甲狀腺微小乳頭狀癌頸淋巴結(jié)轉(zhuǎn)移的危險(xiǎn)因素分析
2015-12-20 08:26:13卞雪艷孫姍姍郭文宇趙明慧孔令平張侖
中國(guó)腫瘤臨床 2015年13期
關(guān)鍵詞:分析
卞雪艷 孫姍姍 郭文宇 趙明慧 孔令平 張侖
·臨床研究與應(yīng)用·
甲狀腺微小乳頭狀癌頸淋巴結(jié)轉(zhuǎn)移的危險(xiǎn)因素分析
卞雪艷 孫姍姍 郭文宇 趙明慧 孔令平 張侖
目的:探討甲狀腺微小乳頭狀癌頸淋巴結(jié)轉(zhuǎn)移的危險(xiǎn)因素,分析高分辨率B超對(duì)側(cè)頸淋巴結(jié)轉(zhuǎn)移的診斷意義。方法:回顧性分析2013年1月至2013年11月天津醫(yī)科大學(xué)腫瘤醫(yī)院共1 037例甲狀腺微小乳頭狀癌患者的臨床病理資料。結(jié)果:1 037例患者中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移率為32.02%(332例),側(cè)頸淋巴結(jié)轉(zhuǎn)移率為6.85%(71例)。男性、年齡≤45歲、腫瘤直徑>5 mm、多灶性、雙發(fā)性、侵犯包膜和甲狀腺外局部侵犯者中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移率較高(P<0.05)。男性、中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移、B超診斷陽(yáng)性者側(cè)頸淋巴結(jié)轉(zhuǎn)移率較高,并且隨著中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移數(shù)目的增多,側(cè)頸轉(zhuǎn)移率也隨之增高(P<0.05)。高分辨率B超對(duì)側(cè)頸淋巴結(jié)轉(zhuǎn)移的靈敏度、特異度分別為92.96%、81.48%。結(jié)論:對(duì)中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移高危因素的人群應(yīng)行預(yù)防性中央?yún)^(qū)淋巴結(jié)清掃術(shù),高分辨率B超對(duì)預(yù)測(cè)甲狀腺微小乳頭狀癌患者頸淋巴結(jié)轉(zhuǎn)移具有重要的診斷意義,對(duì)側(cè)頸淋巴結(jié)轉(zhuǎn)移高危因素的人群應(yīng)行患側(cè)側(cè)頸淋巴結(jié)清掃術(shù)。
甲狀腺微小乳頭狀癌 頸淋巴結(jié)清掃術(shù) B超 診斷
近幾十年甲狀腺乳頭狀癌的發(fā)病率逐年增高,占所有新發(fā)甲狀腺惡性腫瘤90%以上[1]。其可能原因是隨著影像學(xué)技術(shù)如B超、CT、MRI及細(xì)針穿刺學(xué)的發(fā)展,甲狀腺乳頭狀癌的檢出率遞增。甲狀腺微小乳頭狀癌(papillary thyroid microcarcinoma,PTMC)是指腫瘤直徑≤1 cm的甲狀腺乳頭狀癌[2]。據(jù)報(bào)道,甲狀腺微小乳頭狀癌的中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移率可達(dá)24%~64%[3-4]。