急性呼吸窘迫綜合征機械通氣患者呼出氣冷凝液中過氧化氫和白介素6水平變化及其臨床意義研究
2015-03-23 05:34:59牛毓茜楊國輝
實用心腦肺血管病雜志 2015年3期
牛毓茜,楊國輝
·論著·
急性呼吸窘迫綜合征機械通氣患者呼出氣冷凝液中過氧化氫和白介素6水平變化及其臨床意義研究
牛毓茜,楊國輝
目的探討急性呼吸窘迫綜合征(ARDS)機械通氣患者呼出氣冷凝液(EBC)中過氧化氫(H2O2)和白介素6(IL-6)水平變化及其臨床意義。方法選取2012年9月—2013年12月貴陽醫(yī)學院附屬醫(yī)院內(nèi)科重癥監(jiān)護病房(MICU)收治的ARDS患者42例,均經(jīng)氣管插管或氣管切開進行機械通氣治療。按患者入住MICU兩周后轉歸分為存活組22例和死亡組20例,比較兩組患者機械通氣后1、3、5、7 d急性生理學及慢性健康狀況(APACHE)Ⅱ評分、APACHEⅢ評分及EBC中H2O2、IL-6水平,分析兩組患者機械通氣后1、3、5、7 d APACHEⅡ評分、APACHEⅢ評分與EBC中H2O2、IL-6水平的相關性。結果(1)存活組患者機械通氣后3、5、7 d EBC中H2O2和IL-6水平低于機械通氣后1 d,死亡組患者機械通氣后7 d EBC中H2O2和IL-6水平高于機械通氣后1、3、5 d(P<0.05)。(2)機械通氣后1 d兩組患者APACHEⅡ和APACHEⅢ評分比較,差異無統(tǒng)計學意義(P>0.05);機械通氣后3、5、7 d死亡組患者APACHEⅡ和APACHEⅢ評分高于存活組(P<0.05)。(3)械通氣后1、3 d兩組患者EBC中H2O2和IL-6水平比較,差異無統(tǒng)計學意義(P>0.05);機械通氣后5、7 d死亡組患者EBC中H2O2和IL-6水平均高于存活組(P<0.05)。(4)存活組患者機械通氣后不同時間點EBC中H2O2和IL-6水平與APACHEⅡ和APACHEⅢ評分間無直線相關關系(P>0.05);死亡組患者機械通氣后5、7 d EBC中H2O2水平與APACHEⅡ和APACHEⅢ評分呈正相關,EBC中IL-6水平與APACHEⅡ和APACHEⅢ評分呈負相關(P<0.05)。結論ARDS機械通氣患者EBC中H2O2和IL-6水平均升高,且與病情嚴重程度相關,其可作為氣道炎性反應的監(jiān)測指標,結合APACHE評分可為評估患者預后提供參考。
呼吸窘迫綜合征,成人;呼吸,人工;呼出氣冷凝液;過氧化氫;白介素6
牛毓茜,楊國輝.急性呼吸窘迫綜合征機械通氣患者呼出氣冷凝液中過氧化氫和白介素6水平變化及其臨床意義研究[J].實用心腦肺血管病雜志,2015,23(3):25-28.[www.syxnf.net]
Niu YQ,Yang GH.Changes and clinical significances of hydrogen peroxide and interleukin-6 levels in exhaled breath condensate of patients with acute respiratory distress syndrome treated with mechanical ventilation[J].Practical Journal of Cardiac Cerebral Pneumal and Vascular Disease,2015,23(3):25-28.
