絕經前后尿酸與代謝綜合征的關聯分析
2015-06-01 12:30:16錢巧霞周敬茹丁月楊亞軍2金2王笑峰2王久存
復旦學報(醫學版) 2015年5期
錢巧霞周敬茹丁 月楊亞軍,2金 力,2王笑峰,2王久存,2△
(1復旦大學生命科學學院現代人類學教育部重點實驗室 上海 200438;2復旦大學泰州健康科學研究院 泰州 225300)
絕經前后尿酸與代謝綜合征的關聯分析
錢巧霞1周敬茹1丁 月1楊亞軍1,2金 力1,2王笑峰1,2王久存1,2△
(1復旦大學生命科學學院現代人類學教育部重點實驗室 上海 200438;2復旦大學泰州健康科學研究院 泰州 225300)
目的分析比較絕經前、后女性血清尿酸水平與代謝綜合征(metabolic syndrome,MS)的關系。方法采取多階段整群隨機抽樣的方法于2013年抽取江蘇省泰興市根思鄉、姚王鎮等12個自然村,調查40~65歲的女性3 187人,其中未絕經1 457人,已絕經者1 730人。分別分析未絕經組和絕經組尿酸水平與MS的關系。結果MS的總患病率為15.34%,絕經女性為18.68%,明顯高于未絕經女性(11.41%,P<0.001)。MS的患病率均隨尿酸水平的升高而升高(趨勢檢驗,P<0.001),同一尿酸水平時絕經女性的MS患病率高于未絕經女性。多因素Logistic回歸分析結果顯示無論是否絕經,尿酸均是MS的獨立危險因素,但同一尿酸水平時絕經女性患的MS患病風險高于未絕經女性。結論絕經對尿酸和MS的關系具有“修飾”作用,絕經后尿酸對MS的風險作用有所增加。
絕經; 代謝綜合征; 尿酸
尿酸是經腎臟排泄的嘌呤代謝產物。隨著生活水平提高和飲食結構改變,高嘌呤食物攝入不斷增多,體內尿酸水平也逐年增高[1]。研究表明,尿酸水平升高會增加代謝綜合征(metabolic syndrome,MS)的患病風險[2-3]。
女性絕經后失去雌激素的保護,體內尿酸水平將顯著升高。Wingrove等[4]發現,絕經后女性血清尿酸濃度比未絕經女性高10%;多因素校正后,該比例達到16%,且具有更顯著的統計學意義。此外,有研究發現絕經后MS的患病率也顯著增加。Eshtiaghi等[5]研究顯示,校正年齡因素后,絕經后MS的患病風險增加了2.85(1.31~6.20)倍。
然而,絕經是否會影響尿酸與MS之間的關系?目前僅有韓國的一個團隊對其進行了初步研究,發現絕經后尿酸對MS的風險有所增加[6]。由于不同種族間疾病的發生存在異質性,近年來中國人特別是女性群體,尿酸水平普遍升高且MS的患病率也存在增加趨勢[7-9],在中國人群中絕經是否會影響尿酸與MS之間的關系尚不清楚。本研究以3 187例40~65歲女性作為研究對象,通過比較絕經前、后女性血清尿酸水平與MS的關系,來探究絕經對于尿酸和MS之間關系的影響,為女性MS的防控提供新思路。
資料和方法
研究對象采取多階段整群隨機抽樣的方法于2013年抽取江蘇省泰興市根思鄉、姚王鎮等12個自然村。以具有當地戶籍或在當地居住≥5年的40 ~65歲的女性為研究對象,排除有嚴重認知障礙等不能完成和不配合受訪者。現場共調查3 456人,其中259人因非自然絕經,7人因檢查指標不全而被剔除,最終共納入3 187人進入分析。
問卷調查受訪者清晨在村衛生室集合,由經過專業培訓并考察合格的調查員對其進行一對一面對面調查。內容包括:一般人口學特征、疾病史、藥物治療史、是否絕經、絕經方式等。