目前對(duì)于cN0的PMTC患者是否需行中央?yún)^(qū)淋巴結(jié)清掃術(shù)觀點(diǎn)不一,有研究認(rèn)為預(yù)防性清掃中央?yún)^(qū)淋巴結(jié)增加了喉返神經(jīng)損傷及甲狀旁腺功能低下的危險(xiǎn)[5],但另有研究認(rèn)為預(yù)防性中央?yún)^(qū)淋巴結(jié)清掃可降低PMTC患者復(fù)發(fā)率并提高生存率[6-7]。本研究擬分析甲狀腺微小乳頭狀癌淋巴結(jié)轉(zhuǎn)移的相關(guān)危險(xiǎn)因素,篩選淋巴結(jié)轉(zhuǎn)移高危險(xiǎn)因素患者,從而為手術(shù)方式的選擇提供參考價(jià)值并探討高分辨率B超對(duì)診斷側(cè)頸淋巴結(jié)轉(zhuǎn)移的意義。
1 材料與方法
1.1 臨床資料
天津醫(yī)科大學(xué)腫瘤醫(yī)院2013年1月至2013年11月PMTC患者共1 221例,其中新發(fā)病例1 120例(91.73%)。單純行患側(cè)腺葉切除83例,行中央?yún)^(qū)淋巴結(jié)清掃術(shù)或甲狀腺癌聯(lián)合根治術(shù)1 037例。納入標(biāo)準(zhǔn):初治,經(jīng)術(shù)后病理確診為PMTC,手術(shù)方式為腺葉+中央?yún)^(qū)淋巴結(jié)清掃術(shù)或側(cè)頸淋巴結(jié)清掃術(shù)。中央?yún)^(qū)淋巴結(jié)清掃術(shù)的范圍上界至甲狀軟骨,下界達(dá)胸腺,外側(cè)界為頸動(dòng)脈鞘內(nèi)側(cè)緣,包括氣管前、氣管旁、喉前淋巴結(jié)等。側(cè)頸淋巴結(jié)清掃范圍根據(jù)1991年美國(guó)耳鼻喉頭頸外科基金會(huì)標(biāo)準(zhǔn)分為Ⅱ、Ⅲ、Ⅳ、Ⅴ區(qū)。術(shù)中在有效保留甲狀旁腺及喉返神經(jīng)功能的情況下行病灶同側(cè)中央?yún)^(qū)淋巴結(jié)清掃術(shù)。若術(shù)前B超或術(shù)中探查發(fā)現(xiàn)有側(cè)頸淋巴結(jié)轉(zhuǎn)移,則術(shù)中清除病灶側(cè)頸淋巴結(jié)。
1.2 統(tǒng)計(jì)學(xué)分析
實(shí)驗(yàn)數(shù)據(jù)分析采用SPSS 20.0統(tǒng)計(jì)軟件,結(jié)果采用χ2檢驗(yàn),多因素分析采用非條件Logistic回歸模型分析。P<0.05為差異有統(tǒng)計(jì)學(xué)意義。
2 結(jié)果
2.1 患者特點(diǎn)