機械通氣是搶救急性呼吸窘迫綜合征(ARDS)患者生命的重要措施[1]。ARDS常因感染、低氧血癥和不適當?shù)臋C械通氣而導致機體氧化應激,從而引起氧化應激產(chǎn)物和細胞因子水平升高[2]。而氧化應激在ARDS發(fā)病過程中起重要作用,其產(chǎn)物及細胞因子可損傷全身臟器,目前認為其可能是引起多臟器損傷和多器官功能衰竭的重要原因。近年來,檢測呼出氣冷凝液(exhaled breath condensate,EBC)越來越受到國內(nèi)外研究者的重視,其具有無創(chuàng)、實時、可重復性收集等優(yōu)點,由于標本直接來源于下氣道,因此結果真實可靠;且收集EBC無年齡限制,尤其適用于氣管插管和氣管切開的危重癥患者[3-4]。目前,國內(nèi)外關于ARDS患者EBC中氧化應激產(chǎn)物和細胞因子變化的研究報道較少。為此,本研究檢測了ARDS機械通氣患者EBC中過氧化氫(H2O2)和白介素6(IL-6)水平變化,并探討其臨床意義。
1 資料與方法
1.1 入選標準根據(jù)2012年ARDS柏林定義[5]制定納入標準:(1)存在發(fā)生ARDS的高危因素;(2)發(fā)病1周內(nèi);(3)需要正壓機械通氣治療;(4)具有嚴重氧合障礙,即在吸入氧濃度(FiO2)為1.00、呼氣末正壓(PEEP)≥5 cm H2O(1 cm H2O=0.098 kPa)的情況下,氧合指數(shù)(PaO2/FiO2)≤300 mm Hg(1 mm Hg =0.133 kPa);(5)胸片示雙肺浸潤影,無法用積液、肺不張或結節(jié)解釋。排除標準:(1)年齡<18歲;(2) 1周內(nèi)曾發(fā)生急性心肌梗死(AMI);(3)心力衰竭; (4)妊娠;(5)支氣管胸膜瘺、氣胸或2周內(nèi)曾行肺葉切除術;(6)合并神經(jīng)肌肉疾病或顱內(nèi)壓增高;(7)嚴重慢性呼吸系統(tǒng)疾病;(8)慢性肝臟疾病;(9)骨髓移植;(10)惡性疾病或慢性疾病終末期。
1.2 一般資料選取2012年9月—2013年12月貴陽醫(yī)學院附屬醫(yī)院內(nèi)科重癥監(jiān)護病房(MICU)收治的符合入選條件的ARDS患者42例,均經(jīng)氣管插管或氣管切開進行機械通氣治療,其中男28例,女14例;年齡30~71歲,平均(58.5±18.4)歲。按患者入住MICU兩周后轉歸分為存活組22例和死亡組20例,存活組患者中男16例,女6例;年齡30~65歲,平均(57.5 ±17.4)歲;原發(fā)疾病:肺炎12例,多發(fā)傷6例,全身感染3例,術后大出血1例。死亡組患者中男12例,女8例;年齡35~71歲,平均(58.7±19.2)歲;原發(fā)疾病:肺炎10例,多發(fā)傷5例,全身感染3例,術后大出血2例。兩組患者性別、年齡及原發(fā)疾病間具有均衡性。本研究遵循貴陽醫(yī)學院附屬醫(yī)院制定的相關倫理學標準,并得到該委員會批準。入選研究對象均由患者家屬簽署知情同意書。
1.3 研究方法比較兩組患者機械通氣后1、3、5、7 d急性生理學及慢性健康狀況(APACHE)Ⅱ評分和APACHEⅢ評分及EBC中H2O2和IL-6水平。并分別分析兩組患者機械通氣后1、3、5、7 d APACHEⅡ評分和APACHEⅢ評分與EBC中H2O2和IL-6水平的相關性。
1.3.1 APACHEⅡ評分和APACHEⅢ評分分別記錄患者性別、年齡、體溫、血壓、心率、呼吸頻率、吸入氧濃度(FiO2)、動脈血氣分析相關指標(動脈血氧分壓、動脈血二氧化碳分壓、pH值)、血細胞比容、白細胞計數(shù)、腎功能、肝功能、血鈉、血鉀、血糖、格拉斯哥昏迷量表評分、原發(fā)慢性疾病、入住MICU主要原因等,所有生理指標取24 h內(nèi)最差值。
