七氟烷預處理減輕肝癌根治術患者肝臟缺血再灌注損傷
2016-03-26 06:18:16胡禮宏陳小非韓新生陸才德寧波大學醫學院附屬李惠利醫院麻醉科浙江寧波5040西安交通大學醫學院第二附屬醫院麻醉科陜西西安70004寧波大學醫學院附屬李惠利醫院肝膽外科浙江寧波5040
中國現代醫生 2016年1期
胡禮宏 徐 霞 陳小非 韓新生 陸才德.寧波大學醫學院附屬李惠利醫院麻醉科,浙江寧波 5040;.西安交通大學醫學院第二附屬醫院麻醉科,陜西西安70004;.寧波大學醫學院附屬李惠利醫院肝膽外科,浙江寧波 5040
?
七氟烷預處理減輕肝癌根治術患者肝臟缺血再灌注損傷
胡禮宏1徐霞1陳小非1韓新生2陸才德3
1.寧波大學醫學院附屬李惠利醫院麻醉科,浙江寧波315040;2.西安交通大學醫學院第二附屬醫院麻醉科,陜西西安710004;3.寧波大學醫學院附屬李惠利醫院肝膽外科,浙江寧波315040
[摘要]目的探討七氟烷預處理對肝癌根治術患者肝臟缺血再灌注損傷的影響和機制。方法選擇2013年12月~2014年12月擇期行肝癌根治術患者60例,隨機分為對照組和觀察組,每組30例。對照組采用全憑靜脈麻醉,觀察組采用靜吸復合麻醉,于肝門阻斷前吸入2%的七氟烷30 min,洗脫15 min。于術前(T0)、手術結束(T1)、術后24 h(T2),術后3 d(T3)、5 d(T4)、7 d(T5)各個時間點取中心靜脈血,檢測丙氨酸氨基轉移酶(ALT)、門冬氨酸氨基轉移酶(AST)、超氧化物歧化酶(SOD)、丙二醛(MDA)、炎性因子TNF-α、IL-1和IL-10。記錄術后住院天數。結果與術前比較,兩組患者術后血清AST、ALT、MDA、TNF-α、IL-1濃度明顯升高(P<0.05),觀察組AST和ALT 在T2~T5等時間點,TNF-α在T1~T4等時間點,MDA和IL-1在T1~T5等時間點顯著低于對照組(P<0.05),對照組SOD水平變化不明顯;觀察組血清SOD和IL-10濃度于T1~T5時間點顯著高于對照組(P<0.05)。觀察組患者術后住院天數明顯短于對照組(P<0.05)。結論七氟烷預處理能減輕肝癌根治術患者肝臟缺血再灌注損傷,可能是通過抑制TNF-α、IL-1激活,抑制氧自由基的生成,促進IL-10的激活和釋放來達到的。
[關鍵詞]七氟烷;預處理;肝癌根治術;缺血再灌注損傷
浙江省寧波市衛生局醫學科技計劃項目(2013A01)
肝癌根治術時為減少出血,在切除之前需阻斷肝門,造成不同程度的肝臟缺血再灌注損傷,而對肝臟缺血再灌注損傷的保護研究是目前基礎和臨床研究的熱點。七氟烷是目前臨床上常用的吸入麻醉藥,可以安全應用于患者,大量的研究表明七氟烷能減輕心、腦、腎等臟器的缺血性損傷[1-15],有報道稱七氟烷預處理能減輕大鼠肝臟缺血再灌注損傷[16,17],這些研究均為基礎性研究,雖七氟烷在臨床麻醉應用廣泛,常被用于肝臟手術中,但尚未見到有關七氟烷預處理對手術患者肝臟缺血再灌注損傷影響的相關研究報道,故我們通過對擇期行肝癌根治術患者行七氟烷缺血預處理,探討七氟烷預處理對肝癌根治術患者肝臟缺血再灌注損傷的保護作用和機制,為臨床減輕臟器缺血再灌注損傷提供新方法和依據。
