium-induced hemeoxygenase-1 gene expression isassociated with thedepletion of glutathionein therootsof Medicagosativa[J]. Biometals, 2011, 24(1): 93-103.
[25] Grion N, Repetto EM, Pomeraniec Y, et al. Induction of nitric oxide synthase and heme oxygenase activities by endotoxin in the rat adrenal cortex: involvement of both signaling systems in the modulation of ACTH-dependent steroid production [J]. J Endocrinol, 2007, 194(1): 11-20.
·專題·
作者單位:1.蘭州大學(xué)第二醫(yī)院神經(jīng)內(nèi)科,甘肅蘭州市730000;2.蘭州大學(xué)第二臨床醫(yī)學(xué)院,甘肅蘭州市730000。作者簡(jiǎn)介:田婷(1989-),女,漢族,甘肅白銀市人,碩士研究生,主要研究方向:腦血管病。通訊作者:石正洪(1966-),女,漢族,博士,教授,主任醫(yī)師,碩士研究生導(dǎo)師,主要研究方向:腦血管病。E-mail: lzuszh@163.com。
Relationshipof BilirubinwithAcuteIschemicStrokeand ChineseIschemicStrokeSubclassification
TIANTing1, LI Jing1, SHI Zheng-hong1, GUANZhi-yuan2, FENGBin1
1. Department of Neurology, theSecond Hospital, Lanzhou University, Lanzhou, Gansu 730000, China;2. TheSecond School of Clinical Medicine, Lanzhou University, Lanzhou, Gansu730000, China
Abstract:Objective To investigate the relationship of the serum bilirubin level with acute ischemic stroke (AIS), and Chinese ischemic strokesubclassification (CISS), strokeseverity and short-term outcomeof AISpatients. Methods616 patientswith AISaswell as664 patientswithout strokematched with gender and agewerecompared and analyzed with thenon-conditional Logistic regression. TheAISpatientsweredivided based on theCISS, and their bilirubin levelswerecompared. TheAISpatientsweredivided into high bilirubin group and normal bilirubin group, their scores of the National Institute of Health Stroke Scale (NIHSS) as admission and discharge, and neural function improvement rate were compared. Results The levels of total bilirubin (TBIL), direct bilirubin (DBIL) and indirect bilirubin (IBIL) werehigher in theAISgroup than in thecontrol group (P<0.01), and the TBIL wastheindependent risk factorsof AIS(OR=1.026, 95%CI 1.012-1.041, P<0.001). Therewasno significant differenceof thelevelsof TBIL, DBIL and IBIL among thepatientsof CISS(P>0.05). The NIHSS score was higher in the high bilirubin group than in the normal bilirubin group as admission (P<0.05), but it was not significant as discharge (P>0.05), nor the rate of neural function improvement (P>0.05). Conclusion The serum bilirubin level elevated and correlated with the severity in the AIS patients, which might be the risk of pathogenesis and AIS. The bilirubin was not various with the CISS, and might belessinvolvedintheshort-termoutcomeof AIS.
Keywords:ischemicstroke; Chineseischemicstrokesubclassification; bilirubin; National Instituteof Health StrokeScale
(收稿日期:2015-07-30修回日期:2015-08-27)
基金項(xiàng)目:蘭州科技計(jì)劃項(xiàng)目(No.2011-1-134)。
DOI:10.3969/j.issn.1006-9771.2015.11.005
[中圖分類號(hào)]R743.3
[文獻(xiàn)標(biāo)識(shí)碼]A
[文章編號(hào)]1006-9771(2015)11-1260-04
猜你喜歡
體育科技文獻(xiàn)通報(bào)(2022年3期)2022-05-23 13:46:54
美與時(shí)代·美術(shù)學(xué)刊(2022年3期)2022-04-27 01:18:15
天津外國語大學(xué)學(xué)報(bào)(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
科技傳播(2019年22期)2020-01-14 03:06:54
火花(2019年12期)2019-12-26 01:00:28
民用飛機(jī)設(shè)計(jì)與研究(2019年4期)2019-05-21 07:21:24
人大建設(shè)(2019年12期)2019-05-21 02:55:32
汽車工程學(xué)報(bào)(2017年2期)2017-07-05 08:13:02
學(xué)苑創(chuàng)造·A版(2015年11期)2016-01-14 09:03:27