艾塞那肽聯(lián)合門冬胰島素控制血糖療效分析
2016-05-14 07:53:39楊智勇
中國現(xiàn)代醫(yī)生 2016年6期
楊智勇
[摘要] 目的 分析肥胖癥合并2型糖尿病的確診患者通過應(yīng)用艾塞那肽注射液聯(lián)合門冬胰島素注射液控制血糖和體重指數(shù)的臨床綜合效果,及縮短血糖達(dá)標(biāo)所需的時(shí)間。 方法 對我院2014年6月~2015年6月確診為2型糖尿病且體重指數(shù)(BMI)>28 kg/m2的住院患者100例,隨機(jī)分為對照組和觀察組;兩組基礎(chǔ)治療的方法均為門冬胰島素注射液連續(xù)皮下注射日基礎(chǔ)量,對照組在基礎(chǔ)治療的同時(shí)給予阿卡波糖片50 mg,每日3次,餐時(shí)嚼服;觀察組在基礎(chǔ)治療的基礎(chǔ)上應(yīng)用艾塞那肽注射液5 μg皮下注射每日2次。兩組均給予監(jiān)測指端血糖每日8次。患者住院治療30 d后觀察血糖總體控制情況,綜合評估療效。 結(jié)果 觀察組的治療后血糖控制總體優(yōu)于對照組,差異有統(tǒng)計(jì)學(xué)意義(P<0.05);觀察組糖化血紅蛋白與體重指數(shù)治療后均優(yōu)于對照組,差異有高度統(tǒng)計(jì)學(xué)意義(P<0.01),兩組均未發(fā)生嚴(yán)重低血糖病例,觀察組的血糖達(dá)標(biāo)時(shí)間較對照組顯著縮短,差異有高度統(tǒng)計(jì)學(xué)意義(P<0.01),觀察組的胰島素用量小于對照組,差異有高度統(tǒng)計(jì)學(xué)意義(P<0.01)。 結(jié)論 肥胖癥合并2型糖尿病患者采用艾塞那肽注射液聯(lián)合門冬胰島素注射液控制血糖可使血糖達(dá)標(biāo)率增高,體重指數(shù)穩(wěn)中有降,血糖達(dá)標(biāo)時(shí)間縮短,讓患者最大限度受益,血糖達(dá)標(biāo)的同時(shí)避免了體重增加的弊端,減少和防止了糖尿病并發(fā)癥的發(fā)生,較口服阿卡波糖片聯(lián)合門冬胰島素注射液療效顯著,安全可靠,值得臨床推廣。
[關(guān)鍵詞] 艾塞那肽注射液;門冬胰島素;阿卡波糖片;2型糖尿病;胰島素泵
[中圖分類號] R587.1 [文獻(xiàn)標(biāo)識碼] B [文章編號] 1673-9701(2016)06-0029-05
Effect analysis on exenatide combined with insulin aspart in blood glucose control
YANG Zhiyong
Department of Internal Medicine, Datong Huayang Hospital, Xining 810000, China
[Abstract] Objectives To analyze the clinical effect of exenatide injection combined with insulin aspart injection in controlling of blood glucose and weight indices and the reaching-standard time of blood glucose among 50 patients with obesity and type Ⅱ diabetes. Methods A total of 100 patients diagnosed as type Ⅱ diabetes with BMI >28 kg/m2 treated in our hospital from June 2014 to June 2015 were selected and randomly divided into the control group and the observation group. Patients in both groups were treated by daily insulin aspart injection continuous and subcutaneous basal therapy. Patients in the control group were additionally given acarbose tablet 50 mg, tid, chewing at meals; while patients in the observation group were additionally given exenatide subcutaneous injection, 5 μg, bid. Blood glucose of patients in both groups were monitored through finger tips for eight times per day. The overall control of blood glucose and curative effect were assessed after 30 days of hospitalization. Results The blood glucose control in general of observation group after treatment was better than the control group, the difference was statistically significant(P<0.05); glycosylated hemoglobin and body mass index (BMI) of observation group were better than control group after treatment, the difference was statistically significant(P<0.01), two groups were not cases of severe hypoglycemia, the time of blood glucose control of observation group was significantly shortened, the difference was statistically significant(P<0.01), the insulin dosage of observation group was less than the control group, the difference was statistically significant(P<0.01). Conclusion Exenatide subcutaneous injection combined with insulin aspart injection can increase the rate of reaching the standard of blood glucose among patients with obesity and type Ⅱ diabetes, and can keep the weight of patients stable with a slight decline, shorten the reaching-standard time, and benefit the patients to the maximum limit that effectively controlling blood glucose and avoiding gaining weight, as well as reducing the incidence of diabetic complications. Compared with oral administration of acarbose tablet combination of insulin aspart injection has more significant effectiveness and accredited safety, which is worthy to be promoted.