1 資料與方法
1.1臨床資料
選擇我院2013年12月~2014年12月擇期行肝癌根治術患者60例,經醫院倫理委員會批準,患者和家屬簽署知情同意書。入選標準:美國麻醉醫師分級ASAⅠ~Ⅱ級,術前肝功能正常,無轉移,無肝膽手術史,無心肺腎等重要臟器疾病。排除標準:術前肝功能異常,合并心、肺、腎等重要臟器疾病及精神疾病史患者,對七氟烷類吸入麻醉過敏患者。左半肝31例,右半肝29例;男35例,女25例,年齡35~65歲,體質量45~80(55.58±10.75)kg,入院后編號采用隨機數字表法分為對照組和觀察組,每組30例。
1.2方法
兩組患者術前禁飲禁食,術前常規行橈動脈穿刺置管和右頸內靜脈穿刺置管,兩組麻醉誘導方法一致,均采用靜脈快誘導:咪達唑侖0.05 mg/kg,芬太尼4 μg/kg,羅庫溴銨0.6 mg/kg,丙泊酚2 mg/kg,經口氣管插管,連接BLease8500呼吸機,間歇正壓通氣,潮氣量8~10 mL/kg,呼吸頻率12 bpm,術中維持PETCO230~40 cmH2O。
對照組術中麻醉維持采用全憑靜脈麻醉,丙泊酚8000 μg/(kg·h),瑞芬太尼,順勢阿曲庫銨1 μg/(kg·h)。觀察組采用靜吸復合麻醉,靜脈維持采用丙泊酚8000 μg/(kg·h),瑞芬太尼,順勢阿曲庫銨1 μg/(kg·h),肝門阻斷前吸入2%的七氟烷30 min,洗脫15 min,于肝門阻斷前完成。術中持續監測收縮壓(SBP)、舒張壓(DBP)、平均動脈壓(MAP)、心電圖(ECG)、心率(HR)、腦電雙頻譜指數(BIS)、脈搏氧飽和度(SPO2)、呼氣末二氧化碳(PETCO2)、中心靜脈壓(CVP),術中維持BIS50(40~60)左右。術中肝門阻斷采用Pringle法[18]。
1.3觀察指標
于術前(T0),手術結束時(T1),術后1 d(T2)、3 d (T3)、5 d(T4)、7 d(T5)各個時間點取中心靜脈血,采用全自動生化檢測儀檢測肝功能指標丙氨酸氨基轉移酶(ALT)、門冬氨酸氨基轉移酶(AST);采用黃嘌呤氧化酶法測定血清超氧化物歧化酶(SOD);采用硫代巴比妥酸(TBA)法測定血清脂質過氧化代謝產物丙二醛(MDA);采用ELISA法檢測炎性因子TNF-α、IL-1、IL-10。記錄阻斷次數、時間、出血量、手術時間和術后住院天數等。
1.4統計學方法
應用SPSS14.0統計學軟件進行處理,計量資料以均數±標準差(±s)表示,組間比較用兩樣本均數t檢驗,組內比較用單因素方差分析,計數資料采用χ2檢驗,以P<0.05為差異有統計學意義。
