膠囊內鏡檢查中祛泡劑最佳應用時機的效果分析
2016-08-07 13:53:13王海紅史久健李愛琴余東亮盛劍秋
胃腸病學和肝病學雜志 2016年3期
王海紅, 郭 花, 史久健, 楊 浪, 王 昕, 謝 惠, 李愛琴, 余東亮, 湯 姍, 盛劍秋
1.河南省民權縣疾病預防控制中心門診部,河南 商丘 476000;2.北京軍區總醫院消化內科;3.海南省三亞市 92474 部隊醫院
膠囊內鏡檢查中祛泡劑最佳應用時機的效果分析
王海紅1, 郭 花2, 史久健3, 楊 浪2, 王 昕2, 謝 惠2, 李愛琴2, 余東亮2, 湯 姍2, 盛劍秋2
1.河南省民權縣疾病預防控制中心門診部,河南 商丘 476000;2.北京軍區總醫院消化內科;3.海南省三亞市 92474 部隊醫院
目的 重點觀察祛泡劑在膠囊內鏡檢查中最佳應用時機選擇后的應用效果。方法 300例在北京軍區總醫院消化內鏡中心接受膠囊內鏡檢查的患者,隨機分成3組:A組(100例):口服膠囊內鏡前45 min時服用祛泡劑30 ml;B組(100例):口服膠囊內鏡前30 min時服用祛泡劑30 ml;C組(100例):口服膠囊內鏡前15 min服用祛泡劑30 ml。比較3組患者胃、小腸及結腸內的氣泡量、圖像清晰度、腸道清潔滿意度和閱片醫師滿意度,并觀察有無不良反應。結果 3組患者均無不良反應發生,A組胃腔、小腸腸道和結腸腸道內氣泡量少,影像清晰度好,閱片醫師滿意度最好,其膠囊內鏡圖像清晰度、腸道清潔程度和病變發現率優于B組和C組,差異有統計學意義(P<0.01)。結論 膠囊內鏡檢查前45 min服用祛泡劑可以充分祛除胃、小腸和結腸內的氣泡和黏液,明顯提高膠囊內鏡檢查的影像清晰度、腸道清潔程度和病變發現率,閱片醫師滿意度好。
膠囊內鏡;祛泡劑;氣泡;清晰度;滿意度
膠囊內鏡(capsule endoscopy, CE)檢查越來越廣泛地應用到臨床中,在無癥狀人群中應用也越來越廣泛,為小腸疾病的檢查提供了新途徑,其可對全胃腸道進行簡便、快速、無創、連續地觀測性檢查[1]。膠囊內鏡雖有優點,但與普通胃鏡、腸鏡相比,不能自由充氣、注水,不能人為控制觀察角度及采集圖像。腸道清潔程度是影響膠囊內鏡影像質量的關鍵[2]。若消化道內存在大量泡沫,直接降低膠囊內鏡視野攝像清晰度,影響閱片醫師直接觀察,造成誤診、漏診[3]。因此,檢查前做好充分的腸道準備可以提高膠囊內鏡圖像質量,對于提高膠囊內鏡病變檢出率極其重要。我國膠囊內鏡檢查前腸道準備主要是根據結腸鏡檢查前腸道準備方法改進,很多研究表明聯合應用聚乙二醇電解質散劑和祛泡劑清潔腸道效果優于單用其中任何一種[4]。為進一步探討膠囊內鏡檢查前祛泡劑的最佳應用時機,本研究對北京軍區總醫院消化內鏡中心300例接受膠囊內鏡檢查者,按照膠囊內鏡檢查前腸道準備聯合應用祛泡劑不同時機進行了隨機對照研究。
1 資料與方法
1.1 一般資料 收集2013年2月-2015年3月在北京軍區總醫院消化內鏡中心進行膠囊內鏡檢查的300例符合入選標準的檢查者。其中男 196 例,女 104 例,年齡19~65歲,平均(47.58±15.6)歲。入選標準:(1)不明原因消化道出血,即反復發作的血便或黑便或糞便潛血持續陽性,經上、下消化道內鏡檢查均無陽性發現者;(2)不明原因慢性腹痛及腹瀉患者;(3)臨床懷疑小腸炎癥性腸病,但無腸梗阻及腸狹窄者;無癥狀體檢者。隨機分為3組,A組(100例):膠囊內鏡檢查前45 min時服用祛泡劑;B組(100例):膠囊內鏡檢查前30 min時服用祛泡劑;C組(100例):膠囊內鏡檢查前15 min服用祛泡劑。3組檢查者在性別、年齡、身高、體質量差異無統計學意義(P>0.05),具有可比性。
1.2 儀器與藥品 300例患者均采用重慶金山公司生產的OMOM (JS-ME-Ⅲ型)膠囊內鏡及配套的圖像記錄儀和影像工作站。電池工作時間8~12 h。檢查前患者禁食8 h,禁水6 h,于檢查當日早晨6時口服聚乙二醇電解質散劑2 000 ml(舒泰神,北京生物制藥股份有限公司),服用后按不同時段口服祛泡劑30 ml(西甲硅油乳劑 Glienicker Weg 125 D-12489 Berlin,商品名:柏西,德國柏林化學股份有限公司,規格:40 mg/ml×30 ml/瓶)。