[Key words] Exenatide injection; Insulin aspart; Acarbose tablets; Type Ⅱ diabetes; Insulin pump
2型糖尿病是常見的代謝性疾病,我國糖尿病患者數(shù)目居世界首位,糖尿病給我國造成的的經(jīng)濟(jì)負(fù)擔(dān)也逐年上升[1]。其主要發(fā)病原因?yàn)檫z傳與環(huán)境因素,胰島素抵抗和β細(xì)胞功能缺陷、胰島素α細(xì)胞功能異常和胰高血糖樣肽-1(GLP-1)分泌缺陷。依據(jù)2型糖尿病的發(fā)病病因,補(bǔ)充外源胰島素和GLP-1受體激動(dòng)劑是有效的。為了更好的控制2型糖尿病患者的血糖,減少2型糖尿病患者的并發(fā)癥的發(fā)生、發(fā)展在臨床治療過程中十分重要,本研究通過應(yīng)用艾塞那肽注射液5 μg,每日2次,皮下注射,聯(lián)合應(yīng)用門冬胰島素注射液連續(xù)皮下持續(xù)泵入基礎(chǔ)量治療控制血糖和體重指數(shù)的臨床綜合效果,現(xiàn)報(bào)道如下。
1 資料與方法
1.1 一般資料
選取2014年6月~2015年6月我院確診為2型糖尿病并且體重指數(shù)>28 kg/m2的患者100例,在患者了解了實(shí)驗(yàn)全過程并且在知情同意的情況下實(shí)施,符合1999年WHO診斷及分型標(biāo)準(zhǔn),F(xiàn)PG>11.1 mmol/L,年齡20~65歲,男性腰圍≥85 cm,女性腰圍≥80 cm;糖化血紅蛋白(HbA1c)為8%~12%,排除標(biāo)準(zhǔn):(1)1型糖尿病,妊娠糖尿病,糖尿病急性并發(fā)癥。(2)嚴(yán)重肝、腎功能異常,既往有急慢性胰腺炎病史的患者。(3)有腫瘤病史。觀察組男女比例為2.34∶1;平均年齡為(48.7±1.6)歲。對照組男女比例為2.31∶1;平均年齡為(48.5±1.8)歲。兩組患者的一般情況無明顯差異(P>0.05)。
1.2 治療方法
兩組患者均每日監(jiān)測8次血糖(三餐前、三餐后2 h、睡前、凌晨3時(shí))及HbA1c,兩組均予以規(guī)范化、系統(tǒng)化糖尿病宣教,并嚴(yán)格控制飲食以及運(yùn)動(dòng)療法,基礎(chǔ)治療均為基礎(chǔ)量門冬胰島素注射液(英文名:Insulin Aspart Injecion;國藥準(zhǔn)字:J20100123;進(jìn)口藥品注冊標(biāo)準(zhǔn):JS20100088;企業(yè)名稱:Novo Nordisk A/S;生產(chǎn)地址:Novo Alle,DK-2880 Bagsvaerd,Denmark;規(guī)格:3 mL∶300單位(筆芯)持續(xù)皮下泵入,選用PH300胰島素泵。觀察組在基礎(chǔ)治療上加用艾塞那肽注射液(英文名稱:Exenatide injection;生產(chǎn)廠家:Baxter Pharmaceutical Solution LLC.;執(zhí)行標(biāo)準(zhǔn):JX20080117;進(jìn)口藥品注冊證號:5 μg(0.25 mg/mL,1.2 mL/支)的進(jìn)口藥品準(zhǔn)字號:H20130434;規(guī)格:5 μg劑量刻度注射筆:0.25 mg/mL,1.2 mL/支,單次注射藥量5 μg,內(nèi)含60次注射的藥量)5 μg/次,每日2次,對照組為在基礎(chǔ)治療上口服阿卡波糖50 mg,每日3次。兩組治療30 d為1個(gè)療程,設(shè)為觀察點(diǎn),觀察臨床癥狀改變、空腹血糖、餐后2 h血糖、血糖達(dá)標(biāo)時(shí)間、糖化血紅蛋白、胰島素用量、BMI值。