2 結果
2.1一般資料
兩組患者性別、體重、阻斷次數、時間、手術時間、出血量等一般資料比較,差異無統計學意義(P>0.05)。見表1。
2.2兩組患者血清肝功能指標的變化情況
兩組患者血清AST和ALT于術后明顯升高,于術后1 d達到高峰,術后3 d開始下降,觀察組于術后7 d恢復正常,而對照組尚未恢復。兩組在T0和T1點比較,無顯著差異,觀察組在T2、T3、T4和T5等時間點顯著低于對照組(P<0.05)。見表2。
2.3兩組患者SOD和MDA的變化情況
兩組患者血清SOD濃度在術后均有升高,術后24 h達到高峰,術后3 d開始下降,對照組各時間點比較無顯著差異,觀察組術后各時間點均高于術前,在T1、T2、T3、T4和T5顯著高于對照組(P<0.05)。對照組血清MDA濃度于術后開始升高,術后1 d達高峰,3 d開始下降,T2、T3、T4顯著高于T0(P<0.05),觀察組血清MDA濃度變化趨勢同對照組,在T4恢復至術前水平,觀察組在T1、T2、T3、T4和T5時間點顯著低于對照組(P<0.05)。見表3。
表1 兩組患者一般資料(±s,n=30)

表1 兩組患者一般資料(±s,n=30)
對照組觀察組t/χ2值P 18/12 17/13 0.07 >0.05 15/15 16/14 0.07 >0.05 50.35±10.65 51.43±10.89 0.39 >0.05 54.36±10.56 55.23±10.12 0.33 >0.05 1.59±0.37 1.62±0.38 0.31 >0.05 12.59±2.61 13.23±2.53 0.97 >0.05 123.50±15.58 125.65±16.67 0.52 >0.05 224.86±21.61 223.35±22.65 0.26 >0.05組別 性別(男/女) 左半肝/右半肝 年齡(歲) 體重(kg) 阻斷次數(次) 阻斷時間(min) 手術時間(min) 出血量(mL)
表2 兩組患者血清肝功能指標的變化情況(±s,n=30)
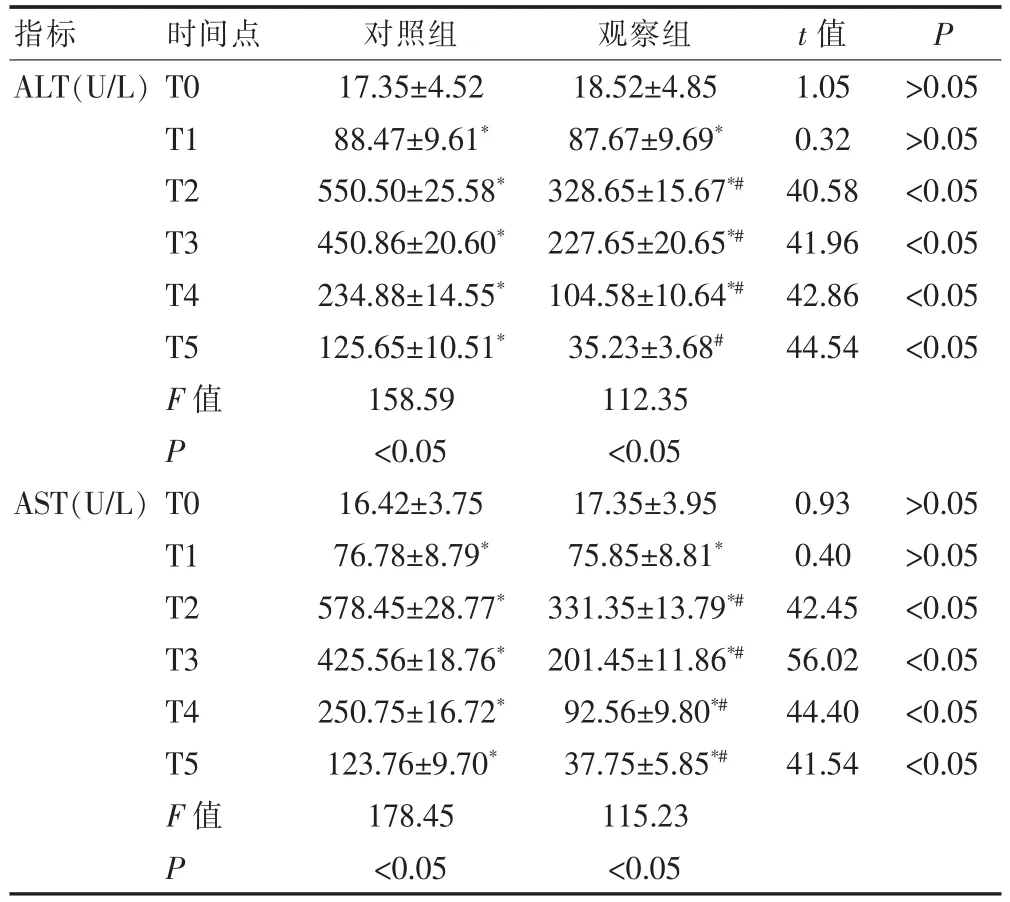
表2 兩組患者血清肝功能指標的變化情況(±s,n=30)
注:與組內T0比較,*P<0.05,與對照組比較,﹟P<0.05
ALT(U/L)AST(U/L)T0 T1 T2 T3 T4 T5 F值P T0 T1 T2 T3 T4 T5 F值P 17.35±4.52 88.47±9.61*550.50±25.58*450.86±20.60*234.88±14.55*125.65±10.51*158.59 <0.05 16.42±3.75 76.78±8.79*578.45±28.77*425.56±18.76*250.75±16.72*123.76±9.70*178.45 <0.05 18.52±4.85 87.67±9.69*328.65±15.67*#227.65±20.65*#104.58±10.64*#35.23±3.68#112.35 <0.05 17.35±3.95 75.85±8.81*331.35±13.79*#201.45±11.86*#92.56±9.80*#37.75±5.85*#115.23 <0.05 1.05 0.32 40.58 41.96 42.86 44.54 0.93 0.40 42.45 56.02 44.40 41.54 >0.05 >0.05 <0.05 <0.05 <0.05 <0.05 >0.05 >0.05 <0.05 <0.05 <0.05 <0.05指標 時間點 對照組 觀察組 t值 P
表3 兩組患者血清SOD和MDA的變化情況(±s,n=30)
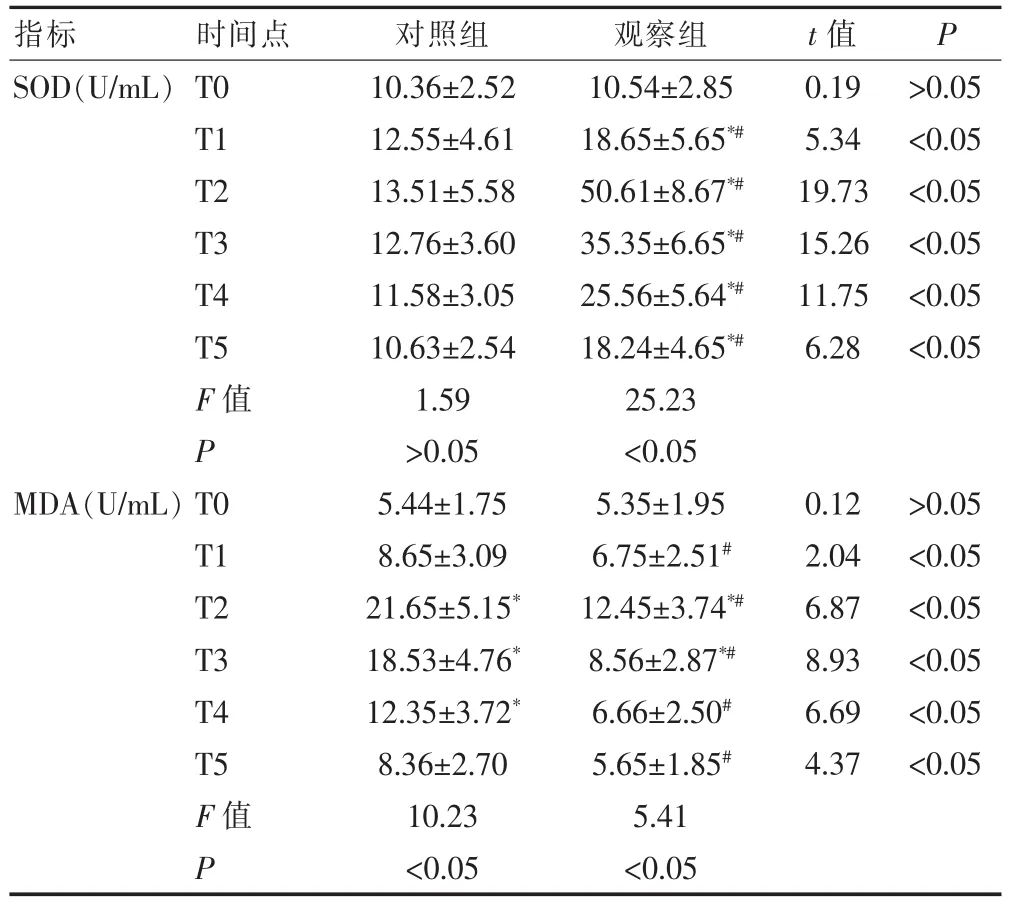
表3 兩組患者血清SOD和MDA的變化情況(±s,n=30)
注:與組內T0比較,*P<0.05,與對照組比較,#P<0.05
SOD(U/mL)MDA(U/mL)T0 T1 T2 T3 T4 T5 F值P T0 T1 T2 T3 T4 T5 F值P 10.36±2.52 12.55±4.61 13.51±5.58 12.76±3.60 11.58±3.05 10.63±2.54 1.59 >0.05 5.44±1.75 8.65±3.09 21.65±5.15*18.53±4.76*12.35±3.72*8.36±2.70 10.23 <0.05 10.54±2.85 18.65±5.65*#50.61±8.67*#35.35±6.65*#25.56±5.64*#18.24±4.65*#25.23 <0.05 5.35±1.95 6.75±2.51#12.45±3.74*#8.56±2.87*#6.66±2.50#5.65±1.85#5.41 <0.05 0.19 5.34 19.73 15.26 11.75 6.28 0.12 2.04 6.87 8.93 6.69 4.37 >0.05 <0.05 <0.05 <0.05 <0.05 <0.05 >0.05 <0.05 <0.05 <0.05 <0.05 <0.05指標 時間點 對照組 觀察組 t值 P
2.4兩組患者炎性因子的變化
兩組患者TNF-α、IL-1濃度于術后明顯升高(P<0.05),于術后1 d達到高峰,術后3 d開始下降。觀察組血清TNF-α濃度于T2、T3、T4時間點,IL-1于T2、T3、T4和T5時間點顯著低于對照組(P<0.05),于術后5 d基本恢復正常。對照組血清IL-10濃度術后升高,T2顯著高于T0,觀察組血清IL-10濃度于術后明顯升高(P<0.05),在T1、T2、T3、T4和T5時間點的濃度值顯著高于對照組(P<0.05)。見表4。