1.3 方法 所有進行膠囊內鏡檢查者均簽署檢查知情同意書,A組膠囊內鏡檢查前45 min口服西甲硅油乳劑30 ml; B組膠囊內鏡檢查前30 min口服西甲硅油乳劑30 ml;C組膠囊內鏡檢查前15 min口服西甲硅油乳劑30 ml,3組均未再服用其他任何促胃動力等相關藥物。檢查開始后2 h內禁食、水,2 h后可飲少量清水,4 h后可進全流質飲食,檢查結束后恢復正常飲食。檢查期間受檢者可自由活動,避免接近磁場或電動車充電器之類的場所。
1.4 觀察指標 根據康艷等[5]文獻標準,對胃、小腸內的氣泡量及其對胃、小腸黏膜觀察的影響程度分為3個等級, 優:腸腔內無氣泡及黏液,能清晰地觀察到腸壁及腸腔情況;良:腸腔內少量氣泡及黏液,基本能觀察到腸壁及腸腔情況;差:腸腔內較多甚至大量氣泡及黏液,基本看不清腸壁及腸腔情況。根據內鏡醫師閱讀時的滿意度分為3個等級。Ⅰ級(非常滿意):胃及小腸和結腸腸腔無氣泡及黏液附著,清晰度好,觀察病變滿意;Ⅱ級(一般):胃及小腸和結腸腸腔內少量氣泡和黏液,清晰度尚可,尚不嚴重影響觀察病變;Ⅲ級(不滿意):胃及小腸和結腸腸腔內較多氣泡和黏液附著,清晰度差,影響觀察病變。
1.5 統計學處理 采用SPSS 13. 0軟件進行統計分析,組間資料進行χ2檢驗,P<0.01為差異有顯著統計學意義。
2 結果
所有患者均順利完成檢查且觀測到部分結腸,均未出現不良反應。由專職內鏡醫師單盲進行閱片。A組胃、小腸和結腸內氣泡量及黏液最少,黏膜清晰度最高,閱片滿意度最好,分別與B組和C組比較,差異均有統計學意義(P<0.01,見表1~2,圖1)。A組的病變發現率,尤其是小腸病變發現率明顯高于B組和C組,差異有統計學意義(P<0.01,見表3)。
表1 各組胃、小腸、結腸內清潔度的比較[例數 (%)]
Tab 1 Comparison of stomach, small intestine and colon cleanliness in three groups [n(%)]

組別例數優良差優良率(%)A組100935298.00B組10096815.00C組10043937.00
表2 3組內鏡醫師閱片滿意度的比較 [例數(%)]
Tab 2 Comparison of endoscopist satisfaction in three groups [n(%)]
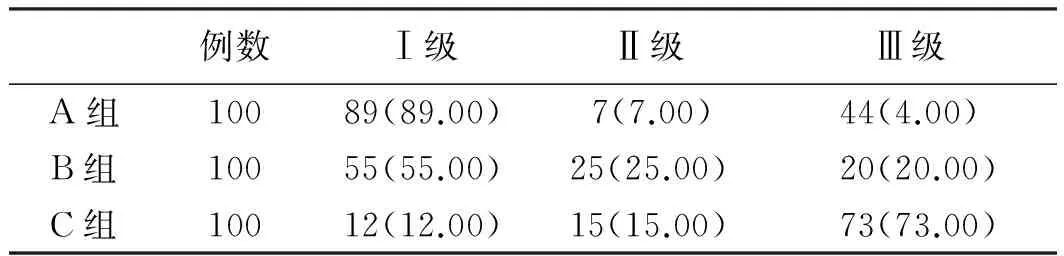
例數Ⅰ級Ⅱ級Ⅲ級A組10089(89.00)7(7.00)44(4.00)B組10055(55.00)25(25.00)20(20.00)C組10012(12.00)15(15.00)73(73.00)
表3 內鏡醫師閱片病變檢出率*[例數(%)]
Tab 3 Lesion detection rate of endoscopists read the piece[n(%)]

組別例數胃小腸結腸A組10072(72.00)88(88.00)32(32.00)B組10013(13.00)7(7.00)5(5.00)C組1006(6.00)4(4.00)3(3.00)
注:*指總共發現的消化道病變例數,即每例檢查者可能發現超過1次以上病變。
3 討論