1037例行中央?yún)^(qū)淋巴結(jié)清掃或側(cè)頸淋巴結(jié)清掃術(shù)的甲狀腺微小乳頭狀癌患者中,男性208例(20.1%)、女性829例(79.9%),男女比例1∶3.99;年齡12~76歲,平均年齡(45.67±0.99)歲,其中年齡≤45歲505例(48.7%),>45歲532例(51.3%)。腫瘤直徑≤5mm 499例(48.1%),>5 mm 538例(51.9%)。1 037例患者中,多灶性、雙發(fā)性、包膜侵犯、局部侵犯、伴發(fā)橋本甲狀腺炎患者所占比例分別為32.5%(337例)、34.5%(358例)、68.9%(715例)、2.6%(27例)、6.3%(65例)。所有病例中,中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移率為32.02%(332例),側(cè)頸淋巴結(jié)轉(zhuǎn)移率為6.85%(71例),同時(shí)發(fā)生中央?yún)^(qū)和側(cè)頸淋巴結(jié)轉(zhuǎn)移率為6.65%(69例)。其中經(jīng)術(shù)前B超診斷或術(shù)中探查有側(cè)頸區(qū)淋巴結(jié)轉(zhuǎn)移者98例,均行患側(cè)甲狀腺癌聯(lián)合根治術(shù)。
2.2 中央?yún)^(qū)轉(zhuǎn)移危險(xiǎn)因素
如表1所示,男性患者的中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移率高于女性患者(P<0.05)。年齡≤45歲患者中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移率為35.05%,年齡>45歲患者其中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移率為29.16%(P=0.041),說(shuō)明年齡與中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移有相關(guān)性,且年齡≤45歲患病是其危險(xiǎn)因素。腫瘤直徑是否影響中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移(central lymph node metastasis,CLNM)一直存在爭(zhēng)議,本研究1 037例患者中,腫瘤直徑≤5 mm 126例(25.25%),>5 mm 206例(48.33%),說(shuō)明病灶大小是CLNM的影響因素(P<0.05)。同樣,腫瘤侵犯包膜、侵犯局部組織、多灶性及雙發(fā)性均為CLNM的危險(xiǎn)因素(P<0.05),而伴發(fā)橋本甲狀腺炎對(duì)CLNM無(wú)影響(P=0.824)。多因素分析表明,年齡、性別、腫瘤大小、侵犯包膜是甲狀腺微小乳頭狀癌的獨(dú)立危險(xiǎn)因素(表2)。

表1 中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移情況與臨床資料相關(guān)性分析Table 1 Correlation analysis of cervical lymph node metastases with clin?ical data of papillary thyroid microcarcinoma patients
2.3 側(cè)頸淋巴結(jié)轉(zhuǎn)移的危險(xiǎn)因素