1.3.2 收集EBC參照文獻[2]設計外觀類似葫蘆形狀的雙向開口EBC玻璃收集器,裝入充滿冰水混合物的有機玻璃器皿中。EBC玻璃收集器兩端分別接入呼吸機呼氣端管道替代蓄水罐,持續(xù)20 min收集EBC。接入呼吸機呼氣端前應關掉濕化瓶溫度開關,并清除呼吸機管道內(nèi)液體以防其進入EBC玻璃收集器,造成標本污染。待標本收集完畢,檢測EBC總量,并進行分裝,立即放置于冰箱保存(-80℃),留待同批檢測。
1.3.3 H2O2的測定取EBC標本250 μl,采用化學熒光法檢測H2O2。高香草酸(homovanillic acid,HVA)、辣根過氧化酶(horsheradish peroxidase,HRP)均購自Sigma公司(美國);標準H2O2溶液購自北京某試劑公司。建立直線回歸方程時,需依據(jù)標準H2O2溶液水平(0.14~2.21 μmol/L)及其熒光強度(實測值與空白對照值的差值)繪制標準曲線,通過直線回歸方程與熒光強度計算H2O2水平,同一份樣品分別檢測3次,取平均值。
1.3.4 IL-6的測定采用酶聯(lián)免疫吸附試驗(ELISA)檢測IL-6,試劑盒購自Cayman公司(美
國)。依據(jù)標準樣品測定的吸光度(A)值繪制標準曲線,并采用曲線擬合法求出直線回歸方程,再根據(jù)各待測樣本A值計算EBC中IL-6水平。
1.4 統(tǒng)計學方法應用SPSS 19.0統(tǒng)計學軟件進行數(shù)據(jù)處理,計量資料以(x±s)表示,組間比較采用兩獨立樣本t檢驗,組內(nèi)比較采用配對t檢驗;相關性分析采用Pearson相關分析。以P<0.05為差異有統(tǒng)計學意義。
2 結果
2.1 APACHEⅡ和APACHEⅢ評分機械通氣后1 d兩組患者APACHEⅡ和APACHEⅢ評分比較,差異無統(tǒng)計學意義(P>0.05);機械通氣后3、5、7 d死亡組患者APACHEⅡ和APACHEⅢ評分高于存活組,差異有統(tǒng)計學意義(P<0.05,見表1)。
2.2 EBC中H2O2和IL-6水平存活組患者機械通氣后3、5、7 d EBC中H2O2和IL-6水平低于機械通氣后1 d,死亡組患者機械通氣后7 d EBC中H2O2和IL-6水平高于機械通氣后1、3、5 d(P<0.05)。機械通氣后1、3 d兩組患者EBC中H2O2和IL-6水平比較,差異無統(tǒng)計學意義(P>0.05);機械通氣后5、7 d死亡組患者EBC中H2O2和IL-6水平均高于存活組,差異有統(tǒng)計學意義(P<0.05,見表2)。
2.3 相關性分析存活組患者機械通氣后不同時間點EBC中H2O2和IL-6水平與APACHEⅡ和APACHEⅢ評分間無直線相關關系(P>0.05);死亡組患者機械通氣后5、7 d EBC中H2O2水平與APACHEⅡ和APACHEⅢ評分呈正相關(P<0.05);EBC中IL-6水平與APACHEⅡ和APACHEⅢ評分呈負相關(P<0.05,見表3)。
表1 兩組患者機械通氣后不同時間點APACHEⅡ和APACHEⅢ評分比較(±s,分)Table 1 Comparison of APACHEⅡscore and APACHEⅢscore between the two groups at different time points after mechanical ventilation

表1 兩組患者機械通氣后不同時間點APACHEⅡ和APACHEⅢ評分比較(±s,分)Table 1 Comparison of APACHEⅡscore and APACHEⅢscore between the two groups at different time points after mechanical ventilation