膠囊內鏡自問世10余年來,已經成為小腸檢查的重要手段之一,但其局限性也很明顯,定位、定性比較困難,還有眾多的因素可能影響膠囊內鏡的圖像質量,如:內鏡拍攝角度、腸蠕動、腸內氣泡數及黏液附著、腸液量及清潔度等[4]。因此,良好的腸道準備對膠囊內鏡檢查非常重要。祛泡劑用于上消化道內鏡檢查和膠囊內鏡檢查,可提高檢查圖像的清晰度,利于閱片醫師提高病變的發現率[6],但是如何選擇祛泡劑口服的最佳時機,以發揮更好的祛泡效果是關鍵問題,本組研究表明,在膠囊內鏡檢查時提前30 min口服祛泡劑腸道氣泡,清潔度好,閱片醫師滿意,但是提前45 min口服西甲硅油乳劑30 ml,則更能充分有效地祛除胃、小腸腸道內的氣泡,提高檢查圖像的清晰度,內鏡醫師閱片滿意度好,病變檢出率明顯優于檢查前30 min和檢查前15 min口服西甲硅油乳劑,與國外研究[7-8]發現加服祛泡劑的試驗組較對照組受腸腔內氣泡的影響少,圖像質量均顯著優于對照組。與中國膠囊內鏡臨床應用指南中進行膠囊內鏡檢查30 min口服祛泡劑效果好也相符合[9-10],由此可見,在進行膠囊內鏡檢查時,為了使腸道內氣泡量及黏液減少并獲得更清晰的圖像,在標準腸道清腸后,吞服膠囊內鏡前45 min口服祛泡劑應該是進行該檢查的最佳時機,從而達到內鏡醫師閱片滿意和提高病變的檢出率,值得臨床上推廣和應用。

圖1 3組不同時間口服西甲硅油乳劑檢查后胃、小腸、結腸的膠囊內鏡病例圖 A組:吞服膠囊內鏡前45 min口服西甲硅油乳劑30 ml;B組:吞服膠囊內鏡前30 min口服西甲硅油乳劑30 ml;C組:吞服膠囊內鏡前15 min口服西甲硅油乳劑30 ml
Fig 1 Colon capsule endoscopy results of stomach, small intestine after oral simethicone emulsion in 3 different time A: simethicone emulsion was taken 30 ml before 45 minutes oral capsule endoscopy; B: simethicone emulsion was taken 30 ml before 30 minutes oral capsule endoscopy; C: simethicone emulsion was taken 30 ml before 15 minutes oral capsule endoscopy
[1]Zhang ZQ, Chen X, Wu BY, et al. Clinical applications of capsule endoscopy [M]. Beijing: People’s Medical Publishing House, 2006. 張子其, 陳孝, 吳本儼, 等. 膠囊內鏡臨床應用[M]. 北京: 人民軍醫出版社, 2006.
[2]Chen X, Zhang ZQ, Zhang Y, et al. The effects of intestinal content on capsule endoscopy image [J]. Sichuan Medical Journal, 2009, 30(6): 788-790. 陳孝, 張子其, 張鈺, 等. 腸內容物特性對膠囊內鏡圖像質量的影響[J]. 四川醫學, 2009, 30(6): 788-790.
[3]Kong JY, Bao XQ, Tang P, et al. Application and study of Simethicone and PEG-electrolyte powder in preparation of bowel for colonoscopy [J]. Chin J Gastroenterol Hepatol, 2010, 19 (4): 372-373. 孔金艷,鮑小倩,唐平, 等. 西甲硅油乳劑在結腸鏡檢查中的應用與研究[J]. 胃腸病學和肝病學雜志, 2010, 19(4): 372-373.
[4]Guo GH, Yin SX, Tang LW, et al. The clinical study of capsule endoscopy images of different bowel preparation [J]. Hebei Medical Journal, 2009, 31(9): 1509-1560. 郭桂華,尹淑新,唐立偉,等. 不同腸道準備方法對膠囊內鏡檢查圖像的臨床研究[J]. 河北醫學, 2009, 31(9): 1509-1560.
