
縮短肝癌篩查間隔對乙型肝炎肝硬化相關肝細胞癌患者預后的影響
2017-08-07 10:05:38丁惠國張世斌張月寧王貞彪吳燕京于海濱
臨床肝膽病雜志 2017年7期
關鍵詞:肝癌
李 鵬, 丁惠國, 徐 輝, 張世斌, 張月寧, 王貞彪, 吳燕京, 于海濱
(首都醫科大學附屬北京佑安醫院 消化中心, 北京 100069)
縮短肝癌篩查間隔對乙型肝炎肝硬化相關肝細胞癌患者預后的影響
李 鵬, 丁惠國, 徐 輝, 張世斌, 張月寧, 王貞彪, 吳燕京, 于海濱
(首都醫科大學附屬北京佑安醫院 消化中心, 北京 100069)
目的 探討縮短肝癌篩查間隔對乙型肝炎肝硬化患者早期肝細胞癌(HCC)檢出情況及預后的影響,探索針對這一HCC高危人群的適宜篩查方案。方法 收集2007年1月-2008年1月北京佑安醫院消化中心診治的乙型肝炎肝硬化患者310例, 按其篩查時間分為間隔3個月篩查組(A組)78例和間隔6個月篩查組(B組)232例。篩查項目為血清AFP及B超, 隨訪5年,對期間檢出的HCC患者繼續隨訪至終點(死亡或2016年12月31日)。比較2組患者HCC的檢出情況和預后。2組間計量資料比較采用t檢驗,計數資料比較采用χ2檢驗或Fisher檢驗;生存分析采用Kaplan-Meier法。結果 310例患者至隨訪5年結束累積檢出HCC 73例,A組21例,B組52例;A組中巴塞羅那肝癌分期中屬于早期(A期)者占66.7%(14/21),顯著高于B組的15.4%(8/52)(χ2=18.685,P<0.001)。A組行根治性治療的患者比例顯著高于B組(76.2%vs 36.5%,χ2=9.424,P=0.002)。對檢出的HCC癌患者繼續隨訪至終點時,患者累積生存時間:A組為(66.4±8.0)個月,顯著高于B組(38.1±4.5)個月(t=4.295,P=0.038);累積生存率:A組為71.4%(15/21),B組為46.2%(24/52),A組顯著高于B組(χ2=3.840,P=0.043)。 結論 針對乙型肝炎肝硬化患者, 間隔3個月進行篩查可提高HCC早期檢出率,使其獲得更多可根治性治療的機會, 延長生存時間。
肝炎病毒,乙型; 肝硬化; 癌, 肝細胞; 早期診斷; 預后
據文獻[1-2]報道,自臨床確診后,肝細胞癌(HCC)患者5年生存率僅為6%~9%,而早期診斷為HCC患者的5 年生存率則高達50%~75%,因此, 國內外指南[3]均強調HCC的早期篩查和監測是延長患者生存期的有效手段。目前國內的常規篩查方案與亞太地區指南推薦方案一致,即6個月檢查一次肝臟B超及AFP[4]。但是針對乙型肝炎肝硬化這個HCC高危人群,經常發現患者即使按這個方案隨訪,發現腫瘤時也已經不是早期,失去了根治性治療機會。