注:APACHE=急性生理學及慢性健康狀況;與機械通氣后1 d比較,*P<0.05;與機械通氣后3 d比較,△P<0.05;與機械通氣后5 d比較,▲P<0.05
1 d3 d5 d7 d存活組2222.56±8.2617.86±6.30*12.45±6.48*11.24±5.67*△60.85±16.2351.84±16.68*40.35±13.66*37.29±12.15組別例數(shù)APACHEⅡ評分APACHEⅢ評分1 d3 d5 d7 d *死亡組2021.23±4.6726.54±8.28*33.36±6.45*△42.08±6.24*△▲59.92±15.0175.38±11.69*89.12±13.98*△118.57±18.14*△t 001 0.911.345.9213.08 P值0.0610.0480.022<0.0050.0810.0330.018<0.值1.261.464.3310.03*
表2 兩組患者機械通氣后不同時間點EBC中H2O2和IL-6水平比較(±s)Table 2 Comparison of H2O2and IL-6 levels in EBC between the two groups at different time points after mechanical ventilation

表2 兩組患者機械通氣后不同時間點EBC中H2O2和IL-6水平比較(±s)Table 2 Comparison of H2O2and IL-6 levels in EBC between the two groups at different time points after mechanical ventilation
注:H2O2=過氧化氫,IL-6=白介素6;與機械通氣后1 d比較,*P<0.05;與機械通氣后3 d比較,△P<0.05;與機械通氣后5 d比較,▲P<0.05
1 d3 d5 d7 d存活組220.18±0.130.12±0.03*0.08±0.03*0.05±0.02*△14.66±6.1211.03±2.28*10.48±2.12*6.58±2.07組別例數(shù)H2O2(μmol/L)IL-6(ng/L) 1 d3 d5 d7 d*△死亡組200.15±0.030.17±0.040.24±0.140.35±0.15*△▲12.88±5.2313.25±3.1215.95±4.3619.18±4.19*△▲t 0.931.815.1712.031.081.928.8215.11 P值0.0790.0520.0290.0020.0930.0710.0110.002值
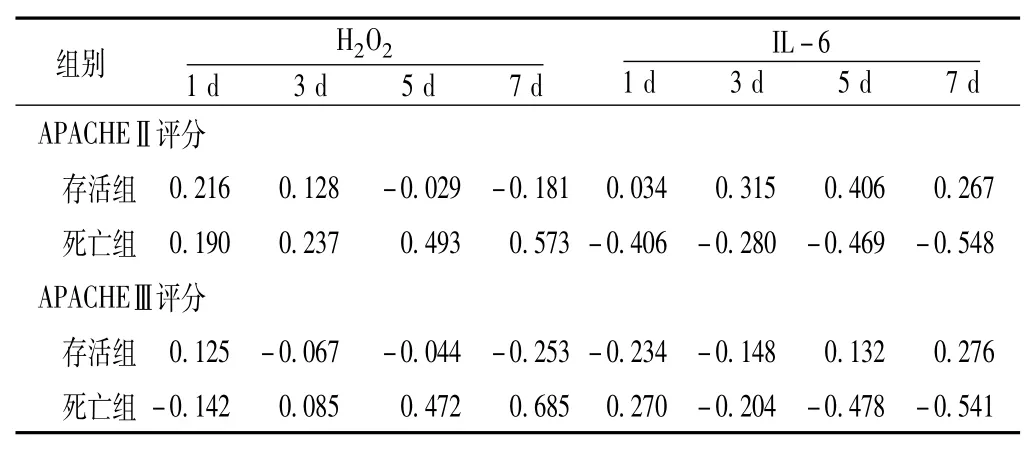
表3 兩組患者不同時間點APACHEⅡ和APACHEⅢ評分與EBC中H2O2和IL-6水平的相關性分析(r值)Table 3 Correlation between APACHEⅡscore,APACHEⅢscore and H2O2,IL-6 level in EBC between the two groups at different time points after mechanical ventilation
3 討論
H2O2是炎性細胞激活O2時產(chǎn)生的代謝產(chǎn)物,其可以引起下呼吸道蛋白酶/抗蛋白酶、氧化/抗氧化失衡,導致小氣道和肺組織損傷[6-7],為機體氧化應激的重要標志物。IL-6是具有重要作用的多功能、多向性細胞因子[8],其可以參與多種疾病的發(fā)生發(fā)展過程、機體的炎性反應及免疫應答。國外文獻報道,ARDS患者EBC中H2O2水平明顯升高,其中以膿毒癥和嚴重腦損傷所致的ARDS患者最明顯[9]。近年研究還發(fā)現(xiàn),經(jīng)典的機械通氣策略(大潮氣量、小呼吸末正壓)可以導致EBC中IL-6水平升高[10]。因此,探討ARDS機械通氣患者EBC中H2O2和IL-6水平變化對監(jiān)測氣道炎癥、評估病情嚴重程度及協(xié)助判斷疾病預后具有重要的臨床意義。