本研究分析98例行甲狀腺癌聯(lián)合根治術(shù)的PMTC患者,其中經(jīng)術(shù)后病理確診的側(cè)頸淋巴結(jié)轉(zhuǎn)移患者71例,轉(zhuǎn)移率72.45%。單因素分析提示(表3),男性、中央?yún)^(qū)轉(zhuǎn)移、術(shù)前B超診斷陽(yáng)性、中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移數(shù)目為側(cè)頸轉(zhuǎn)移的危險(xiǎn)因素,且隨著中央?yún)^(qū)轉(zhuǎn)移淋巴結(jié)數(shù)目增多,側(cè)頸轉(zhuǎn)移的概率亦增加(P<0.05)。多因素分析表明,B超診斷是側(cè)頸轉(zhuǎn)移的獨(dú)立預(yù)測(cè)因素(P=0.003),OR值為0.227,95%CI為15.358~219.644。
2.4 B超對(duì)側(cè)頸淋巴結(jié)轉(zhuǎn)移診斷的意義
98例行側(cè)頸淋巴結(jié)清掃術(shù)的患者中經(jīng)B超診斷有側(cè)頸淋巴結(jié)轉(zhuǎn)移為86例,病理確診為71例。B超診斷有側(cè)頸淋巴結(jié)轉(zhuǎn)移而病理診斷陰性5例,而病理診斷陽(yáng)性B超診斷陰性5例。高分辨率B超對(duì)側(cè)頸淋巴結(jié)轉(zhuǎn)移的靈敏度、特異度、假陰性率和假陽(yáng)性率分別為92.96%、81.48%、7.04%、18.52%。

表2 中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移的多因素Logistic回歸分析Table 2 Multivariate logistic regression analysis for central lymph node metastasis
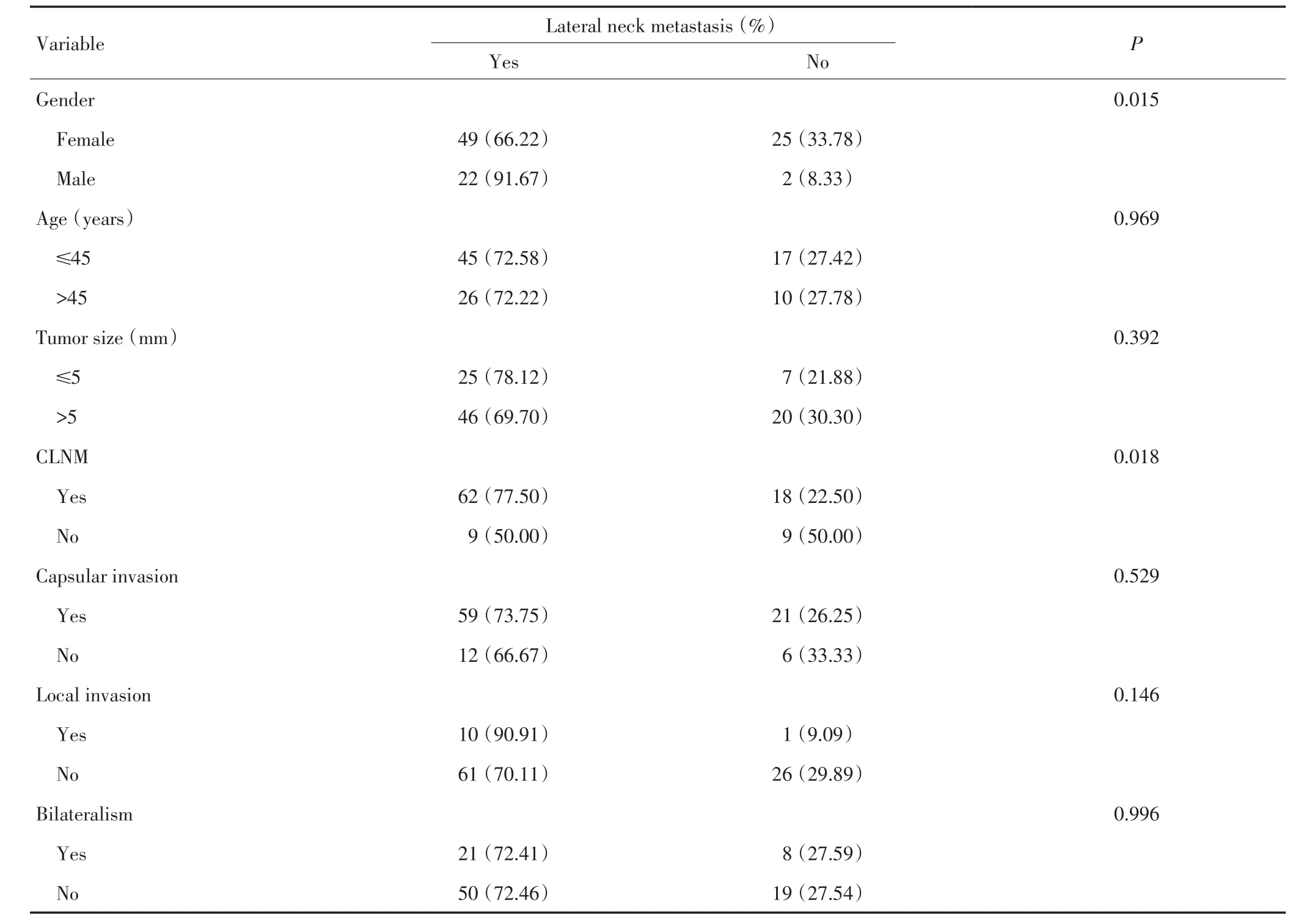
表3 側(cè)頸淋巴結(jié)轉(zhuǎn)移情況與臨床資料相關(guān)性分析Table 3 Correlation analysis of lateral neck metastases with clinical data of papillary thyroid microcarcinoma patients
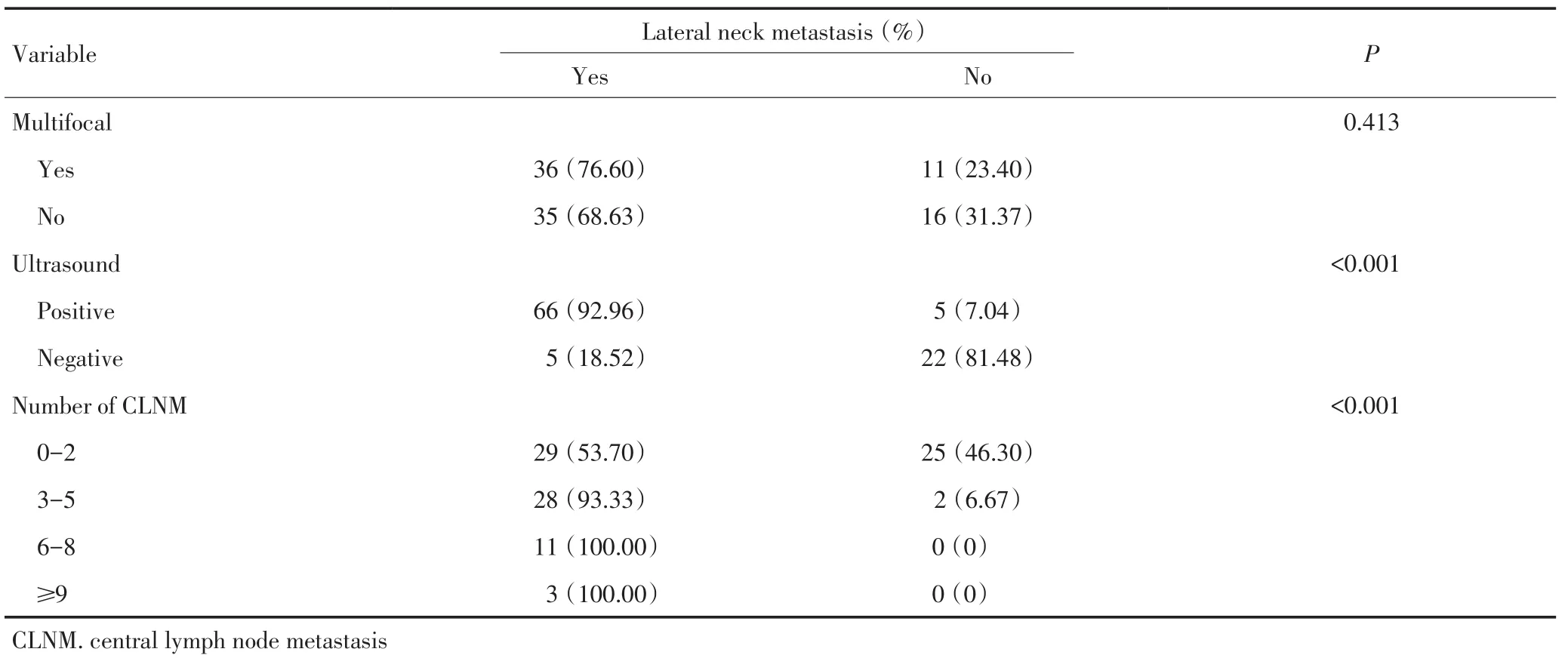
表3 側(cè)頸淋巴結(jié)轉(zhuǎn)移情況與臨床資料相關(guān)性分析(續(xù)表3)Table 3 Correlation analysis of lateral neck metastases with clinical data of papillary thyroid microcarcinoma patients
3 討論