2.5術后住院天數
對照組術后住院天數為(10.68±2.55)d,觀察組術后住院天數為(8.98±1.64)d,觀察組顯著短于對照組,差異有統計學意義(t=3.09,P<0.05)。
表4 兩組患者炎性因子的變化(±s,n=30)
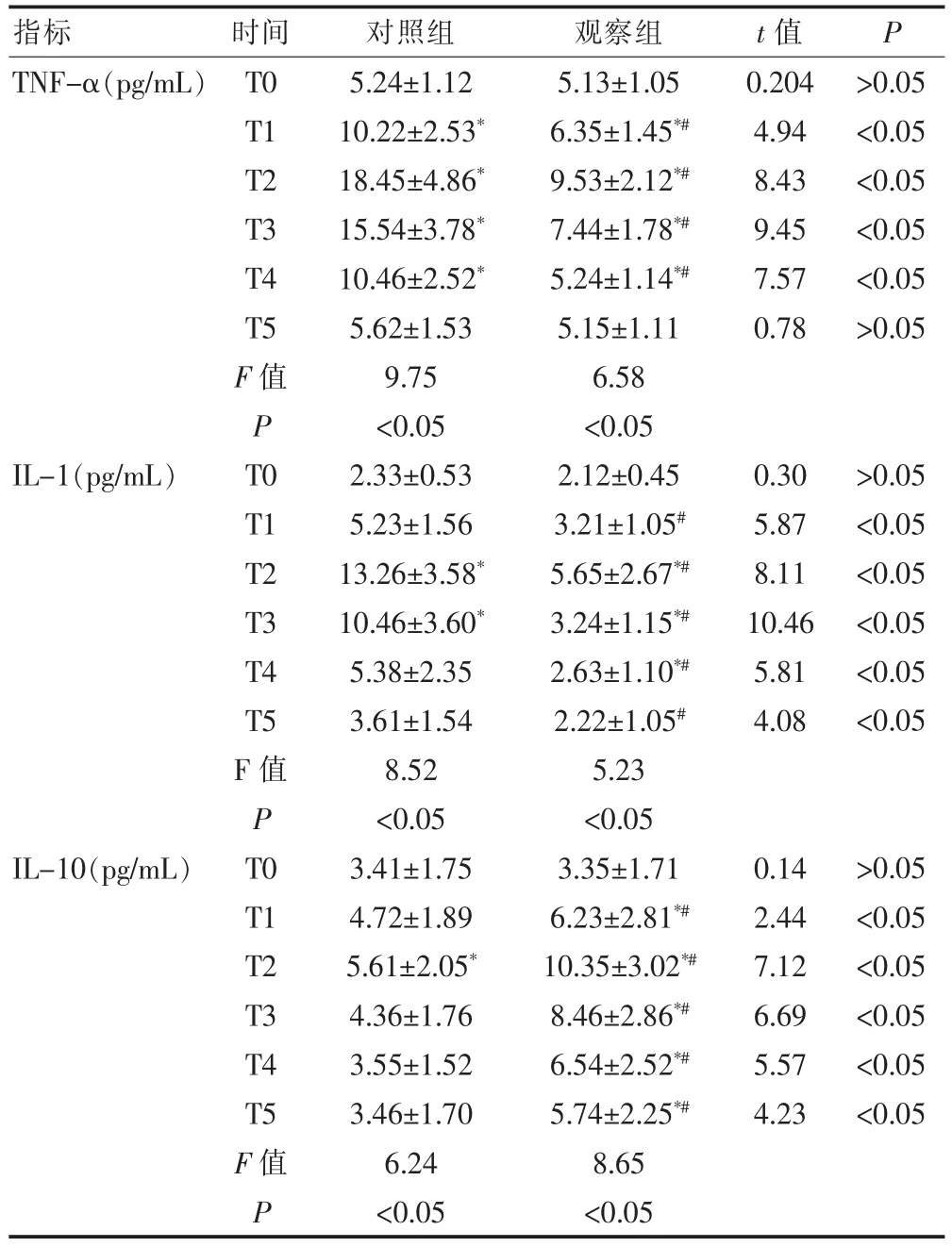
表4 兩組患者炎性因子的變化(±s,n=30)
注:與組內T0比較,*P<0.05,與對照組比較,#P<0.05
TNF-α(pg/mL)IL-1(pg/mL)IL-10(pg/mL)T0 T1 T2 T3 T4 T5 F值PT 0 T1 T2 T3 T4 T5 F值PT 0 T1 T2 T3 T4 T5 F值 P 5.24±1.12 10.22±2.53*18.45±4.86*15.54±3.78*10.46±2.52*5.62±1.53 9.75 <0.05 2.33±0.53 5.23±1.56 13.26±3.58*10.46±3.60*5.38±2.35 3.61±1.54 8.52 <0.05 3.41±1.75 4.72±1.89 5.61±2.05*4.36±1.76 3.55±1.52 3.46±1.70 6.24 <0.05 5.13±1.05 6.35±1.45*#9.53±2.12*#7.44±1.78*#5.24±1.14*#5.15±1.11 6.58 <0.05 2.12±0.45 3.21±1.05#5.65±2.67*#3.24±1.15*#2.63±1.10*#2.22±1.05#5.23 <0.05 3.35±1.71 6.23±2.81*#10.35±3.02*#8.46±2.86*#6.54±2.52*#5.74±2.25*#8.65 <0.05 0.204 4.94 8.43 9.45 7.57 0.78 0.30 5.87 8.11 10.46 5.81 4.08 0.14 2.44 7.12 6.69 5.57 4.23 >0.05 <0.05 <0.05 <0.05 <0.05 >0.05 >0.05 <0.05 <0.05 <0.05 <0.05 <0.05 >0.05 <0.05 <0.05 <0.05 <0.05 <0.05指標 時間 對照組 觀察組 t值 P
3 討論
肝臟手術為了減少出血和術野清潔,常阻斷肝門,開放后就會造成一定程度的肝臟缺血再灌注損傷,造成肝臟缺血再灌注損傷的機制有氧自由基及其引發的脂質過氧化反應、鈣離子超載、中性粒細胞的聚集、細胞因子炎性因子的釋放等[19],常采用缺血預處理或后處理針對上述機制來減少缺血再灌注損傷,這也是目前基礎和臨床研究的熱點。七氟烷是目前臨床上常用的吸入麻醉藥,可安全應用于麻醉誘導和維持。研究表明,七氟烷對心、腦、腎等重要臟器的缺血性損傷具有保護作用[1-15]。有報道稱,七氟烷預處理能減輕大鼠肝臟缺血再灌注損傷[16,17],這些研究均為基礎性研究,我們通過對擇期行肝癌根治術患者,吸入2%的七氟烷行缺血預處理,探討七氟烷預處理對肝癌根治術患者肝臟缺血再灌注損傷的影響和機制,為臨床減輕臟器缺血再灌注損傷提供新方法和依據。