本研究結果顯示,存活組患者機械通氣初期EBC中H2O2和IL-6水平升高,且其水平隨病情好轉開始降低,而死亡組患者隨病情惡化而繼續(xù)升高,估計與機械通氣患者感染重、氣道分泌物多、氣道炎性反應劇烈、肺部氧化應激加重而導致H2O2和IL-6生成超過過氧化酶清除能力有關。疾病進一步惡化后,患者EBC中H2O2和IL-6水平明顯升高,提示感染導致氧自由基生成增加,導致氧化-抗氧化失衡和氣道炎癥。機械通氣后1、3 d兩組患者EBC中H2O2和IL-6水平無差異,機械通氣后5、7 d死亡組患者EBC中H2O2和IL-6水平高于存活組,表明在機械通氣初期患者氧化應激和氣道炎癥程度較輕,因此該階段及時、有效地控制感染、糾正低氧血癥對患者取得良好預后具有重要意義;且ARDS機械通氣患者EBC中H2O2和IL-6水平能夠作為反映ARDS氣道炎性反應和肺部氧化損傷增強的早期較敏感指標,可協(xié)助判斷病情嚴重程度及預后。
本研究結果還顯示,存活組患者APACHEⅡ和APACHEⅢ評分隨機械通氣時間延長而開始降低,死亡組則相反,且死亡組患者機械通氣3、5、7 d APACHEⅡ和APACHEⅢ評分均高于存活組。相關性分析結果顯示,存活組患者機械通氣后不同時間點EBC中EBC中H2O2和IL-6水平與APACHEⅡ和APACHEⅢ評分間無直線相關關系,而死亡組患者機械通氣后5、7 d EBC中H2O2水平與APACHEⅡ和APACHEⅢ評分呈正相關,EBC中IL-6水平與APACHEⅡ和APACHEⅢ評分呈負相關。可見死亡組患者EBC中H2O2和IL-6水平的動態(tài)變化趨勢與APACHEⅡ和APACⅢ評分動態(tài)變化趨勢一致,H2O2和IL-6水平、APACHEⅡ和APACHEⅢ評分在死亡組均呈上升趨勢。因此,測定EBC中H2O2和IL-6水平還可用以輔助臨床、指導治療。
ARDS機械通氣患者EBC中H2O2和IL-6水平升高的具體機制尚不清楚,可能與下列因素有關:(1)由于存在缺氧及感染,氧自由基釋放增加,導致H2O2和IL-6水平隨之增加,活性氧通過氣道上皮細胞的IL-6釋放而參與局部免疫反應。而腫瘤壞死因子α (TNF-α)同樣可以引起IL-6 mRNA的表達增加[11]。感染及缺氧均可明顯增高患者交感神經(jīng)興奮性,引起血液中兒茶酚胺類物質(zhì)增加,進一步促進IL-6分泌。(2)在感染和缺氧的共同作用下,下呼吸道中性粒細胞及巨噬細胞數(shù)量明顯增多,而這些細胞可釋放較多H2O2。(3)不適當?shù)臋C械通氣引發(fā)或加重原有肺損傷,引起呼吸機相關性肺損傷(ventilation-associated lung injury,VALI)[10],此類變化促使肺內(nèi)炎性遞質(zhì)向血液內(nèi)轉移,可加重或引發(fā)全身炎癥反應綜合征,從而使EBC中H2O2和IL-6水平增加[12]。缺氧、感染和不適當?shù)臋C械通氣是引起EBC中H2O2和IL-6水平升高的主要原因,因此,抗氧化和抗感染治療及肺復張策略可以抑制ARDS機械通氣患者肺部氧化應激和炎性遞質(zhì)的產(chǎn)生。
綜上所述,ARDS機械通氣患者EBC中H2O2和IL-6水平均升高,且與病情嚴重程度相關,其可作為氣道炎性反應的監(jiān)測指標,結合APACHE評分可為評估患者預后提供參考。
[1]葉樹鳴,梁志欣,李影,等.189例急性呼吸窘迫綜合征患者的病死危險因素分層分析[J].國際呼吸雜志,2013,33(7): 533-536.