1.3 觀察指標(biāo)
使用華益精點(diǎn)血糖儀(型號ZE-808)檢測末梢指間血糖8次/d,三餐前血糖、三餐后2 h血糖、睡前血糖、凌晨3時(shí)血糖及HbA1c、胰島素用量、BMI值治療前后的變化。
1.4 評定標(biāo)準(zhǔn)
本次實(shí)驗(yàn)中正常血糖的判斷標(biāo)準(zhǔn)為:血糖控制目標(biāo)以2011年美國糖尿病協(xié)會(huì)(ADA)指南:空腹血糖控制于(3.9~7.2)mmol/L,餐后血糖控制在10 mmol/L以下[2]。低血糖的判定標(biāo)準(zhǔn)為:出現(xiàn)低血糖的癥狀,血糖測定值為<3.9 mmo1/L,依據(jù)治療后血糖波動(dòng)范圍,評估治療2型糖尿病的療效。
1.5 統(tǒng)計(jì)學(xué)方法
采用SPSS 19.0統(tǒng)計(jì)學(xué)軟件處理,計(jì)量資料采用t檢驗(yàn),計(jì)數(shù)資料組間對比采用χ2檢驗(yàn),P<0.05為差異有統(tǒng)計(jì)學(xué)意義。
2 結(jié)果
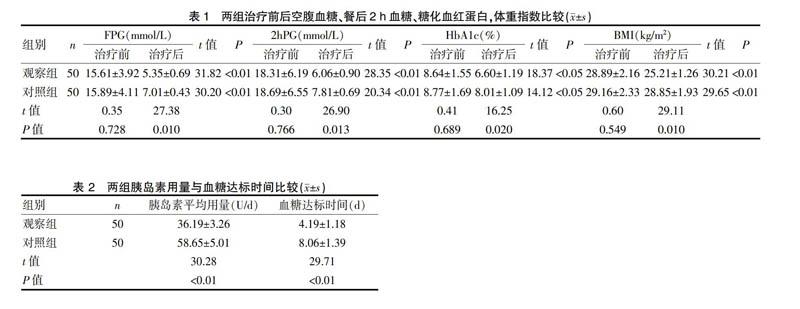
2.1 兩組治療前后空腹血糖、餐后2 h血糖、糖化血紅蛋白,體重指數(shù)比較
分析治療前后三餐血糖、HbA1c、胰島素用量、BMI的變化,結(jié)果顯示兩組治療前FPG、2 hPG及HbA1c、體重指數(shù),差異均無統(tǒng)計(jì)學(xué)意義(P>0.05),觀察組治療后血糖控制總體優(yōu)于對照組,差異有統(tǒng)計(jì)學(xué)意義(P<0.05);觀察組糖化血紅蛋白與體重指數(shù)治療后均優(yōu)于對照組,差異有統(tǒng)計(jì)學(xué)意義(P<0.05),說明艾塞那肽注射液聯(lián)合門冬胰島素注射液控制血糖的同時(shí)可以很好的控制體重。見表1。
2.2 兩組胰島素用量與血糖達(dá)標(biāo)時(shí)間比較
兩組均未發(fā)生嚴(yán)重低血糖病例,觀察組的血糖達(dá)標(biāo)時(shí)間較對照組顯著縮短,差異有高度統(tǒng)計(jì)學(xué)意義(P<0.01),觀察組的胰島素用量小于對照組,差異有高度統(tǒng)計(jì)學(xué)意義(P<0.01),提示觀察組胰島素用量低,血糖控制達(dá)標(biāo)時(shí)間短,速度快。見表2。
3 討論
糖尿病以血糖持續(xù)升高為特征,患病率逐年上升。隨著經(jīng)濟(jì)的發(fā)展及社會(huì)老齡化,糖尿病是繼心腦血管疾病、癌癥后的又一嚴(yán)重危害人民健康的慢性非傳染性疾病[3]。2型糖尿病是非胰島素依賴性糖尿病,與遺傳因素、肥胖、飲食、生活 環(huán)境、胰島素分泌障礙等因素有關(guān)[4]。同時(shí)也與胰島素拮抗激素分泌失調(diào)、胰島素抵抗、神經(jīng)內(nèi)分泌等多種因素有關(guān)。2型糖尿病的發(fā)病機(jī)制是:遺傳因素;肥胖和不健康的生活方式;原發(fā)性胰島素分泌不足及胰島素拮抗激素分泌失調(diào);胰 島素抵抗。多種因素導(dǎo)致血糖升高和胰島素的分泌量相對不足,形成惡性循環(huán)[5], 最終導(dǎo)致心血管系統(tǒng)、神經(jīng)系統(tǒng)、泌尿生殖系統(tǒng)等多個(gè)系統(tǒng)出現(xiàn)并發(fā)癥,嚴(yán)重者可導(dǎo)至死亡[6]。