糖尿病腹部手術中全麻復合硬膜外麻醉和全麻兩種麻醉方法的療效對比
2016-05-14 05:38:13倪利平
糖尿病新世界 2016年8期
關鍵詞:糖尿病
倪利平
DOI:10.16658/j.cnki.1672-4062.2016.08.086
[摘要] 目的 探討全麻復合硬膜外麻醉和全麻用于糖尿病腹部手術中的療效對比分析。 方法 接受糖尿病腹部手術中的老年患者62例,隨機分為兩組,觀察組采全麻復合硬膜外麻醉,對照組采用全麻。觀察兩組麻醉前后血流動力學變化。結果 全麻復合硬膜外麻醉優于全麻(90.3% vs83.9%)。差異無統計學意義(P>0.05)。術后認知障礙,深靜脈栓塞發生率低于全麻(P<0.05)。結論 全麻復合硬膜外麻醉,全麻均可用于老年糖尿病腹部手術,但前者并發癥較少。
[關鍵詞] 糖尿病;全麻復合硬膜外麻醉;全麻;療效對比
[中圖分類號] R587.1 [文獻標識碼] A [文章編號] 1672-4062(2016)04(b)-0086-02
Diabetes Abdominal Surgery in General Anesthesia Compound Epidural Anesthesia and General Anesthesia the Curative Effect of two Methods of Anesthesia
NI Li-ping
Taian Center of Mental Health,Taian,Shandong Province, 271000 China
[Abstract] Objective Discusses general anesthesia compound epidural anesthesia and general anesthesia for curative effect analysis in diabetes abdominal surgery. Methods Diabetes abdominal surgery in 62 cases of elderly patients and randomly divided into 2 groups, the observation group in general anesthesia compound epidural anesthesia, the control group with general anesthesia. Observe two groups hemodynamic changes before and after anesthesia. Result General anesthesia compound epidural anesthesia is superior to general anesthesia (90.3% vs83.9 %). No statistical significance (P > 0.05). Postoperative cognitive impairment, lower incidence of deep vein thrombosis during anesthesia (P < 0.05). Conclusion General anesthesia compound epidural anesthesia, general anesthesia can be used in elderly diabetes abdominal surgery, but the former with less complications.
[Key words] Diabetes;General anesthesia compound epidural anesthesia;General anesthesia;Effect of contrast