生化檢查調查對象血液標本的采集在清晨統一進行,抽取調查對象禁食10 h以上的空腹靜脈血5 m L,分離血清并在5 h內應用東芝40 FR全自動生化分析儀進行尿酸、空腹血糖(fasting plasma glucose,FPG)、高密度脂蛋白膽固醇(high density lipoprotein-cholesterol,HDL-C)、低密度脂蛋白膽固醇(low density lipoprotein-cholesterol,LDL-C)、三酰甘油(triglyceride,TG)、總膽固醇(total cholesterol,TC)等生化指標的檢測。
人體體質指標及測量方法調查對象脫去鞋、帽、外衣,身高、體重的測量通過已校準的自動測量儀(KIKER PIUS GL-310)來完成;腰圍為平靜呼吸狀態下臍上1 cm水平的周長,臀圍為臀部的最大周長,身高和腰臀圍均精確到0.1 cm,體重精確到0.1 kg。采用進口全自動血壓計(EASY-X-900)對右側肱動脈血壓進行測量,測量前30 min內禁止吸煙、飲茶、取坐位休息15 min,連續測量2次,間隔1~2 min,血壓取平均值。體質指數(BMI)=體重(kg)/身高2(m2),腰臀比(WHR)=腰圍(cm)/臀圍(cm)。
診斷標準MS診斷標準采用中華醫學會糖尿病分會MS的診斷標準(CDS2004)[10],需符合以下5項標準中的3項及以上:(1)超重或肥胖,BMI≥25.0 kg/m2;(2)高血糖,FPG≥6.1 mmol/L和(或)已確診為糖尿病并治療者;(3)高血壓,收縮壓≥140 mm Hg(1 mm Hg=0.133 k Pa,下同)和(或)舒張壓≥90 mm Hg和(或)已確診高血壓并治療者;(4)高血脂,空腹血TG≥1.7 mmol/L;(5)空腹血HDL-C<0.9 mmol/L(男),<1.0 mmol/L(女)。停經≥12個月定義為絕經[11]。
統計學方法將調查對象分為未絕經女性和絕經女性進行統計分析。服從正態分布的連續型資料用±s表示,兩組間的均數比較采用獨立樣本的t檢驗,率的比較用χ2檢驗。趨勢檢驗采用χ2趨勢檢驗。尿酸水平與MS關聯因素相關性分析采用Pearson's相關分析。根據尿酸水平四分位進行劃分,4個組別以Q1~Q4表示,以Q1為參照,利用Logistics回歸分析比較女性絕經前后血清尿酸水平與MS的關系。檢驗水準為α=0.05,采用SPSS 18.0進行統計分析。
結 果
人口學特征本研究共納入3 187人,平均年齡(52.28±7.28)歲,未絕經女性1 457人,占45.72%,絕經女性1 730人,占54.28%。絕經者的年齡、腰臀比、收縮壓、舒張壓、HDL-C、LDL-C、FPG、尿酸、TG、TC、MS患病率均高于未絕經者,差異有統計學意義(P<0.01);兩者BMI差異無統計學意義(P>0.05,表1)。
表1 研究對象的一般人口學特征Tab 1 Demographic data of the population based on menopausal status(±s)
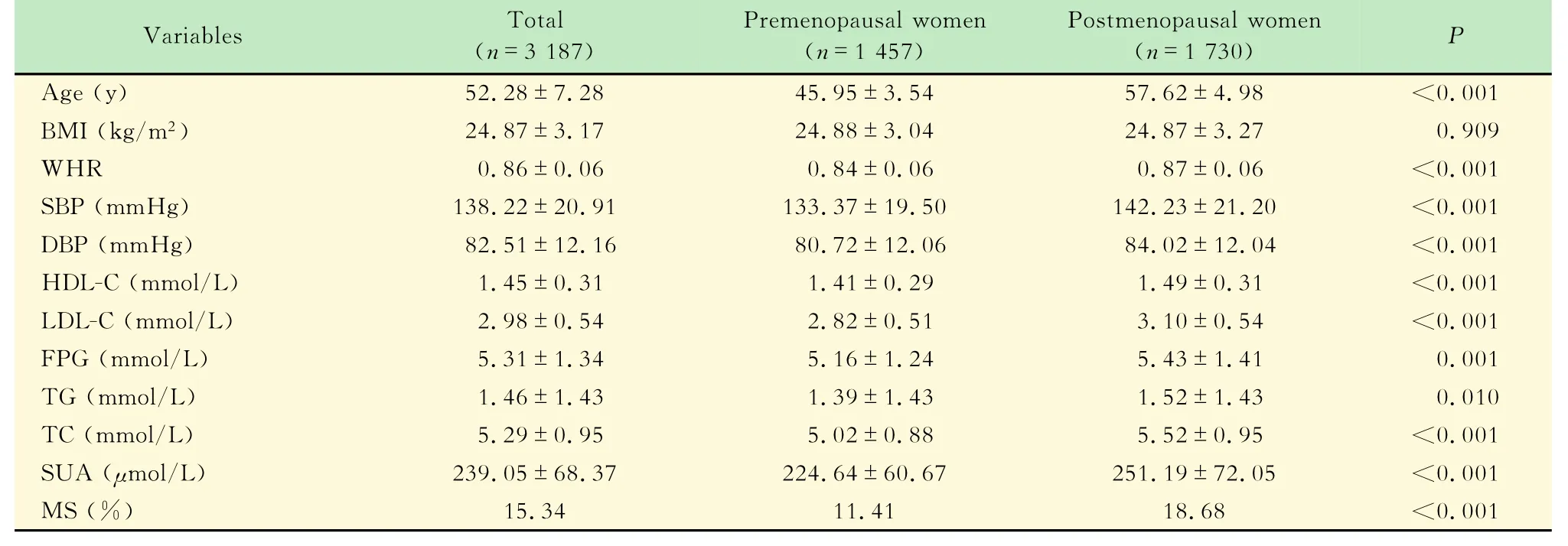
表1 研究對象的一般人口學特征Tab 1 Demographic data of the population based on menopausal status(±s)