有文獻[5]報道,HCC從檢測不到發展到直徑為2 cm約需3~12個月。因此有學者認為可根據腫瘤的生長速度或腫瘤倍增時間確定監測的理想時間間隔[6]。通過前期研究[7]發現,縮短篩查間隔能更早發現HCC,使患者獲得更多根治性治療機會。但能否延長患者生存時間,使患者獲益尚不明確。因此,本研究擴大隨訪病例數,延長隨訪時間,以進一步探究乙型肝炎肝硬化人群的適宜篩查方案。
1 資料和方法
1.1 研究對象 收集2007年1月-2008年1月本院消化中心治療的乙型肝炎肝硬化患者,診斷均符合《慢性乙型肝炎防治指南(2010年版)》[8]。排除標準:(1)篩選時或隨訪期間合并或重疊感染其他嗜肝病毒;(2)篩選時存在心、肺、腦、腎及神經系統疾病;(3)篩選時存在其他惡性腫瘤;(4)妊娠及哺乳期女性。HCC的診斷依據衛生部頒布的《原發性肝癌診療規范(2011年版)》[9]和2010年美國肝病學會肝癌診治指南[6]。HCC分期依據巴塞羅那(BCLC)分期標準[10]。
1.2 研究方法
1.2.1 篩查方案 對所有患者按不同篩查間隔時間分為A組: 間隔3個月;B組: 間隔6個月。自入組時開始進行血清AFP及肝臟B超篩查。 所有患者隨訪5年,對于隨訪期間發現HCC的患者繼續隨訪至2016年12月31日或至患者死亡。 AFP≥20 μg/L和(或)B超發現肝內結節定義為篩查陽性。基線及篩查隨訪期內全部陽性病例均經CT、MRI或病理檢查進一步確診,排除的患者繼續按原有方案隨訪,至下一隨訪時間,如B超顯示結節最大直徑≥1 cm或增大≥原結節最大直徑的50%或數目增多≥1個,進一步行CT、MRI或病理檢查,如沒有變化或變化未達上述標準,繼續按原方案隨訪,直至隨訪結束。
1.2.2 檢測指標及方法 (1)血清學:空腹采集外周血檢測如下指標。AFP檢測:采用全自動電化學發光免疫分析系統進行測定(Cobas e601,羅氏公司,德國)。HBV血清學標志物檢測:電化學發光法測定(170電化學發光儀,羅氏公司,德國);肝臟生化及凝血指標測定:ALT、AST、TBil、Alb測定采用全自動生化分析儀(AU5400,奧林巴斯公司,日本);PT測定采用比濁法。(2)影像學:進行B超、CT、MRI檢查。(3)病理組織學和(或)細胞學:檢查均由2名以上病理學科專家診斷確證。

2 結果
2.1 一般資料 本次納入隨訪患者共310例,其中A組78例,B組232例。2組患者在人口特征及臨床特點方面差異均無統計學意義(P值均>0.05)(表1)。
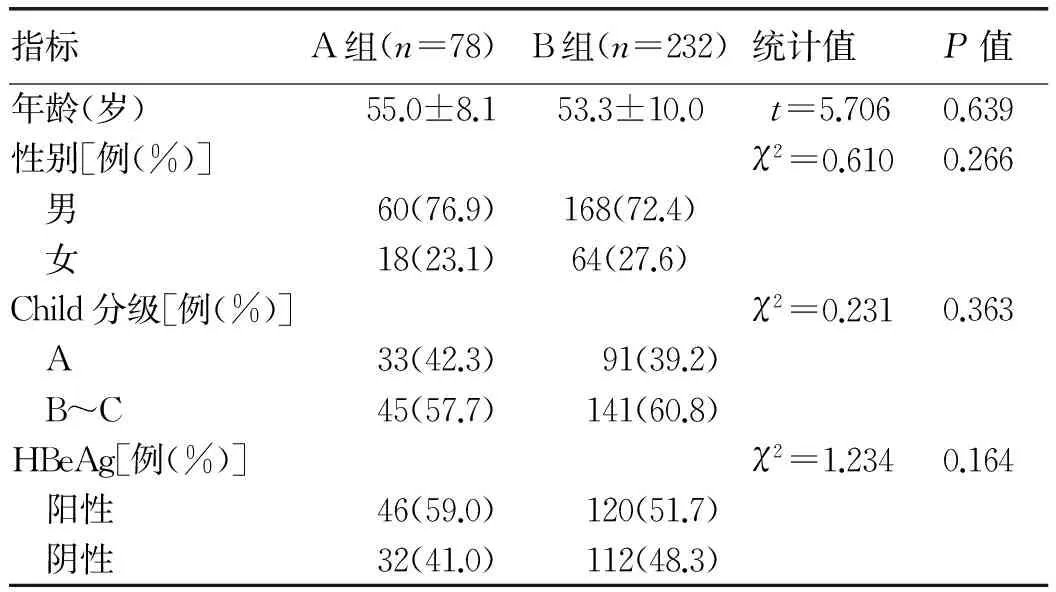
表1 2組患者的基線資料及臨床相關指標比較