糖尿病腹部手術是老年患者常見的手術之一,因存在術中出血量大,創傷刺激大等特點,加之老年患者常合并高血壓,冠心病等基礎疾病,增加了麻醉風險。在麻醉方式的選擇上存在爭議。我科采用全麻復合硬膜外麻醉和全麻用于糖尿病腹部手術進行比較,現報道如下。
1 資料與方法
1.1 一般資料
選擇2013年1—6月施行糖尿病腹部手術老年患者62例,ASAⅡ~Ⅲ級。男性38例,女性24例。年齡65~82歲,平均年齡72歲。隨機分為A組全麻復合硬膜外麻醉組,B組全麻組。各組均為31例患者。兩組病人年齡,性別進行對比,差異無統計學意義。所有病人均完善檢查及控制基礎疾病。麻醉前均簽定知情同意書。
1.2 麻醉方法
于麻醉前30 min肌注0.5 mg阿托品,0.1 mg苯巴比妥鈉。司克林2 mg/kg、萬可松0.08 mg/kg、芬太尼5~8 ug/kg快速誘導之后插入氣管,接入麻醉劑控制呼吸,循環參數穩定。觀察組吸入異氟醚,采用靜脈滴注普魯卡因1%加司克林0.1%混合液。實驗組在進行麻醉誘導前進行T7~T9椎間隙硬外穿刺,采用5 mL利多卡因(1%~1.5%)為實驗,5 min后安全則分次注入10~15 mL利多卡因(1%~1.5%)。術中如需追加麻醉藥,加吸異氟醚。
1.3 觀察指標
(1)麻醉效果 根據中華醫學會制定標準判定,Ⅰ級麻醉效果良好,肌松和鎮痛效果佳。Ⅱ級鎮痛良好,肌松較低。Ⅲ級鎮痛較低,肌松較差。Ⅳ級鎮痛,肌松效果均較差。Ⅴ級無麻醉效果;(2)麻醉前后血流動力學改變。心率,血壓,血氧飽和度觀察。(3)并發癥:認知功能障礙,深靜脈栓塞(DVT)。
1.4 統計方法
所有數據采用SPSS 11.0軟件進行統計學處理。計數資料采用χ2檢驗。P<0.05為差異有統計學意義。
2 結果
2.1 兩組患者均順利完成手術,無麻醉死亡病例
比較手術時間,出血量差異無統計學意義。
2.2 兩組麻醉效果比較
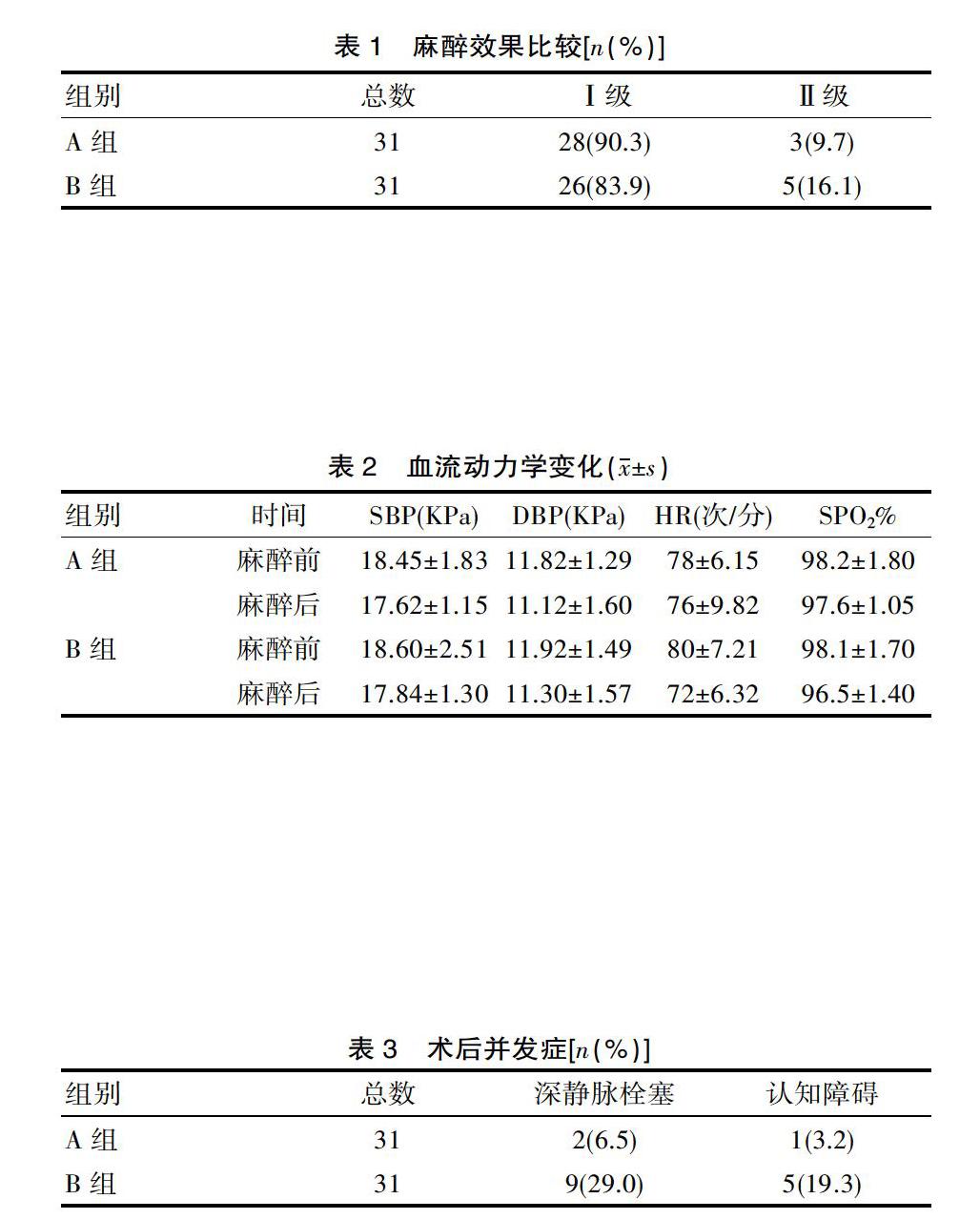
均在Ⅰ~Ⅱ級。其中A組Ⅰ級90.3%,Ⅱ級9.7%。B組Ⅰ級83.9%,Ⅱ級16.1%。A組Ⅰ級高于B組,但差異無統計學意義(P>0.05)。見表1。
2.3 血流動力學變化
SBP,DBP,HR,SO2麻醉前后比較,差異無統計學意義。見表2。
2.4 術后并發癥比較
A組深靜脈栓塞2例,認知障礙1例,B組深靜脈栓塞9例,認知障礙5例。A組明顯低于B組,P<0.05,差異有統計學意義。見表3。
3 討論
全麻復合硬膜外麻醉兼顧了腰麻的靈活性和硬膜外麻醉的可靠性,起到了起效快,阻滯完全的作用[1]。有研究表明,在擴容處理的前提下,全麻復合硬膜外麻醉可大大減少局麻藥物的使用,同時可有效的控制藥物的速度,有利于老年人血流動力學的控制[2]。并可很好的控制麻醉平面。
該科應用全麻復合硬膜外麻醉和全麻均取得了較好的效果。、兩組麻醉效果比較,均在Ⅰ~Ⅱ級。其中A組Ⅰ級90.3%,Ⅱ級9.7%。B組Ⅰ級83.9%,Ⅱ級16.1%。A組Ⅰ級高于B組,但P>0.05,差異無統計學意義。血流動力學,SBP,DBP,HR,SO2麻醉前后比較,差異無統計學意義。
術后并發癥,全麻復合硬膜外麻醉少于全麻。其中深靜脈栓塞發生率6.5%vs29.0%。與有關報道基本一致[3-8]。其原因與下列有關:(1)椎管內麻醉使交感神經阻滯,下腔靜脈擴張,下肢循環血流量增加,DVT不易發生[9];(2)全麻復合硬膜外麻醉減少心肺負荷,抑制血小板的激活,降低高凝狀態;(3)局麻藥有抗血栓作用,可抑制微血栓形成;(4)患者可早期下床活動,減少血栓形成。
綜上,全麻復合硬膜外麻醉及全麻均可用于老年糖尿病腹部手術,但全麻復合硬膜外麻醉并發癥少。在今后的臨床工作中可進一步觀察總結。
[參考文獻]
[1] 陳家驊.聯合腰麻硬膜外麻醉與硬膜外麻醉用于老年病人手術的比較[J].中華麻醉學雜志,2011(19):364.