BMI:Body mass index;WHR:Waist-to-hip ratio;SBP:Systolic blood pressure;DBP:Diastolic blood pressure;HDL-C:High density lipoprotein-cholesterol;LDL:Low density lipoprotein-cholesterol;FPG:Fasting plasma glucose;TG:Triglycerides;TC:Total cholesterol;SUA:Serum uric acid;MS:Metabolic syndrome.The difference between premenopausal women and postmenopausal women was analyzed by t-test.
MS患病率與尿酸水平正相關無論是未絕經女性還是絕經女性MS的患病率均隨著尿酸水平的升高而升高(趨勢檢驗,P<0.001);同一尿酸水平絕經女性MS的患病率高于未絕經女性(圖1)。

圖1 不同尿酸水平下MS的患病率Fig 1 Prevalence of MS according to serum uric acid level
尿酸水平與MS相關因素顯著相關BMI、收縮壓、舒張壓、HDL-C、FPG、TG都是MS的重要組分,而年齡、腰臀比、LDL-C、TC均與MS有密切關聯。女性尿酸水平與MS諸多相關因素是否相關,(表2),總體上,尿酸水平除與FPG無關(P>0.05)外,與其余因素均相關(P<0.001),相關系數最高的前5位因素依次為腰圍(r=0.257)、TG(r= 0.243)、BMI(r=0.240)、LDL-C(r=0.187)、年齡(r=0.186),尿酸與HDL-C呈負相關,相關系數為r=-0.147;進一步分析顯示,未絕經女性尿酸水平與年齡和空腹血糖無關聯,與其余因素均相關,(P <0.001)。相關系數最高的前5位因素依次為TG、BMI、腰臀比、LDL-C、收縮壓,尿酸與HDL-C呈負相關,相關系數為r=-0.126;絕經女性尿酸水平與FPG無關聯,與其余因素均相關(P<0.01),相關系數最高的前5位因素依次為BMI、TG、HDL-C(r=-0.216)、腰臀比、收縮壓。
尿酸是MS的獨立危險因素根據尿酸水平進行四分位劃分,4個組別以Q1~Q4表示。以Q1為參照,利用兩個模型進行多因素Logistic回歸分析后顯示,在總人群、未絕經女性、絕經女性,尿酸都是MS的獨立危險因素。同一個尿酸水平絕經女性患MS的風險高于未絕經女性,如校正年齡、BMI、收縮壓、舒張壓、HDL-C、FPG、TG、腰臀比、LDL-C、TC后(Model 2),當尿酸水平Q1為199~240 μmol/L時,絕經女性MS的患病風險為2.03(1.05 ~3.93),高于未絕經女性1.27(0.62~2.60)。當尿酸水平Q2為241~280μmol/L時,絕經女性MS的患病風險為2.25(1.19~4.28),高于未絕經女性的1.23(0.60~2.51)。當尿酸水平Q3>280μmol/L時,絕經女性MS的患病風險為2.31(1.26~4.24),高于未絕經女性的1.79(0.89~3.59)(表3)。

表2 尿酸水平與MS相關因素Pearson相關性分析Tab 2 Pearson bivariate correlation between serum uric acid and MS related variables
討 論
MS是個體多種代謝異常情況的集聚狀態,發病以胰島素抵抗或肥胖為核心,是心血管疾病、Ⅱ型糖尿病的重要危險因素。我國MS的患病率正在逐年增長,盧偉等[12]在上海人群的調查中發現,女性45歲以后MS的患病率有明顯上升趨勢,且患病率超過男性。本研究MS的總體患病率為15.34%,絕經女性MS的患病率高達18.68%,是未絕經女性(11.41%)的1.64倍。