[2]易麗,席修明.小潮氣量通氣加肺復張法對急性呼吸窘迫綜合征療效的影響[J].中國危重病急救醫(yī)學,2005,8,17(8): 472-476.
[3]CarterSR,DavisCS,KovacsEJ.Exhaledbreathcondensate collection in the mechanically ventilated patient[J].Respir Med,2012,106(5):601-613.
[4]HorváthI,HuntJ,BarnesPJ.Exhaledbreathcondensate: methodological recommendations and unresolved questions[J]. European Respiratory Journal,2005,26(3):523-548.
[5]Ranieri VM,Rubenfeld GD,Thompson BT,et al.Acute respiratory distress syndrome:the berlin definition[J].JAMA,2012,307 (23):2526-2533.
[6]楊國輝,王廣發(fā).對機械通氣患者呼出氣冷凝液中過氧化氫的研究[J].中國危重病急救醫(yī)學,2008,20(6):324-326.
[7]楊國輝,王廣發(fā).慢性阻塞性肺疾病機械通氣患者呼出氣冷凝液中過氧化氫和白細胞介素-6的監(jiān)測及意義[J].中國危重病急救醫(yī)學,2010,22(8):455-458.
[8]Carradi M,Pignatti P,Manini P,et al.Comparison between exhaled and sputum oxidative stress biomarkers in chronic airway inflammation[J].Eur Respir J,2004,24(6):1011-1017.
[9]張文彬,陳建榮,蔡映云.急性肺損傷/急性呼吸窘迫綜合征患者呼出氣冷凝液檢測的研究進展[J].國際呼吸雜志,2009,29 (22):1365-1369.
[10]The Acute Respiratory Distress Syndrome Network.Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome[J].N Engl J Med,2000,342(18):1301-1308.
[11]Roca O,Gómez-Ollés S,Cruz MJ,et al.Effects of salbutamol on exhaledbreathcondensatebiomarkersinacutelunginjury: prospective analysis[J].Crit Care,2008,12(3):R72.
[12]Halbertsma FJ,Vaneker M,scheffer GJ,et al.Cytokines and biotrauma in ventilator-induced lung injury:a critical review of the literature[J].Neth J Med,2005,63(10):382-392.
Changes and Clinical Significances of Hydrogen Peroxide and Interleukin-6 Levels in Exhaled Breath Condensate of Patients with Acute Respiratory Distress Syndrome Treated with Mechanical Ventilation
NIU Yu-qian,YANG Guohui.