2.2 HCC篩查結果 基線至隨訪6個月,2組均未發現HCC。至隨訪5年結束共確診HCC 73例,17例病理診斷,56例CT和MRI診斷。
2.3 HCC患者的腫瘤特點和治療狀況 73例HCC患者中,A組21例,B組52例。A組早中期HCC的比例為66.7%(14/21),B組為15.4%(8/52), 2組比較差異有統計學意義(χ2=18.685,P<0.001)。A組中2例行肝移植,5例手術切除,9例行射頻消融治療;B組中3例手術切除治療,16例行射頻消融治療。A組行根治性治療的患者比例顯著高于B組(76.2%vs 36.5%,χ2=9.424,P=0.002)(表2)。
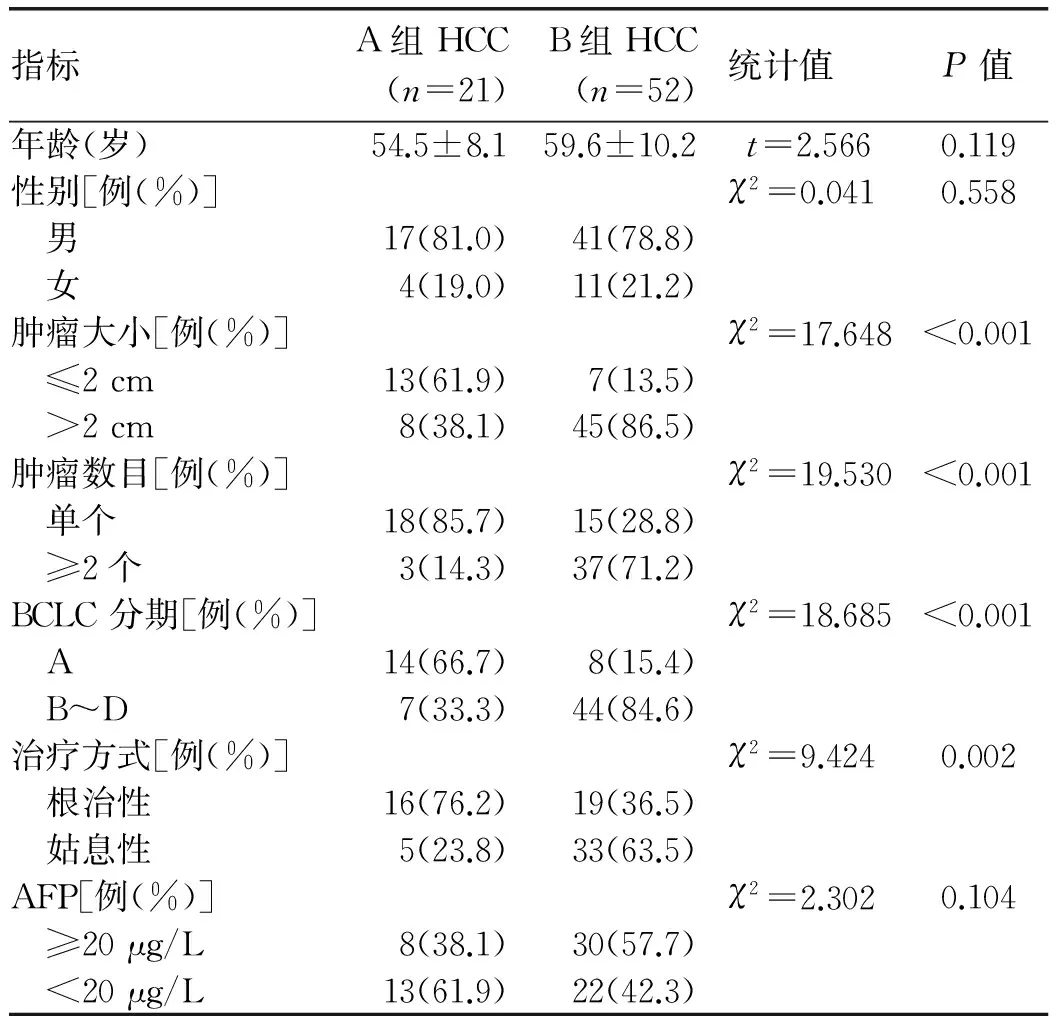
表2 2組發生HCC患者的人口學資料和臨床指標比較
2.4 HCC患者的生存情況比較 2組HCC患者累積生存時間比較,A組顯著高于B組,差異有統計學意義[(66.4±8.0)個月vs(38.1±4.5)個月,t=4.295,P=0.038)。隨訪結束累積生存率A組為71.4%(15/21),B組為46.2%(24/52),2組比較差異有統計學意義 (χ2=3.840,P=0.043)(圖1)。
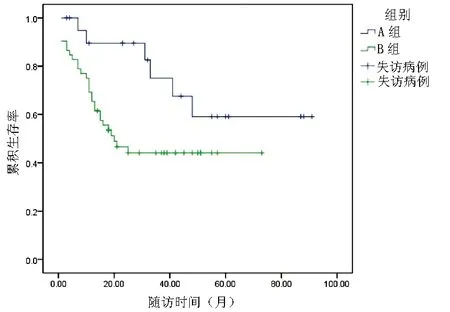
圖1 2組HCC患者累積生存率比較
3 討論
HCC的根治性治療包括肝移植、腫瘤手術切除、射頻消融治療,但根治性治療有賴于腫瘤的早期發現。文獻[11-14]證實BCLC A期HCC可以從根治性治療中獲益,有望延長患者生存期。因此,有效的篩查方案尤為重要。
通常影響篩查方案質量的因素包括兩個:篩查的項目和篩查的頻率。HCC的篩查項目包括影像學和血清學標志物。影像學中肝臟超聲檢查是全球公認的篩查工具,雖然CT和MRI對HCC的診斷優勢顯著高于超聲,但受限于價格昂貴和高技術含量等因素,很難用于人群的腫瘤篩查。對于血清學標志物,目前世界上不同地區有不同建議,美國和歐洲肝病學會的指南[6,15]均未推薦血清學標志物,主要認為目前的血清學標志物敏感度和特異度低,對于HCC的早期篩查沒有幫助。而亞太地區包括我國在內仍將AFP作為重要的血清學標志物,文獻[16]報道AFP的敏感性和特異性在60%~70%左右。這可能和亞太地區的HCC患者以HBV感染為主, 而HBV感染相關HCC患者AFP的陽性率高有關。但仍有近1/3的HCC患者AFP陰性,故近年探索新的血清學標志物一直是臨床研究的熱點[17-18]。有研究[19]顯示,異常凝血酶原的敏感度和特異度均高于AFP,被日本肝病學會指南[20]推薦用于與AFP進行聯合篩查。但有文獻[18]指出,日本以丙型肝炎患者居多,丙型肝炎所致的HCC其異常凝血酶原水平較AFP陽性率有增高的趨勢,這表明異常凝血酶原對丙型肝炎所引起的腫瘤有特異性,我國的HCC以乙型肝炎所致為主,篩查效果如何,尚需進一步研究。因此,目前通過改進篩查項目提高HCC篩查效率的研究進展不多。