本研究中兩組患者肝功能指標于術后明顯升高,于術后1 d達到高峰,術后3 d開始下降,觀察組于術后7 d恢復正常,而對照組尚未恢復。術后觀察組顯著低于對照組(P<0.05),觀察組住院天數明顯短于對照組(P<0.05),充分說明觀察組患者通過七氟烷預處理肝臟缺血再灌注損傷較輕,術后恢復較快,術后住院天數減少。
肝臟缺血再灌注損傷時機體可通過多種途徑產生大量氧自由基,引發脂質過氧化反應,MDA是自由基攻擊生物膜引發的脂質過氧化反應產物,其含量可反映脂質過氧化程度,間接地反映出細胞受自由基攻擊和損傷的程度,超氧化物歧化酶(SOD)是氧自由基清除劑,可以有效清除氧自由基[19,20]。本研究結果顯示,兩組血清MDA濃度于術后明顯升高,而對照組在T1、T2、T3、T4和T5時間點顯著高于觀察組,血清SOD濃度對照組各時間點比較無顯著差異,而在觀察組術后均顯著升高,顯著高于對照組,說明七氟烷預處理可以刺激SOD的活性,有效清除氧自由基,抑制過氧化,減輕肝臟損傷。
肝臟缺血再灌注可以引起炎性因子TNF-α和IL-1的大量產生和釋放,進而多種途徑造成肝臟損傷,TNF-α和IL-1之間還可以相互促進釋放,進一步加重損傷[19,21]。本研究顯示,觀察組血清TNF-α濃度于T1、T2、T3和T4時間點,IL-1在T1、T2、T3、T4 和T5時間點顯著低于對照組,說明七氟烷預處理可以抑制炎性因子TNF-α和IL-1的激活和釋放,從而間接減輕缺血再灌注損傷。IL-10是一種抗炎細胞因子,它可以通過抑制NF-κB和TNF-α的活性減輕炎癥反應。本研究中,觀察組血清IL-10濃度顯著高于對照組,說明七氟烷預處理可以激活和釋放炎性因子IL-10,從而減輕肝臟的損傷。
本研究表明,2%的七氟烷預處理可以減輕肝癌根治術患者肝臟缺血再灌注損傷,其可能是通過抑制氧自由基的生成,進而抑制脂質過氧化反應,抑制炎性因子TNF-α和IL-1的激活和釋放,激活炎性因子IL-10等途徑來實現的。
[參考文獻]
[1] Thomas L,Sean C,Thomas C,et al. Sevoflurane protects against renal ischemia and reperfusion injury in mice via the transforming growth factor-β1 pathway[J]. Am J Physiol Renal Physiol,2008,295(1):F128-F136.