表3 不同尿酸水平發生MS風險的多因素Logistic回歸分析Tab 3 Adjusted odds ratio(95%confidence interval)for risk of MS according to uric acid concentration derived from multivariate Logistic regression analysis
本研究證實尿酸是MS的獨立危險因素,并且尿酸與MS諸多相關因素關聯,與文獻一致[12-15]。一項對2 222名山東人(>25歲)隨訪6年的研究結果顯示,校正TC、LDL-C后,尿酸是MS發病的獨立危險因素(OR=1.69,P<0.001)[15]。目前有學者建議把尿酸用于預測女性MS,且已有研究報道利用尿酸值診斷女性MS的曲線下面積可達0.82[16-17]。
之前的研究多側重于尿酸與MS的關系,而很少關注絕經這一因素對尿酸與MS關系的影響。本研究多因素Logistic回歸分析結果發現中國人群中無論是否絕經,尿酸水平的升高都會獨立增加MS患病風險。但是,絕經后尿酸對MS的作用風險更大。Lee等[6]在韓國的研究(1 018名未絕經女性和626名已絕經女性)結果顯示,校正了年齡和BMI后,未絕經女性第四分位尿酸水平MS患病風險是第一分位尿酸水平的2.08 (1.21~3.97)倍,而絕經女性第四分位尿酸水平MS患病風險是第一分位尿酸水平的2.38(1.33~4.03)倍。這說明絕經對尿酸和MS的關系具有“修飾”作用,絕經后尿酸對MS的風險作用有所增加。
絕經如何影響尿酸與MS關系的作用機制尚不清楚。一方面,已有研究證實尿酸是MS的危險因素會增加胰島素抵抗的風險。隨訪研究發現,基線為高尿酸血癥的患者15年后發展成胰島素抵抗的風險是正常人的1.36倍[18]。高尿酸患者進行降低血尿酸治療后,患者的胰島素抵抗及胰島β細胞功能都有所改善[19]。另一方面,絕經后體內最大的變化是卵巢功能逐漸衰退和雌激素水平逐漸下降,這會導致血清尿酸水平升高,胰島素敏感性降低,炎性因子水平升高。雌激素對尿酸水平的調節具有重要作用,研究發現使用雌激素替代治療的絕經后女性的尿酸水平及高尿酸患病率明顯下降[20-21]。Nicholls等[22]發現,雌激素水平越高,腎臟對尿酸的清除能力越高,尿酸再吸收能力越低。大量研究表明絕經是胰島素抵抗的危險因素。絕經后雌激素水平下降,而雌激素可以增強胰島素的信號轉導,增強糖脂代謝關鍵酶的活性,促進葡萄糖轉運體的表達和轉位,增強胰島素的敏感性[23-24]。絕經后一些細胞因子(如IL-6、TNF-a、瘦素、脂聯素等)水平升高,增加了胰島素抵抗的風險[25-26]。如IL-6作為一種前炎性因子能下調胰島素受體底物和葡萄糖轉運蛋白,阻礙葡萄糖的轉運[26],從而直接使得胰島素抵抗風險增加。絕經后,腎尿酸清除能力下降導致血清尿酸水平升高,同時胰島素敏感性降低,增加了尿酸與MS的風險關系。絕經、尿酸、MS三者之間可能存在更為復雜的關系,有待更多的研究去探索。
本研究為橫斷面研究,樣本量有限,因果論證的強度較為局限,絕經對尿酸與MS的關系的影響尚需擴大樣本量或者通過前瞻性研究進一步論證。在MS的防控工作中,絕經女性應成為重點人群,加強尿酸水平的監測,倡導健康飲食和健康的生活方式。
[1]Liu B,Wang T,Zhao HN,et al.The prevalence of hyperuricemia in China:a meta-analysis[J].BMC Public Health,2011,11:832.