另一方面,對于篩查的頻率,目前全球各大指南的篩查方案基本均是針對所有人群,并沒有針對發生HCC的不同風險人群而采取不同方案。乙型肝炎肝硬化患者被公認為HCC的高危人群,每6個月篩查一次,臨床工作中經常遇到雖然篩查到腫瘤,但往往已不是早期,失去可根治性治療的機會。能否通過改變篩查頻率達到提高篩查效率的目的?目前只有日本肝病學會的指南[20]提出針對肝硬化這一高危人群應縮短篩查間隔的建議。筆者之前的研究工作也證實,針對乙型肝炎肝硬化人群縮短篩查間隔有利于發現更多BCLC A期肝癌,為其贏得了更多根治性治療機會。本次在前期研究[7]基礎上擴大隨訪人群,延長隨訪時間,研究發現間隔3個月篩查一次篩查出早期HCC的比例顯著高于間隔6個月的患者,有更多比例的人群得到根治性治療(76.2%vs 36.5%),進一步印證了前期研究結果。對所有篩查出的HCC患者進行隨訪,間隔3個月篩查一次的患者平均生存時間顯著高于間隔6個月的患者。
因此,筆者認為對于乙型肝炎肝硬化這一HCC的高危人群, 縮短篩查間隔為3個月,可以提高早期HCC的檢出率,使更多患者獲得根治性治療機會,顯著延長患者生存時間。更重要的是,此建議并沒有增加不易推廣的新的檢測項目,也沒有明顯加重患者的經濟負擔,易于廣大基層醫院推廣實施,使更多患者從中獲益。本研究選取醫院一定時間范圍內就診患者為隨訪對象,病例數有限,研究結果可能存在一定偏倚。今后希望通過進行多中心大樣本的臨床研究,進一步證實研究結論。
[1] QI JH, WANG J, KATAYAMA H, et al.Circulating microRNAs ( cmiRNAs) as novel potential biomarkers for hepatocellular carcinoma[J].Neoplasma, 2013, 60(2): 135-142.[2] VILANA R, FORNER A, GARCIA AN, et al.Hepatocellular carcinoma: diagnosis, staging, and treatment strategy[J].Radiologia, 2010, 52(5): 385-398.
[3] KUDO M. The 2008 Okuda lecture: management of hepatocellular carcinoma: from surveillance to molecular targeted therapy[J]. J Gastroenterol Hepatol, 2010, 25(3): 439- 452.