[2] Khatod M,Inacio MC,Bini SA,et al.Prophylaxis anainst pulmonary embolism in patients undergoing total hip arthroplasty[J].J Bone Joint Surg Am,2011,93:1767-1772.
[3] Mauermann WJ,Shilling AM,Zuo Z.A comparison of neuraxial block versus general anesthesia for elective total hip replacement:a meta-analysis[J].Anesth Analg,2015,103(4):1018-1025.
[4] Davis F M,Medermott E,Hickton C,et al.Influence of general anesthesia on haemostasis during total hip arthroplasty[J].British Journal of Anaesthesia,2013,17(18):184-185.
[5] 熊振輝,金婭芳.全麻和單側重比重全麻復合硬膜外麻醉糖尿病腹部手術的臨床比較[J].中國現代醫生,2012(50):68-71.
[4] Burkhart CS, Steiner LA. Can postoperative cognitive dysfunction be avoided[J].Hosptial Practice(Minneap), 2012, 40(1): 214-223.
[5] 徐靜,萬燕杰,曾因明,等.中樞炎性細胞因子與認知功能損害[J].國外醫學(麻醉學與復蘇分冊) ,2005,26(2) :105-107.
[6] 程曉云,田卓敏,韓元福.烏司他丁聯合生脈注射液在老年急腹癥患者圍手術期的應用[J].實用醫院臨床雜志,2012, 9( 1) :115-118.
[7] Moller JT,Cluitmans P,Rasmussen LS,et al.Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study[J].Lancet,1998,9106(351):857-861.
[8] Tallcy JJ,Bertenshaw R,Brown DL, et al. N-[[(5-methyl-3-phenylisoxazol-4-yl)- phenyl] sulfonyl] propanamide, sodium alt,parecoxib sodium: A potent and selective inhibitor of COX-2 for parenteral administration[J].JMed Chem,2013,43:1661-1663.
[9] Cheer SM,Goa KL. Parecoxib (parecoxib sodium)[J]. Drugs,2014,61(8):1133-41.
(收稿日期:2016-01-15)
猜你喜歡
中老年保健(2022年5期)2022-08-24 02:35:42
中老年保健(2022年1期)2022-08-17 06:14:56
中老年保健(2021年5期)2021-08-24 07:07:20
中老年保健(2021年9期)2021-08-24 03:51:04
中老年保健(2021年7期)2021-08-22 07:42:16
中老年保健(2021年3期)2021-08-22 06:49:56
中老年保健(2021年11期)2021-08-22 03:15:16
中國生殖健康(2020年2期)2021-01-18 02:51:44
中國生殖健康(2018年2期)2018-11-06 07:11:04
基層中醫藥(2018年2期)2018-05-31 08:45:04