[2]Tae WY,Ki CS,Hun SS,et al.Relationship between serum uric acid concentration and insulin resistance and metabolic syndrome [J].Circ J,2005,69(8):928-933.
[3]劉佩文,陳璐璐,孫暉,等.武漢地區人群高尿酸血癥與代謝綜合征的相關性[J].中國糖尿病雜志,2007(12):727-728.
[4]Wingrove CS,Walton C,Stevenson J.The effect of menopause on serum uric acid levels in non-obese healthy women[J]. Metabolism,1998,47(4):435-438.
[5]Eshtiaghi R,Esteghamati A,Nakhjavani M.Menopause is an independent predictor of metabolic syndrome in Iranian women [J].Maturitas,2010,65(3):262-266.
[6]Lee HJ,Park HT,Cho GJ,et al.Relationship between uric acid and metabolic syndrome according to menopausal status[J]. Gynecol Endocrinol,2011,27(6):406-411.
[7]Nan H,Qiao Q,Dong Y,et al.The prevalence of hyperuricemia in a population of the coastal city of Qingdao,China[J].J Rheumatol,2006,33(7):1346-1350.
[8]余俊文,楊同廣,刁偉霞,等.廣東省佛山市居民高尿酸血癥及痛風的流行病學調查[J].中華流行病雜志,2010,31(8):860-862.
[9]Yu S,Guo X,Yang H,et al.An update on the prevalence of metabolic syndrome and its associated factors in rural northeast China[J].BMC Public Health,2014,14:877.
[10]中華醫學會糖尿病學分會代謝綜合征研究協作組.中華醫學會糖尿病學分會關于代謝綜合征的建議[J].中華糖尿病雜志,2004,12(3):5-10.
[11]Nash D,Magder LS,Sherwinet R,et al.Bone density-related predictors of blood lead level among peri-and postmenopausal women in the United States:The Third National Health and Nutrition Examination Survey,1988-1994[J].Am J Epidemiol,2004,160(9):901-911.
[12]盧偉,劉美霞,李銳,等.上海15~74歲居民代謝綜合征的流行特征[J].中華預防醫學雜志,2006,40(4):262-268.
[13]梁凱,曲勇,鄧楠,等.無癥狀性高尿酸血癥與代謝綜合征及其組分相關性的研究[J].中國糖尿病雜志,2013,21(5):388 -391.
[14]Zhang Q,Zhang C,Song X,et al.A longitudinal cohort based association study between uric acid level and metabolic syndrome in Chinese Han urban male population[J].BMC Public Health,2012,12:419.
[15]Wang JY,Chen YL,Hsu CH,et al.Predictive value of serum uric acid levels for the diagnosis of metabolic syndrome in adolescents[J].J Pediatr,2012,161(4):753-756.
[16]Lee MS,Lin SC,Chang HY,et al.High prevalence of hyperuricemia in elderly Taiwanese[J].Asia Pac J Clin Nutr,2005,14(3):285-292.
[17]胡健偉,馮艷,蔡曉琴,等.不同性別居民尿酸水平與代謝綜合征相關性[J].中國公共衛生,2013,29(4):562-565.
[18]Eswar K,Pandya BJ,Chung L,et al.Hyperuricemia in young adults and risk of insulin resistance,prediabetes,and diabetes:a 15-year follow-up study[J].Am J Epidemiol.2012,176(2):108-116.
[19]丁立新,賀娓利,吉漩.降低血尿酸治療對高尿酸血癥患者胰島素抵抗及胰島β細胞功能的影響[J].中國糖尿病雜志,2012,20(7):496-498.
[20]Sumino H,Ichikawa S,Kanda T,et al.Reduction of serum uric acid by hormone replacement therapy in postmenopausal women with hyperuricaemia[J].Lancet,1999,354(9179):650.