[4] OMATA M, LESMANA LA, TATEISHI R, et al.Asian Pacific Association for the study of the liver consensus recommendations on hepatocellular carcinoma[J].Hepatol Int, 2010, 4(2): 439-474.
[5] BRUIX J, SHERMAN M, LLOVET JM, et al.Clinical management of hepatocellular carcinoma. Conclusion of the Barcelona-2000 EASL Conference[J]. J Hepatol, 2001, 35(3): 421-430.
[6] BRUIX J, SHERMAN M. Management of hepatocellular carcinoma-an update[J]. Hepatology , 2011, 53(3): 1020-1022.[7] LI P, CHEN YH, ZHANG SB, et al.Comparison of dierent hepatocarcinoma screening schemes for patients with hepatitis B associated cirrhosis: Detection rate and impact on prognosis[J].World Chin J Dig, 2015, 20(23): 3298-3303. (in Chinese) 李鵬, 陳玉涵, 張世斌, 等. 乙型肝炎肝硬化患者不同肝癌篩查方案的比較及對預后影響[J]. 世界華人消化雜志, 2015, 20(23): 3298-3303.
[8] Chinese Society of Hepatology and Chinese Society of Infectious Diseases, Chinese Medical Association. The guideline of prevention and treatment for chronic hepatitis B (2010 version)[J]. J Clin Hepatol, 2011, 27(1): I-XVI. (in Chinese) 中華醫學會肝病學分會, 中華醫學會感染病學分會. 慢性乙型肝炎防治指南(2010年版)[J]. 臨床肝膽病雜志, 2011, 27(1): I-XVI.