[5]Kang Y, Chen X, Liu BY. Preliminary study on bowel preparation for capsule endoscopy [J]. Chin J Dig Endosc, 2006, 23(4): 307-309. 康艷, 陳星, 劉變英. 膠囊內鏡腸道準備初探[J]. 中華消化內鏡雜志, 2006, 23(4): 307-309.
[6]Wang ZQ, Wang X, Deng MM, et al. Application of simethicone in the preparations before colonscopy examination [J]. Sichuan Medical Journal, 2010, 31(6): 867-869. 王忠瓊, 王烜, 鄧明明, 等. 西甲硅油乳劑在結腸鏡檢查準備中的應用[J]. 四川醫學, 2010, 31(60): 867-869.
[7]Valiante F, Bellumat A, De Bona M, et al. Bisacodyl plus split 2-Lpolyethylene glycol-citrate-simethicone improves quality of bowel preparation before screening colonoscopy [J]. World J Gastroenterol, 2013, 19(33): 5493-5499.
[8]De Leone A, Tamayo D, Fiori G, et al. Same-day 2-L PEG-citratesimethicone plus bisacodyl vs split 4-L PEG:bowel cleansing for late-morning colonoscopy [J]. World J Gastrointest Endosc, 2013, 5(9): 433-439.
[9]Ge ZZ, Chen HY, Gao YJ, et al. Study of the best candidates for capsule endoscopy for obscure gastrointestinal bleeding [J]. J Diagn Concepts Pract, 2008, 7(1): 26-29. 戈之錚, 陳海英, 高云杰, 等. 膠囊內鏡對不明原因消化道出血最佳檢查時機的研究[J]. 診斷學理論與實踐, 2008, 7(1): 26-29.
[10]Tang BD, Li M, Liu SC, et al. Clinical application of simethicone in the prepatations before colonoscopy examinations [J]. Journal of Tropical Medicine, 2007, 7(10): 985-986, 982. 唐保東, 李媚, 劉思純, 等. 西甲硅油乳劑在膠囊內鏡檢查前準備中的臨床應用[J]. 熱帶醫學雜志, 2007, 7(10): 985-986, 982.
(責任編輯:李 健)
Effect of the best application time of the simethicone emulsion in the capsule endoscopy
WANG Haihong1, GUO Hua2, SHI Jiujian3, YANG Lang2, WANG Xin2, XIE Hui2, LI Aiqin2, YU Dongliang2, TANG Shan2, SHENG Jianqiu2
1.Clinic in Minquan County Center for Disease Control and Prevention, Shangqiu 476000; 2.Department of Gastroenterology, the Military General Hospital of Beijing PLA; 3.92474 Military Hospital of PLA, China
Objective To observe the application effect of the best application time of the simethicone emulsion in the capsule endoscopy. Methods Three hundred patients underwent capsule endoscopy examination in the Military General Hospital of Beijing PLA were randomly divided into 3 groups: group A: simethicone emulsion (30 ml) was taken 45 minutes before capsule endoscopy examination; group B: simethicone emulsion was taken 30 minutes before capsule endoscopy examination; group C: simethicone emulsion was taken 15 minutes before capsule endoscopy examination. Bubble volume and image clarity in stomach, small intestine and colon, intestinal cleaning and reading doctorsatisfaction, as well as the adverse reactions were compared among 3 groups. Results No adverse reactions occurred in the 3 groups, group A had the least bubble and the most clear image in stomach, small intestine and colon, and intestinal cleaning and reading doctor satisfaction. The lesion detection rate of group A was higher than that of other two groups. The difference was statistically significant (P<0.01). Conclusion In order to fully remove air bubbles and mucous adhesion in the stomach, small intestine and colon, and to improve image clarity, intestinal cleaning and reading doctor satisfaction, it’s better to take simethicone emulsion 45 minutes before capsule endoscopy examination.
Capsule endoscopy; Simethicone emulsion; Air bubbles; Clarity; Satisfaction
10.3969/j.issn.1006-5709.2016.03.020
王海紅,主治醫師,碩士,研究方向:消化內鏡、早癌診斷及內鏡下治療。E-mail: 38763481@qq.com
盛劍秋,教授,主任醫師,博士生導師,研究方向:消化系統疾病及內鏡下診斷和治療。E-mail: Jianqiu@263.com
R57
A
1006-5709(2016)03-0308-03
2015-05-11