[2] Zhou S,Liao W,Yang L,et al. Effects of sevoflurane pretreatment on renal Src and FAK expression in diabetic rats after renal ischemia/reperfusion injury[J]. Mol Cell Biochem,2013,384(1-2):203-211.
[3] Lee H,Park YH,Jeon YT,et al. Sevoflurane post-conditioning increases nuclear factor erythroid 2-related factor and haemoxygenase-1 expression via protein kinase C pathway in a rat model of tran sient global cerebral ischaemia[J]. Br J Anaesth,2015,114(2):307-318.
[4] Yang Q,Yan W,Li X,et al. Activation of canonical notch signaling pathway is involved in the ischemic tolerance induced by sevoflurane preconditioning in mice [J]. Anesthesiology,2012,117(5):996-1005.
[5] Ye R,Yang Q,Kong X,et al.Sevoflurane preconditioning improves mitochondrial function and long-term neurologic sequelae after transient cerebral ischemia:role of mito chondrial permeability transition[J]. Critical Care Medicine,2012,40(9):2685-2693.
[6] Chen Y,Nie H,Tian L,et al. Sevoflurane preconditioninginduced neuroprotection is associated with Akt activation via carboxy-terminal modulator protein inhibition[J]. Br J Anaesth,2015,114(2):327-335.
[7] Chappell D,Heindl B,Jacob M,et al. Sevoflurane reduces leukocyte and platelet adhesion after ischemia-reperfusion by protecting the endothelial glycocalyx[J]. Anesthesiology,2011,115(3):483-491.
[8] Wang J,Meng F,Cottrell JE,et al. Metabotropic actions of the volatile anaesthetic sevoflurane increase protein kinase M synthesis and induce immediate preconditioningprotection of rat hippocampal slices[J]. The Journal of Physiology,2012,590(16):4093-4107.
[9] Li X,Luo P,Wang F,et al. Inhibition of N-myc downstreamregulated gene-2 is involved in an astrocyte-specific neuroprotection induced by sevofluranepreconditioning [J]. Anesthesiology,2014,121(3):549-562.
[10] Ye R,Yang Q,Kong X,et al. Sevoflurane preconditioning improves mitochondrial function and long-term neurologic sequelae after transient cerebral ischemia:Role of mitochondrialpermeabilitytransition[J].Critical Care Medicine,2012,40(9):2685-2693.
[11] Luo C,Yuan D,Zhao W,et al. Sevoflurane ameliorates intesting ischemia-reperfusion induced lung injury by inhibiting the synergistic action between mast cell activation and oxidative stress[J]. Mol Med Rep,2015,2(1):1082-1090.
[12] Gong JS,Yao YT,Fang NX,et al. Sevoflurane postconditioning attenuates reperfusion-induced ventricular arrhythmias in isolated rat hearts exposed to ischemia/ reperfusion injury[J]. Molecular Biology Reports,2012,39 (6):6417-6425.
[13] Xie H,Liu Q,Qiao S,et al. Delayed cardioprotection by sevoflurane preconditioning:a novel mechanism via inhibiting beclin 1-mediated autophagic cell death in cardiac myocytes exposed to hypoxia/reoxygenation injury[J]. Int J Clin Exp Pathol,2015,8(1):217-226.