淋巴結(jié)轉(zhuǎn)移是分化型甲狀腺癌最主要的轉(zhuǎn)移途徑,轉(zhuǎn)移方式主要是由中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移至側(cè)頸區(qū)淋巴結(jié)。有研究提示PMTC頸部淋巴結(jié)轉(zhuǎn)移率為24%~64%[3-4],而本研究中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移率為32.02%,與文獻(xiàn)報(bào)道一致。盡管甲狀腺微小乳頭狀癌的頸部淋巴結(jié)轉(zhuǎn)移率較高,但有報(bào)道提示頸部淋巴結(jié)轉(zhuǎn)移對(duì)分化型甲狀腺癌患者的死亡率無(wú)影響[8]。因此對(duì)臨床上淋巴結(jié)陰性的PMTC患者是否需要預(yù)防性清掃中央?yún)^(qū)淋巴結(jié)至今仍有爭(zhēng)議[9]。
Mao等[1]對(duì)332例甲狀腺微小癌患者進(jìn)行分析,認(rèn)為年齡(≤45歲)、男性是甲狀腺微小乳頭狀癌中央?yún)^(qū)轉(zhuǎn)移的獨(dú)立危險(xiǎn)因素。本研究對(duì)1 037例甲狀腺微小乳頭狀癌進(jìn)行回顧性分析發(fā)現(xiàn),年齡≤45歲、男性、腫瘤直徑>5 mm、侵犯包膜是PMTC患者中央?yún)^(qū)轉(zhuǎn)移的獨(dú)立危險(xiǎn)因素。Liu等[10]一項(xiàng)Meta分析統(tǒng)計(jì)1 928例行預(yù)防性中央?yún)^(qū)淋巴結(jié)清掃的PMTC患者,認(rèn)為對(duì)于腫瘤直徑>5 mm、多灶性或侵犯包膜的PMTC患者應(yīng)行預(yù)防性中央?yún)^(qū)淋巴結(jié)清掃術(shù)。Popa?dich等[11]認(rèn)為,中央?yún)^(qū)淋巴結(jié)清掃可造成暫時(shí)性的低鈣及聲帶麻痹,但對(duì)于遠(yuǎn)期低鈣癥狀及聲帶麻痹兩組間比較則無(wú)統(tǒng)計(jì)學(xué)意義。國(guó)內(nèi)有報(bào)道稱二次手術(shù)喉返神經(jīng)損傷率高達(dá)17%[12]。吳延升等[13]對(duì)cN0期患者行預(yù)防性淋巴結(jié)清掃術(shù)后復(fù)發(fā)率明顯低于單純腫物切除和局部廣切者。因此本研究認(rèn)為對(duì)于中央?yún)^(qū)轉(zhuǎn)移高危因素的人群(年齡≤45歲、男性、腫瘤直徑>5 mm、侵犯包膜)應(yīng)預(yù)防性行患側(cè)中央?yún)^(qū)淋巴結(jié)清掃,可以避免復(fù)發(fā)再手術(shù)時(shí)因氣管食管溝瘢痕粘連或組織解剖不清造成甲狀旁腺和喉返神經(jīng)的損傷。
目前關(guān)于Ⅵ區(qū)淋巴結(jié)轉(zhuǎn)移能否作為預(yù)測(cè)側(cè)頸淋巴結(jié)轉(zhuǎn)移的指標(biāo)眾說(shuō)紛紜。本研究分析了98例行側(cè)頸淋巴結(jié)清掃術(shù)的PMTC患者,其側(cè)頸轉(zhuǎn)移率為72.45%,明顯高于中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移率,可能是因術(shù)前B超為術(shù)式的選擇提供了診斷意義。