[9] Ministry of Health of the People′s Republic of China. Diagnosis, management, and treatment of hepatocellular carcinoma[J]. J Clin Hepatol, 2011, 27(11): 1141-1159. (in Chinese) 中華人民共和國衛生部, 原發性肝癌診療規則(2011年版)[J]. 臨床肝膽病雜志, 2011, 27(11): 1141-1159.
[10] FORNER A, REIG ME, de lOPE CR, et al. Current strategy for staging and treatment: the BCLC update and future prospects[J]. Semin Liver Dis, 2010, 30(1): 61-74.
[11] LIN SM, LIN CJ, LIN CC, et al. Randomised controlled trial comparing percutaneous radiofrequency thermal ablation, percutaneous ethanol injection, and percutaneous acetic acid injection to treat hepatocellular carcinoma of 3cm or less[J]. Gut, 2005, 54(8): 1151-1156.
[12] WANG JH, CHANGCHIEN CS, HU TH, et al. The efficacy of treatment schedules according to Barcelona Clinic Liver Cancer staging for hepatocellular carcinoma-survival analysis of 3892 patients[J].Eur J Cancer, 2008, 44(7): 1000-1006.
[13] TSENG PL, WANG JH, TUNG HD, et al. Optimal treatment increased survival of hepatocellular carcinoma patients detected with community-based screening[J].J Gastroenterol Hepatol, 2010, 25(8): 1426-1434.
[14] KUO YH, LU SN, CHEN CL, et al. Hepatocellular carcinoma surveillance and appropriate treatment options improve survival for patients with liver cirrhosis[J].Eur J Cancer, 2010, 46(4): 744-751.
[15] LLOVET JM, DUCREUX M, LENCIONI R. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma[J].J Hepatol, 2012, 56(4): 908-943.
[16] STEFANIUK P, CIANCIARA J, WIERCINSKA-DRAPALO A. Present and future possibilities for early diagnosis of hepatocellular carcinoma[J]. World J Gastroenterol, 2010, 16(4): 418-424.
[17] LIN H, ZHENG WD. The diagnosis and prognostic value of AFP, AFU, TSGF and IL-8 in liver transplantation patients with liver cancer[J]. J Clin Exp Med, 2017, 16(8): 776-780. (in Chinese) 林花, 鄭衛東. AFP、AFU、TSGF及IL-8對肝癌患者診斷及肝移植術預后評估的價值研究[J]. 臨床和實驗醫學雜志, 2017, 16(8): 776-780.
[18] ZHU QX. Diagnostic value of joint detection of golgin 73, alpha-fetoprotein, alpha-fetoprotein variants for primary hepatocellular carcinoma[J]. China Med Herald, 2016, 13(5): 130-133. (in Chinese) 諸琴紅. 高爾基體蛋白73、甲胎蛋白、甲胎蛋白異質體3%聯合檢測對原發性肝癌的診斷價值[J]. 中國醫藥導報, 2016, 13(5): 130-133.
[19] LI JL, SHAGN J, NING HB, et al. Role of serum abnormal prothrombin protein induced by vitamin K absence or antagonist-II in development and progression of hepatocellular carcinoma[J].J Clin Hepatol, 2017, 33(1): 171-174. (in Chinese) 李俊利, 尚佳, 寧會彬, 等.PIVKA-II在肝細胞癌診斷及預后判斷中的作用[J].臨床肝膽病雜志, 2017, 33(1): 171-174.[20] KOKUDO N, HASEGAWA K, AKAHANE M,et al.Evidence-based clinical practice guidelines for hepatocellular carcinoma: the Japan Society of Hepatology 2013 update (3rd JSH-HCC Guidelines)[J]. Hepatol Res, 2015, 45(2): 123-127. 引證本文:LI P, DING HG, XU H, et al. Shortening liver cancer screening interval may improve the prognosis of patients with hepatitis B cirrhosis-related hepatocellular carcinoma[J]. J Clin Hepatol, 2017, 33(7): 1301-1304. (in Chinese) 李鵬, 丁惠國, 徐輝, 等. 縮短肝癌篩查間隔對乙型肝炎肝硬化相關肝細胞癌患者預后的影響[J]. 臨床肝膽病雜志, 2017, 33(7): 1301-1304.