[14] Shiomi M,Miyamae M,Takemura G,et al.Sevoflurane induces cardioprotection through reactive oxygen speciesmediated upregulation of autophagy in isolated guinea pig hearts[J]. Anesth,2014,28(4):593-600.
[15] Fradorf J,Huhn R,Weber NC,et al. Sevoflurane-induced preconditioning:impact of protocol and aprotinin administration on infarct size and endothelial nitric-oxide synthase phosphorylation in the rat heart in vivo[J]. Anesthesiology,2010,113(6):1289-1298.
[16] Beck-Schimmer B,Breitenstein S,Urech S,et al. A randomized controlLed trial on pharmacological preconditioning in liver surgery using a volatile anesthetic[J]. Ann Surg,2008,248(6):909-918.
[17] Ofluoglu E,Kerem M,Utebey G,et al. Hepatic energy metabolism and the differential protective effects of sevoflurane and isoflurane anesthesia in a rat hepatic ischemia-reperfusion injury model[J]. Anesth Analg,2008,106(3):830-837.
[18]胡禮宏,韓新生,郭建榮.雌激素與雌激素受體在大鼠肝臟缺血再灌注損傷中的作用[J].中國臨床藥理學雜志,2013,27(3):187-190.
[19]胡禮宏,韓新生.肝臟缺血再灌注損傷機制研究進展[J].陜西醫學雜志,2008,37(6):739-741.
[20] Liu Y,Yang L,Tao K,et al. Protective effects of hydrogen enriched saline on liver ischemiareperfusion injury by reducing oxidative stress and HMGB1 release[J]. BMC Gastroenterology,2014,14(1):12.
[21] Jiao S,Sun K,Chen X. Inhibition of tumor necrosis factor alpha reduces the outgrowth ofhepatic micrometastasis of colorectal tumors in a mouse model of liverischemia -reperfusion injury[J]. Journal of Biomedical Science,2014,21(1):1.
Sevoflurane pretreatment reduces the liver ischemia reperfusion injury of patients experiencing liver cancer radical operation
HU Lihong1XU Xia1CHEN Xiaofei1HAN Xinsheng2LU Caide3
1.Department of Anesthesiology, Ningbo University Medical School Affiliated Lihuili Hospital, Ningbo 315040, China; 2.Department of Anesthesiology, Xi'an Jiaotong University Medical School Second Affiliated Hospital, Xi’an 710004, China; 3.Department of Hepatobiliary Surgery, Ningbo University Medical School Affiliated Lihuili Hospital, Ningbo 315040, China
[Abstract]Objective To explore the impact and mechanism of sevoflurane pretreatment on liver ischemia reperfusion injury of patients experiencing liver cancer radical operation. Methods Sixty patients receiving liver cancer radical operation from December 2013 to December 2014 were selected and randomly and equally divided into control group and observation group. Patients in the control group were given total intravenous anesthesia, while for patients in the observation group, intravenous inhalational anesthesia was applied: 2%sevoflurane inhalation for 30 min before hepatic portal occlusion and elution for 15 min. Central venous blood was sampled at pre-operation(T0), 0 h(T1), 24 h(T2), 3 d (T3), 5 d(T4), and 7 d(T5)after operation to detect alanine aminotransferase(ALT), aspartate aminotransferase(AST), superoxide dismutase(SOD), Malondialdehyde(MDA), and inflammatory factor TNF-α, IL-1 and IL-10. And the length of hospital stay after operation was also recorded. Results Compared to those before operation, serum AST, ALT, MDA, TNF-α and IL-1 of both groups were significantly increased(P<0.05). AST and ALT at T2~T5, TNF-α at T1~T4, and MDA and IL-1 at T1~T5 of the observation group were significantly lower than those of the control group(P<0.05). SOD of the control group had no evident change, and serum SOD and IL-10 at T1~T5 of the observation group were significantly higher than those of the control group(P<0.05). The hospital stay of patients in the observation group were significantly shorter than those of the control group(P<0.05). Conclusion Sevoflurane pretreatment can reduce the liver ischemia reperfusion injury of patients experiencing liver cancer radical operation, probably by inhibiting the activation of TNF-α and IL-1 and the production of oxygen free radical, and promoting the activation and release of IL-10.
[Key words]Sevoflurane; Pretreatment; Liver cancer radical operation; Ischemia reperfusion injury
收稿日期:(2015-07-09)
[基金項目]浙江省醫學會臨床科研資金項目(2011ZYC-A52);
[中圖分類號]R614
[文獻標識碼]A
[文章編號]1673-9701(2016)01-0001-04