本組分析顯示高分辨率B超對(duì)診斷側(cè)頸淋巴結(jié)轉(zhuǎn)移的靈敏度達(dá)92.96%,男性及中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移均為側(cè)頸淋巴結(jié)轉(zhuǎn)移的危險(xiǎn)因素,而且隨著中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移數(shù)目增多,側(cè)頸淋巴結(jié)轉(zhuǎn)移率增加。有研究表明當(dāng)中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移數(shù)目超過(guò)3枚時(shí),甲狀腺乳頭狀癌患者的10年無(wú)復(fù)發(fā)生存率較高[14]。本研究建議對(duì)于男性、術(shù)前B超診斷有側(cè)頸轉(zhuǎn)移或術(shù)中發(fā)現(xiàn)中央?yún)^(qū)轉(zhuǎn)移淋巴結(jié)數(shù)目超過(guò)3枚的患者,應(yīng)行預(yù)防性側(cè)頸淋巴結(jié)清掃術(shù)。
Mizrachi等[15]發(fā)現(xiàn),術(shù)前B超對(duì)中央?yún)^(qū)淋巴結(jié)轉(zhuǎn)移診斷的靈敏度和特異度分別為95%和90%。Hwang等[16]發(fā)現(xiàn),術(shù)前B超對(duì)側(cè)頸淋巴結(jié)轉(zhuǎn)移診斷的靈敏度和特異度分別為93.8%和80.0%。本研究應(yīng)用術(shù)前超聲評(píng)估,發(fā)現(xiàn)高分辨率B超對(duì)側(cè)頸淋巴結(jié)轉(zhuǎn)移的靈敏度、特異度、假陰性率和假陽(yáng)性率分別為92.96%、81.48%、7.04%、18.52%,具有較高的診斷符合率,而且B超具有方便廉價(jià)、無(wú)放射性的優(yōu)點(diǎn)。Hong等[17]也曾報(bào)道B超對(duì)甲狀腺微小乳頭狀癌側(cè)頸淋巴結(jié)轉(zhuǎn)移的診斷意義。因此,本研究推薦B超作為甲狀腺癌頸淋巴結(jié)轉(zhuǎn)移診斷的重要評(píng)估手段。
本研究數(shù)據(jù)為回顧性分析,尚需前瞻性研究證實(shí)。但據(jù)Carling等[18]研究提示,鑒于甲狀腺乳頭狀癌生存率較高,一項(xiàng)前瞻性臨床試驗(yàn)可能需5 840例患者,花費(fèi)近0.15億美元,完成此項(xiàng)目耗資巨大,所以對(duì)中央?yún)^(qū)淋巴結(jié)清掃的問(wèn)題至今仍是爭(zhēng)議不斷。
[1] Mao LN,Wang P,Li ZY,et al.Risk factor analysis for central nodal metastasis in papillary thyroid carcinoma[J].Oncology Let?ters,2015,9(1):103-107.
[2] Xu D,Lv X,Wang S,et al.Risk factors for predicting central lymph node metastasis in papillary thyroid microcarcinoma[J].Int J Clin Exp Pathol,2014,7(9):6199-6205.