肥胖是2型糖尿病的獨(dú)立危險(xiǎn)因素,大多數(shù)的2型糖尿病患者伴有超重或肥胖[7]。隨著生活方式的改變,目前2型糖尿病合并肥胖的患者逐年增加,這類患者血糖控制難度較大,在口服降糖藥降糖效果不佳時(shí),會(huì)用胰島素控制血糖,同時(shí)可能使得體質(zhì)量增加,因此,2型糖尿病合并肥胖癥的血糖控制是糖尿病治療中的難題[8-10]。
艾塞那肽注射液可顯著降低血糖,并且能持續(xù)降低體重[11,12]。胰高糖素樣肽 1(glucagon-ike peptide-1,GLP-1)是小腸黏膜 L 細(xì)胞在食物刺激下釋放的激素,可促進(jìn)葡萄糖依賴的胰島素分泌[13,14]。艾塞那肽作用機(jī)制有:促進(jìn)葡萄糖依賴的胰島素分泌;抑制高血糖時(shí)胰升糖素的過度分泌;延緩胃排空;降低食欲,減少食物攝入;增加外周組織細(xì)胞,骨骼肌細(xì)胞對胰島素敏感性;降低胰島素抵抗,增加肝糖原儲存[15]。在骨骼肌和脂肪細(xì)胞中,艾塞那肽通過激活磷脂酞肌醇-3一激酶途徑增加葡萄糖攝取,改善外周組織對胰島素的敏感性,促進(jìn)胰島β細(xì)胞增生、刺激β細(xì)胞新生和抑制β細(xì)胞凋亡,從而增加胰島β細(xì)胞數(shù)量[16,17]。艾塞那肽可誘導(dǎo)胰腺導(dǎo)管上皮細(xì)胞、腺細(xì)胞和Nestin陽性導(dǎo)管細(xì)胞(潛在的多能胰島干細(xì)胞)向胰島素分泌細(xì)胞分化,也能促進(jìn)胰腺十二指腸同源框基因(pancre-aticduodenal homeobox-1,PDX-1)的表達(dá),PDX-1是胰腺內(nèi)分泌細(xì)胞功能發(fā)育的必需因子,從而促進(jìn)β細(xì)胞的新生和增殖,增加胰島素分泌[18]。肝臟有艾塞那肽的同源性受體,艾塞那肽可通過抑制磷酸肌醇依賴性激酶1、蛋白激酶C等的磷酸化,降低肝臟的脂肪變性,保持肝臟正常功能。GLP-1在進(jìn)食脂肪和碳水化合物后由空腸、回腸、結(jié)腸的L細(xì)胞分泌的一種腸降糖素,經(jīng)由內(nèi)分泌、神經(jīng) 及底物刺激等途徑作用于各種胰島細(xì)胞,是具有包括調(diào)節(jié)血糖在內(nèi)的多功能肽 類激素[19],因此,GLP-1類似物艾塞那肽在對2型糖尿病患者進(jìn)行多靶點(diǎn)的治療中就顯得至關(guān)重要。艾塞那肽和諾和銳30均可在餐后迅速釋放,但艾塞那肽可在有效控制高血糖的同時(shí)預(yù)防低血糖發(fā)生,這主要是由于艾塞那肽促胰島素分泌呈完全血糖依賴性,此為艾塞那肽的獨(dú)特優(yōu)勢[20],于此同時(shí)艾塞那肽還可抑制胰高血糖素的分泌,多方位控制血糖,同時(shí)延緩胃排空,減少食物攝入,降低體重,降低了2型糖尿病并發(fā)癥的發(fā)病危險(xiǎn)程度[21-26]。而艾塞那肽還可恢復(fù)一相和二相胰島素分泌,促進(jìn)β細(xì)胞增生,降糖的同時(shí)使用艾塞那肽治療還可以降低心血管風(fēng)險(xiǎn)因子,調(diào)節(jié)血脂、降低血壓等多方面益處[27]。已有許多體外研究顯示,GLP-1具有誘導(dǎo)β細(xì)胞增殖和分化的直接作用。對胰島細(xì)胞系 INS-1,GLP-1具有生長因子樣作用,其可以劑量依賴性地增加 DNA的合成,表達(dá)并增加 DNA的結(jié)合活性[28]。