The Second People's Hospital of Guiyang,Guiyang 550081,China
ObjectiveTo investigate the changes and clinical significances of hydrogen peroxide(H2O2)and interleukin-6(IL-6)levels in exhaled breath condensate(EBC)of patients with acute respiratory distress syndrome (ARDS)treated with mechanical ventilation.MethodsFrom September 2012 to December 2013,a total of 42 patients with ARDS treated with mechanical ventilation were selected in MICU,the Second People's Hospital of Guiyang,and they were divided into survival group(n=22)and death group(n=20)according to 2-week prognosis after admission of MICU.APACHEⅡscore,APACHEⅢscore,H2O2and IL-6 levels in EBC were compared between the two groups after 1 day,3 days,5 days,7 days of mechanical ventilation,and their correlations were analyzed.ResultsH2O2and IL-6 levels in EBC after 3 days,5 days,7 days of mechanical ventilation of survival group were lower than those after 1 day of mechanical ventilation,respectively;while H2O2and IL-6 level in EBC after 7 days of mechanical ventilation of death group were higher than those after 1 day,3 days,5 days of mechanical ventilation,respectively(P<0.05).No statistically significant differences of APACHEⅡscore or APACHEⅢscore was found between the two groups after 1 day of mechanical ventilation(P>0.05);while APACHEⅡscore and APACHEⅢscore of death group were higher than those of survival group after 3 days,5 days,7 days of mechanical ventilation,respectively(P<0.05).No statistically significant differences of H2O2or IL-6 level in EBC was found between the two groups after 1 day,3 days of mechanical ventilation,respectively(P>0.05);while H2O2
Respiratory distress syndrome,adult;Respiration,artificial;Exhaled breath condensate;Hydrogen peroxide;Interleukin 6
R 563.8
A
10.3969/j.issn.1008-5971.2015.03.008
2014-12-08;
2015-03-08)
(本文編輯:謝武英)
550081貴州省貴陽市第二人民醫(yī)院呼吸內(nèi)科(牛毓茜);貴州省貴陽醫(yī)學院附屬醫(yī)院內(nèi)科ICU(楊國輝)
and IL-6 levels in EBC of death group were higher than those of survival group after 5 days,7 days of mechanical ventilation,respectively(P<0.05).In survival group,no linear correlation was found between H2O2or IL-6 level in EBC at each time point and APACHEⅡscore or APACHEⅢscore(P>0.05);in death group,H2O2in EBC after 5 days,7 days of mechanical ventilation was positively correlated with APACHEⅡscore and APACHEⅢscore,IL-6 level in EBC after 5 days,7 days of mechanical ventilation was negatively correlated with APACHEⅡscore and APACHEⅢscore(P<0.05).ConclusionH2O2and IL-6 levels in EBC of patients with ARDS treated with mechanical ventilation are higher and correlate with severity of illness,may be monitoring index of airway inflammatory reaction and provide evidences for predicting the prognosis by combining with APACHE score.
猜你喜歡
美與時代·美術學刊(2022年3期)2022-04-27 01:18:15
世界科學技術-中醫(yī)藥現(xiàn)代化(2020年2期)2020-07-25 02:05:56
當代工人(2020年8期)2020-05-25 09:07:38
人大建設(2019年12期)2019-05-21 02:55:32
小溪流(畫刊)(2017年12期)2018-01-10 16:07:29
科技知識動漫(2016年8期)2016-07-29 20:40:09
兒童故事畫報·發(fā)現(xiàn)號趣味百科(2015年12期)2016-01-25 00:41:49
西南軍醫(yī)(2016年6期)2016-01-23 02:21:19
西南軍醫(yī)(2015年2期)2015-01-22 09:09:37
食品科學(2013年15期)2013-03-11 18:25:48