(本文編輯:劉曉紅)
Shortening liver cancer screening interval may improve the prognosis of patients with hepatitis B cirrhosis-related hepatocellular carcinoma
LIPeng,DINGHuiguo,XUHui,etal.
(DepartmentofGastroenterologyandHepatology,BeijingYouAnHospital,CapitalMedicalUniversity,Beijing100069,China)
Objective To investigate the influence of shortening liver cancer screening interval on the detection of early-stage hepatocellular carcinoma (HCC) in patients with hepatitis B cirrhosis and their prognosis, as well as proper screening schemes for such patients at a high risk of HCC. Methods A total of 310 patients with hepatitis B cirrhosis who were diagnosed and treated in Department of Gastroenterology and Hepatology, Beijing YouAn Hospital, from January 2007 to January 2008 were enrolled, and according to the screening interval, they were divided into 3-month screening group (group A) with 78 patients and 6-month screening group (group B) with 232 patients. The screening items included serum alpha-fetoprotein and ultrasound and the patients were followed up for 5 years. The patients with HCC screened out were followed up to the endpoint (death or December 31, 2016). The detection of HCC and prognosis were compared between the two groups. Thet-test was used for comparison of continuous data between groups, the chi-square test or Fisher′s exact test was used for comparison of categorical data between groups, and the Kaplan-Meier method was used for survival analysis. Results At the end of the 5-year follow-up, 73 patients were diagnosed with HCC, with 21 in group A and 52 in group B. Group A had a significantly higher proportion of patients with early-stage HCC (Barcelona Clinic Liver Cancer stage A) than group B [66.7% (14/21) vs 15.4% (8/52),χ2=18.685,P<0.001]. Group A also had a significantly higher proportion of patients who underwent radical surgery than group B (76.2% vs 36.5%,χ2=9.424,P=0.002). The patients with HCC were followed up to the endpoint, and compared with group B, group A had a significantly longer cumulative survival time (66.4±8.0 months vs 38.1±4.5 months,t=4.295,P=0.038) and a significantly higher cumulative survival rate [71.4% (15/21) vs 46.2% (24/52),χ2=3.840,P=0.043]. Conclusion For patients with hepatitis B cirrhosis, a 3-month screening interval can increase the early detection rate of HCC, bring the opportunity of radical treatment for these patients, and prolong their survival time.
hepatitis B virus; liver cirrhosis; carcinoma, hepatocellular; early diagnosis; prognosis
10.3969/j.issn.1001-5256.2017.07.019
2017-01-25;
2017-03-02。
佑安肝病艾滋病基金(YNKT20160024)
李鵬(1977-),男, 副主任醫師,主要從事肝硬化門靜脈高壓的機制及肝癌早期篩查及診斷方面的研究。
R735.7
A
1001-5256(2017)07-1301-04
猜你喜歡
天津醫科大學學報(2019年3期)2019-08-13 06:53:08
中成藥(2016年8期)2016-05-17 06:08:14
癌癥進展(2016年12期)2016-03-20 13:16:17
罕少疾病雜志(2016年5期)2016-03-11 16:34:44
吉林大學學報(醫學版)(2015年1期)2015-12-17 07:47:28
腫瘤預防與治療(2015年1期)2015-09-26 07:26:20
中國當代醫藥(2015年16期)2015-03-01 02:03:11
中國醫藥導報(2015年26期)2015-02-28 22:07:59
肝膽胰外科雜志(2015年4期)2015-02-27 11:12:34
肝膽胰外科雜志(2015年4期)2015-02-27 11:12:24