[3] Cho SY,Lee TH,Ku YH,et al.Central lymph node metastasis in papillary microcarcinoma can be stratified according to the number,the size of metastatic foci,and the presence of desmopla?sia[J].Surgery,2014,157(1):111-118.
[4] Zhao Q,Ming J,Liu C,et al.Multifocality and total tumor diame?ter predict central neck lymph node metastases in papillary thy?roid microcarcinoma[J].Ann Surg Oncol,2013,20(3):746-752.
[5] Giugliano G,Proh M,Gibelli B,et al.Central neck dissection in differentiated thyroid cancer:technical notes[J].Acta Otorhinolar?yngol Ital,2014,34(1):9-14.
[6] Wang Wt,Gu J,Shang J,et al.Correlation analysis on central lymph node metastasis in 276 patients with cN0 papillary thyroid carcinoma[J].Int J Clin Exp Pathol,2013,6(3):510-515.
[7] Kim MK,Mandel SH,Baloch Z,et al.Morbidity following central compartment reoperation for recurrent or persistent thyroid cancer [J].Arch Otolaryngol Head Neck Surg,2004,130(10):1214-1216.
[8] Mazzaferri EL,Jhiang SM.Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer[J]. Am J Med,1994,97(5):418-428.
[9] Lee J,Song Y,Soh EY.Central Lymph Node Metastasis Is an Im?portant Prognostic Factor in Patients with Papillary Thyroid Mi?crocarcinoma[J].Journal of Korean Medical Science,2014,29(1): 48-52.
[10]Liu Z,Wang L,Yi P,et al.Risk factors for central lymph node metastasis of patients with papillary thyroid microcarcinoma:a meta-analysis[J].International Journal of Clinical and Experimen?tal Pathology,2014,7(3):932-937.
[11]Popadich A,Levin O,Smooke-Praw S,et al.A Multicenter co?hort study of total thyroidectomy and routine central lymph node dissection for cN0 papillary thyroid cancer[J].Surgery, 2011,150(6):1048-1057.
[12]Liao YX,Tang HH,Tan XG,et al.Clinical analysis of 73 cases of differentiated thyroid carcinoma reoperation[J].Chinese Jour?nal of General Surgery,2006,15(4):310-311.[廖有祥,湯恢煥,譚興國(guó),等.分化型甲狀腺癌73例再手術(shù)的臨床分析[J].中國(guó)普通外科雜志,2006,15(4):310-311.]
[13]Wu YS,Zhang L,Wang XD,et al.Multivariate regression analy?sis of papillary thyroid carcinoma prognosis[J].Chin J Clin On?col,2007,34(22):1294-1297.[吳延升,張 侖,王旭東,等.甲狀腺乳頭狀癌預(yù)后多因素分析[J].中國(guó)腫瘤臨床,2007,34(22):1294-1297.]
[14]Ricarte-Filho J,Ganly I,Rivera M,et al.Papillary thyroid carci?nomas with cervical lymph node metastases can be stratified into clinically relevant prognostic categories using oncogenic BRAF, the number of nodal metastases,and extra-nodal extension[J]. Thyroid,2012,22(6):575-584.
[15]Mizrachi A,Feinmesser R,Bachar G,et al.Value of ultrasound in detecting central compartment lymph node metastases in differen?tiated thyroid carcinoma[J].Eur Arch Otorhinolaryngol,2014,271 (5):1215-1218.
[16]Hwang HS,Orloff LA.Efficacy of preoperative neck ultrasound in the detection of cervical lymph node metastasis from thyroid cancer[J].Laryngoscope,2011,121(3):487-491.
[17]Hong YR,Yan CX,Mo GQ,et al.Conventional US,elastogra?phy,and contrast enhanced US features of papillary thyroid mi?crocarcinoma predict central compartment lymph node metastases [J].Scientific Reports,2015,13(5):7748-7755.
[18]Carling T,Carty SE,Ciarleglio MM,et al.American Thyroid As?sociation design and feasibility of a prospective randomized con?trolled trial of prophylactic central lymph node dissection for pap?illary thyroid carcinoma[J].Thyroid,2012,22(3):237-244.