GLP-1還可以誘導(dǎo)2種胰腺導(dǎo)管細(xì)胞系分化為能合成并分泌胰島素的細(xì)胞。有研究者發(fā)現(xiàn),GLP-1可以使肥胖的高血糖大鼠出現(xiàn)胰島的生長,β 細(xì)胞的增殖[29]。研究者認(rèn)為,在調(diào)控胰島β細(xì)胞增殖的調(diào)節(jié)網(wǎng)絡(luò)中,GLP-1發(fā)出β 細(xì)胞增殖的啟動(dòng)信號,從而通過增加β 細(xì)胞數(shù)量來滿足機(jī)體對胰島素的需求。研究發(fā)現(xiàn)[30],糖尿病大鼠加用GLP-1 治療后,其β 細(xì)胞的凋亡數(shù)量顯著減少,作為凋亡標(biāo)志的凋亡小體等也顯著減少,說明GLP-1 除了具有促進(jìn)細(xì)胞增殖的作用外,抑制凋亡也是其增加胰島細(xì)胞數(shù)量的重要機(jī)制[31]。阿卡波糖是一種α葡萄糖苷酶抑制劑,研究顯示,碳水化合物在進(jìn)入胃腸道后,經(jīng)由 α 糖苷酶裂解生成一系列單糖,從而被小腸迅速吸收,并引起機(jī)體血糖水平的上升。α-葡萄糖苷酶抑制劑通過競爭性抑制作用對小腸上皮細(xì)胞中的α 葡萄糖苷酶的活性進(jìn)行抑制,減緩機(jī)體對于碳水化合物的消化和吸收,從而促進(jìn)餐后血糖水平的降低[32]。α-糖苷酶抑制劑的主要機(jī)制是在小腸上段通過可逆性地抑制腸系,膜刷狀緣的α-糖苷酶,延緩α-糖苷酶將多糖(如淀粉、寡糖等)分解為單糖(主要為葡萄糖),使葡萄糖的吸收減緩。這種抑制作用是可逆的,葡萄糖的吸收并未被阻斷而是推遲,能夠使餐后的高血糖下降,下餐前也不易出現(xiàn)低血糖,相當(dāng)于“分餐”的作用。α-糖苷酶抑制劑也能使2型糖尿病患者餐后過高的胰島素水平下降,甚至在一定程度上改善胰島素敏感性。此外,α-糖苷酶抑制劑能推進(jìn)大量未消化的碳水化合物抵達(dá)低位小腸,該部位富含產(chǎn)生胰高糖素樣肽-1(glucagon-like peptide 1,GLP-1)的L細(xì)胞,因而能夠刺激GLP-1分泌持續(xù)增加,刺激胰島素釋放,進(jìn)而降低血糖濃度。雙糖、低糖以及多糖的葡萄糖吸收,對 FBG、HbA1c具有一定程度的降低作用,而且可以較好地降低餐后血糖。阿卡波糖還具有多重獲益,可改善脂質(zhì)代謝,顯著升高高密度脂蛋白膽固醇和降低甘油三酯[33,34]。
本結(jié)果表明,觀察組的治療后血糖控制總體優(yōu)于對照組,觀察組糖化血紅蛋白與體重指數(shù)治療后均優(yōu)于對照組,兩組均未發(fā)生嚴(yán)重低血糖病例,觀察組的血糖達(dá)標(biāo)時(shí)間較對照組顯著縮短,觀察組的胰島素用量小于對照組,說明艾塞那肽注射液聯(lián)合門冬胰島素基礎(chǔ)量泵入治療可有效控制血糖達(dá)標(biāo),縮短血糖達(dá)標(biāo)時(shí)間,不使體重增加,減輕胰島素抵抗,避免了高胰島素血癥的發(fā)生,改善了血脂代謝,解除了糖毒性和脂毒性,防止了并發(fā)癥的發(fā)生和發(fā)展。
綜上所述,艾塞那肽注射液特有的葡萄糖依賴性促進(jìn)胰島素分泌可以避免低血糖的發(fā)生,綜合療效優(yōu)于阿卡波糖片聯(lián)合門冬胰島素泵入治療,是2型糖尿病合并有肥胖癥患者的較好的治療方法,值得臨床應(yīng)用及推廣。
[參考文獻(xiàn)]
[1] 高菡璐,蘭莉,喬冬菊,等. 1998~2010年哈爾濱市市區(qū)慢性病流行趨勢分析[J]. 中華疾病控制雜志,2012,16(5):396.