[21]Hak AE,Choi HK.Menopause,postmenopausal hormone use and serum uric acid levels in US women--the Third National Health and Nutrition Examination Survey[J].Arthritis Res Ther,2008,10(5):116.
[22]Nicholls A,Snaith ML,Scott JT.Effect of oestrogen therapy on plasma and urinary levels of uric acid[J].Br Med J,1973,1 (5851):449-451.
[23]Pratchayasakul W,Chattipakorn N,Chattipakorn SC.Estrogen restores brain insulin sensitivity in ovariectomized non-obese rats,but not in ovariectomized obese rats[J].Metabolism,2014,63(6):851-859.
[24]Rasgon NL,Kenna HA,Wroolie TE,et al.Insulin resistance and medial prefrontal gyrus metabolism in women receiving hormone therapy[J].Psychiatry Res,2014,223(1):28-36.
[25]Kim OY,Chae JS,Paik JK,et al.Effects of aging and menopause on serum interleukin-6 levels and peripheral blood mononuclear cell cytokine production in healthy nonobese women[J].Age(Dordr),2012,34(2):415-425.
[26]Lagathu C,Bastard JP,Auclair M,et al.Chronic interleukin-6 (IL-6)treatment increased IL-6 secretion and inducedinsulin resistance in adipocyte:prevention by rosiglitazone[J].Biochem Biophys Res Commun,2003,311(2):372-379.
The relationship between serum uric acid concentration and metabolic syndrome according to different menopausal status
QIAN Qiao-xia1,ZHOU Jing-ru1,DING Yue1,YANG Ya-jun1,2,JIN Li1,2,WANG Xiao-feng1,2,WANG Jiu-cun1,2△
(1Ministry of Education Key Laboratory of Contemporary Anthropology,School of Life Sciences,Fudan University,Shanghai 200433,China;2The Taizhou Health Research Insitute,Fudan University,Taizhou 225300,Jiangsu Province,China)
ObjectiveTo compare the relationship between uric acid and the metabolic syndrome (MS)according to different menopausal status.MethodsIn 2013,3 187 women age ranged from 40 to 65 and including 1 457 premenopausal women and 1 730 postmenopausal women were enrolled from 12 villages of Gensi township and Yaowang township of Taixing city though three-stage stratified sampling method.The study subjects were divided into premenopausal women group and postmenopausal women group for the analysis on the relationship between serum uric acid concentration and metabolic syndrome.ResultsThe overall prevalence of MS was 15.34%,while in the premenopausal women it was 18.68%,which was significantly higher than premenopausal women (11.41%,P<0.001).The prevalence of MS was increasing as the level of serum uric acid(P<0.001,trend test),however the prevalence was higher among postmenopausal women.Logistic regression analysis showed that Uric acid was an independent factor for MSin neither postmenopausal women nor premenopausal women.However,postmenopausal women had greater risk of MS than the premenopausal women with the same uric acid level.ConclusionsMenopause has a“modified”effect on the relationship between uric acid level and MS,and menopause would increase the risk effect of uric acid to MS.
menopause; metabolic syndrome; uric acid
E-mail:xiaofenggautomatic@gmail.com
R589
A
10.3969/j.issn.1672-8467.2015.05.003
2014-12-01;編輯:段佳)
上海市科委基礎研究重大項目(11DJ1400102),國家科技支撐重點項目(2011BAI09B00)△
*This work was supported by the Major Fundamental Research of Shanghai Science and Technology Committee(11DJ1400102)and the National Key Technology Suppor program(2011BAI09B00).
猜你喜歡
美與時代·美術學刊(2022年3期)2022-04-27 01:18:15
健康體檢與管理(2022年2期)2022-04-15 22:33:17
昆明醫科大學學報(2021年1期)2021-02-07 01:06:44
中國生殖健康(2019年2期)2019-08-23 08:12:10
人大建設(2019年12期)2019-05-21 02:55:32
中國男科學雜志(2016年9期)2016-03-20 15:00:09
中國衛生標準管理(2015年1期)2016-01-14 03:41:27
中國健康心理學雜志(2015年5期)2015-09-05 09:55:52
藥學與臨床研究(2015年4期)2015-06-05 11:35:51
中國全科醫學(2013年36期)2013-01-25 06:20:58