(2015-02-16收稿)
(2015-03-17修回)
(編輯:邢穎)
Risk factor analysis for cervical nodal metastasis in papillary microcarcinoma
Xueyan BIAN,Shanshan SUN,Wenyu GUO,Minghui ZHAO,Lingping KONG,Lun ZHANG
Tianjin Medical University Cancer Institute and Hospital,Department of Maxillofacial&E.N.T Oncology,National Clinical Research Center of Cancer;Key Laboratory of Cancer Prevention and Therapy of Tianjin,Tianjin 300060 China.
Lun ZHANG;E-mail:zhanglun@tjmuch.com
Objective:To investigate the risk factors of central lymph node metastasis(CLNM)and lateral neck lymph node metastasis in papillary thyroid microcarcinoma(PTMC)patients,and to analyze the importance of high resolution ultrasonography in the diagnosis of lateral neck lymph node metastasis in PTMC patients.Methods:A retrospective protocol was applied,and a total of 1 037 PTMC patients were reviewed.These patients underwent central lymph node dissection or thyroidectomy with lateral neck lymph node dissection between January and November in 2013 in the Tianjin Medical University Cancer Institute and Hospital.Clinicopathological factors,namely,age,sex,primary tumor size,multifocality,bilateralism,thyroid capsular invasion,and local invasion,were analyzed. Results:CLNMs were found in 332 of 1037 patients(32.0%),and 71 out of 1037 patients had lateral neck lymph node metastasis (6.85%).In the univariate analysis,patients with the following risk factors were at high risk of CLNM(P<0.05):male,aged≤45 years old,with primary tumor size of>5 mm,multifocality,bilateralism,thyroid capsular invasion,and local invasion.Male patients with central lymph node metastasis positively showed high lateral neck lymph node metastasis rate(P<0.05)according to high-resolution ultrasonography diagnosis.The rate of lateral neck lymph node metastasis increased with increasing number of central lymph node metastases.The sensitivity and specificity of high resolution ultrasonography for lateral neck lymph node metastasis were 92.96%and 81.48% in PTMC patients.Conclusion:Prophylactic central compartment lymph node dissection needs to be performed in patients with CLNM risk factors(i.e.,male,aged≤45 years old,primary tumor size of>5 mm,multifocality,bilateralism,thyroid capsular invasion,and local invasion).The importance of high-resolution ultrasonography in diagnosing lateral neck lymph node metastasis was revealed by the results.Thus,this method should be widely popularized.Radical neck dissection should be performed in male patients who received a positive diagnosis via ultrasonography or those with PTMC who had more than three positive nodes in the central lymph node metastasis.However,given the high occurrence rate of PTMC,a prospective study needs to be conducted in the future.
papillary thyroid microcarcinoma,central compartment lymph node dissection,ultrasonography,diagnosis

10.3969/j.issn.1000-8179.20150156
天津醫(yī)科大學(xué)腫瘤醫(yī)院頜面耳鼻喉腫瘤科,國(guó)家腫瘤臨床醫(yī)學(xué)研究中心,天津市腫瘤防治重點(diǎn)實(shí)驗(yàn)室(天津市300060)
張侖 zhanglun@tjmuch.com
卞雪艷 專業(yè)方向?yàn)轭^頸部腫瘤的診療研究。
E-mail:xueyanttkl@sina.cn
猜你喜歡
現(xiàn)代畜牧科技(2021年9期)2021-10-13 06:39:14
民用飛機(jī)設(shè)計(jì)與研究(2020年4期)2021-01-21 09:15:02
電子制作(2018年18期)2018-11-14 01:48:24
山東工業(yè)技術(shù)(2016年15期)2016-12-01 05:31:22
當(dāng)代經(jīng)濟(jì)研究(2016年5期)2016-12-01 03:12:05
現(xiàn)代農(nóng)業(yè)(2016年5期)2016-02-28 18:42:46
出版與印刷(2016年3期)2016-02-02 01:20:11
中國(guó)中醫(yī)藥現(xiàn)代遠(yuǎn)程教育(2014年11期)2014-08-08 13:23:44
華北水利水電大學(xué)學(xué)報(bào)(社會(huì)科學(xué)版)(2014年3期)2014-04-16 04:38:31
終身教育研究(2014年5期)2014-02-28 01:23:06