[2] American Diabetes Association. Standards of medical care indiabetes-2011[J]. Diabetes Care,2011,34(Suppl 1):S11-S61.
[3] Hauber A,E A Gale. Themarketin diabetes[J]. Diabetologia,2006,49(2):247-252.
[4] Corbett JA. Aminoguanidine,anovelin hibit or of nitricoxide formation,prevents diabetic vasculardys function[J]. Diabetes,1992,41(4):552-556.
[5] Lerario AC. Algorithm for the treatment of type 2 diabetes:A positionstatement of Brazilian Diabetes Society[J]. Diabetol Metab Syndr,2010,2(1):35.
[6] Elgzyri T. Basic Management of diabetes mellitus:Practicalguidelines[J]. Libyan J Med,2006,1(2):176-184.
[7] Yang W,Liu J,Weng J,et al. Prevalence of diabetes among men and women in China[J]. N Engl J Med,2010,362(12):1090-1101.
[8] Kahn SE,Haffner SM,Heise MA,et al. Glycemic durability of rosiglitazone, metformin or glyburide monotherapy[J]. N Engl J Med,2006,355(23):2427-2443.
[9] UK Prospective Diabetes Study (UKPDS) Group. Intensi-tive blood-glycemia control with sulphonylureas or insulincompared with conventional treatment and risk of complica-tions in patients with type 2 diabetes[J]. Lancet,1998,352(9131):837-853.
[10] Nathan DM,Buse JB,Davidson MB,et al. Management of hyper-glycemia in type 2 diabetes:A consensus algrithm for the initiation and adjustment of therapy. A consensus statement from the American Diabetes Association and the Europe Association for the study of diabetes[J]. Diabetes Care,2008,31(1):173-175.
[11] Davies MJ,Donneiiy R,Barnett AH,et al. Exenatide com-pared with long-acting insulin to achieve glycaemic control with minimal weight gain in patients with type 2 diabetes:results of the helping evaluate exenatide in patients with diabetes compared with long-acting insulin(HEELA)study[J]. Diabetes Obes Metab,2009,11(12):1153-1162.
[12] Sudhakaran C,F(xiàn)athima M,Anjana RM,et al. Effectiveness of exenatide in Asian Indians in a clinical care setting[J]. Diabetes Technol Ther,2010,12(8):613-618.
[13] Giugliano D,Standl E,Vilsboll T,et al. Is the current therapeutic armamentarium in diabetes enough to control the epidemic and its consequences what are the currentshortcomings[J]. Acta Diabetol,2009,46(3):173-181.
[14] Nauck MA. Unraveling the science of incretin biology[J].Eur J Intern Med,2009,20(Suppl 2):S303-S308.
[15] Knauf C,Cani PD,Perrin C,et al. Brain glucagon-like peptide-1 increases insulin secretionand insulinresistance to favor hepatic glycogenstorage[J]. J Clin Invest,2005,115(12):3554-3563.
[16] 劉敏,荊丹青,白樺,等. 艾塞那肽替代胰島素治療2型糖尿病患者的臨床分析[J]. 山西醫(yī)科大學(xué)學(xué)報(bào),2012, 43(1):47-51.
[17] Nielsen LL,Young AA,Parkes DG. Pharmacology of exenatide(synthetic exendin-4):A potential therapeutic for improved glycemic control of type 2 diabetes[J]. Regul Pept,2004,117(2):77-88.
[18] Feanny,MA Facansp,Ballian N,et al. PDX-1 expression is assoriated with islet proliferation in vitro and vi[J]. Jbiol Chem,2003,278(1):471-478.
[19] Schmidt WE,EG Siegel,W Creutzfeldt,et al. Glucagon-likepeptide-1b utnot glucagon-like peptide-2 stimulates insulinrelease fromisolatedratpancreatic islets[J]. Diabetologia,1985,28(9):704-707.
[20] Noyan-Ashraf MH. GLP-1R agonist liraglutideactivates cytoprotective pathways and improves outcomes after experimental myocardial in farction in mice[J]. Diabetes,2009, 58(4):975-983.
[21] Nauck MA. Unravelingth escience of incretin biology[J]. Am J Med,2009,122(suppl):S3-S10.
[22] Nystrom T. Effects of glucagon-like peptide-1onendo the lial function in type 2 diabetes patients with stable coronaryartery disease[J]. A m J Physiol Endocrinol Metab,2004,287(6):E1209-E1215.
[23] Webb DM,Wintle M,MaloneJ K,et al. Exenatide effects on glucose meta bolism and meta bolicdis or derscommon to over weight and obese patients with type 2 diabetes[J]. Drug Devel Res,2006,67:666-676.
[24] Nauck MA,Duran S,Kim D,et al. A comparison of twice dailyexenatide and biphasic insulin aspart in patients with type 2 diabetes who were suboptimally controlled with sulfony lrea and met formin:An oninferiority study[J].Diabetologia,2007,50:259-267.
[25] Zinman B,Hoogwerf BJ,Garcia SD,et al. The effect of adding exenatide to a thiazolidine dionein suboptimally control led type 2 diabetes[J]. Ann Intern Med,2007,146:477-485 .
[26] Mack CM,Laugero KD,Liu Q,et al. The rapeutic applic ationso fincretin mimetics for metabolic diseases:Preclinical studies[J]. Drug Dev Res,2006,67:553-558 .
[27] Blonde L,Klein EJ,Han J,et al. Interim analysis of the effect sofexenatide treatment on A1C,weight and cardiovascular risk factors over 82 weeks in 314 overweight patients with type 2 diabetes[J]. Diabetes Obes Metab,2006, 8:436-447.
[28] Stoffers DA,Kieffer TJ,Hussain MA,et al. Insulinotropic glucagon-like peptide 1 agonists stimulate expression of homeodomain protein IDX-1 and increas islet size in mouse pancreas[J]. Diabetes,2000,49(5):741-748.
[29] Vahl TP,Paty BW,F(xiàn)uller BD,et al. Effects of GLP-1-(7-36)NH2,GLP-1-(7-37),and GLP-1-(9-36)NH2,on intravenous glucose tolerance and glucose-induced Insulin secretion in healthyhumans[J]. J ClinEndocrinol Metab,2003,88(4):1772-1779.
[30] Farilla L,Bulotta A,Hirshberg B,et al. Glucagon-like peptide 1 inhibits cell apoptosis and improves glucose responsivenese of freshly isolated human islets[J]. Endocrinology,2003,144(12):5149-5158.
[31] Wang Q,Li L,Xu E,et al. Glucagon-like peptide-1 regulates proliferation and apoptosis via activation of protein kinase B in pancreatic INS-1 beta cells[J]. Diabetologia,2004,47(3):478-487.
[32] 張銀波. 阿卡波糖聯(lián)合二甲雙胍對2型糖尿病進(jìn)行治療的臨床療效觀察[J]. 中國現(xiàn)代藥物應(yīng)用,2015,9(13):145.
[33] Gao HW,Xie C,Wang HN,et al. Beneficial metabolic effects of nateglinide versus acarbose in patients with newly-diagnosed type 2 diabetes[J]. Acta Pharmacol Sin,2007,28(4):534-539.
[34] 仇維芝. 拜糖平治療2型糖尿病療效觀察[J]. 現(xiàn)代中西醫(yī)結(jié)合雜志,2013,22(26):2877-2879.
(收稿日期:2015-09-21)
猜你喜歡
中老年保健(2022年5期)2022-08-24 02:35:42
中老年保健(2022年1期)2022-08-17 06:14:56
保健醫(yī)苑(2022年6期)2022-07-08 01:26:34
家庭科學(xué)·新健康(2022年3期)2022-05-10 00:32:13
中老年保健(2021年5期)2021-08-24 07:07:20
中老年保健(2021年11期)2021-08-22 03:15:16
中國生殖健康(2019年2期)2019-08-23 08:12:10
媽媽寶寶(2017年3期)2017-02-21 01:22:30
飼料與畜牧(規(guī)模養(yǎng)豬)(2016年5期)2016-12-01 03:48:40
中國衛(wèi)生標(biāo)準(zhǔn)管理(2015年1期)2016-01-14 03:41:27