中心靜脈壓在感染性休克致急性腎損傷中的作用
2017-09-12 05:35:14王彥軍賈文元張松濤
創傷外科雜志 2017年8期
王彥軍,高 蕊,賈文元,張松濤,趙 威,劉 卓,尹 文
·論 著·
中心靜脈壓在感染性休克致急性腎損傷中的作用
王彥軍,高 蕊,賈文元,張松濤,趙 威,劉 卓,尹 文
目的 分析中心靜脈壓在感染性休克致急性腎損傷(AKI)中的作用。方法 回顧性分析2012年1月-2015年1月在西京醫院急診科確診的感染性休克患者138例,經24h血流動力學監測后根據中心靜脈壓(CVP)分成兩組:CVP 6~10mmHg(63例)組和CVP 11~14mmHg(75例)組。采用每搏連續無創血壓監測系統(CNAP)監測患者血流動力學指標、AKI發病率和死亡率、乳酸等生理生化指標。統計分析CVP與感染性休克致AKI的關聯。結果 兩組患者除CVP不同外(P<0.01),其他生理指標(心率、平均動脈壓、血氧飽和度等)無統計學意義。低CVP組中AKI發病率為49.2%(31例),高CVP組中AKI發病率為78.7%(59例),高CVP組AKI發病率顯著高于低CVP組(χ2=8.12,P<0.05)。其中高CVP組的AKI Ⅲ期患者(42例)顯著多于低CVP組的AKI Ⅱ期患者(13例),χ2=8.12,P<0.05。在兩組患者治療過程中,去甲腎上腺素和多巴酚丁胺的使用沒有明顯差別。高CVP組中死亡率為48.0%(36例),顯著高于低CVP組的死亡率30.2%(19例,χ2=3.93,P<0.05)。相關分析表明,CVP和感染性休克致AKI死亡率呈正相關(r=0.80,P<0.01)。結論 中心靜脈壓處于較高水平狀態增加感染性休克致急性腎損傷的發病率和死亡率。降低CVP可能會降低感染性休克致AKI的死亡率。
腎損傷;中心靜脈壓;休克
感染性休克所致急性腎損傷(AKI)是ICU危重患者中常見的一種器官功能障礙,具有很高的發病率和死亡率[1-3]。前期研究表明[4-5],在感染性休克患者中,AKI的發生率為52%。維持足夠的腎臟灌注壓,在預防感染性休克所致AKI中具有重要作用,但是也有文獻報道[6-7],正常甚至略高的中心靜脈壓可能增加AKI的死亡率。為此,本文通過回顧性分析感染性休克所致急性腎損傷患者的資料,分析中心靜脈壓(CVP)在AKI中的作用。
臨床資料
1 一般資料
回顧性分析2012年1月-2015年1月在西京醫院急診科收治采用血流動力學監測,年齡>18周歲,存活時間>24h確診為感染性休克的患者138例。
2 AKI的診斷標準
采用2005年急性腎損傷網絡(AKIN)制定的AKI分期標準,AKIN1:血肌酐增加到基線1.5~2倍,尿量<0.5mL/(kg·h)超過6h;AKIN2:血肌酐增加到基線2~3倍,尿量<0.5mL/(kg·h)超過12h;AKIN3:血肌酐增加超過基線3倍,尿量<0.3mL/(kg·h)超過24h。
3 CVP測量
鎖骨下靜脈留置中心靜脈導管,壓力傳感器接監護儀(邁瑞),通過方波讀取CVP數值。
4 血流動力學監測
使用每搏連續無創血壓監測系統(CNAP Monitor 500)進行檢測。統計心率、平均動脈壓、心排量、每搏輸出變異率等指標。
5 統計學分析

結 果
1 一般資料
入選患者138例,其中因創傷救診的患者82例,包括道路交通傷35例(42.7%),墜落傷10例(12.2%),擠壓傷8例(9.7%),銳器傷29例(35.4%)。其中肺部感染77例(55.8%),腹腔內感染29例(21.0%),其他感染(包括血行感染、皮膚軟組織感染、中樞神經系統感染等)32例(23.2%)。依據CVP差異分為兩組,高CVP組(11~14mmHg)75例,低CVP組(CVP 6~10mmHg)63例。兩組患者除CVP存在顯著差異外(P<0.05),在年齡、性別、血紅蛋白、血清肌酐、感染類型等差異無統計學意義(表1)。
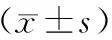
表1 患者基本資料及臨床指標比較
**P<0.01
2 AKI發病率及程度比較
兩組感染性休克患者中AKI共計90例(65.2%),低CVP組中AKI發病率為49.2%(31例),高CVP組中AKI發病率為78.7%(59例),高CVP組AKI發病率顯著高于低CVP組,χ2=13.10,P<0.01。55例AKIN3期患者中,高CVP組42例,與低CVP組相比差異有統計學意義,χ2=8.12,P<0.05(圖1)。
3 兩組患者血流動力學數據
兩組患者在進行CNAP監測24h后,低CVP組的中心靜脈壓低于高CVP組,兩者差異有統計學意義(P<0.01)。而兩組患者的收縮壓、舒張壓、心率、心排量、心指數、每搏輸出量、每搏輸出指數、脈壓差變異率、每搏輸出變異率、血管外周阻力、血管外周阻力指數等生理生化指標在兩組中無統計學意義(表2)。
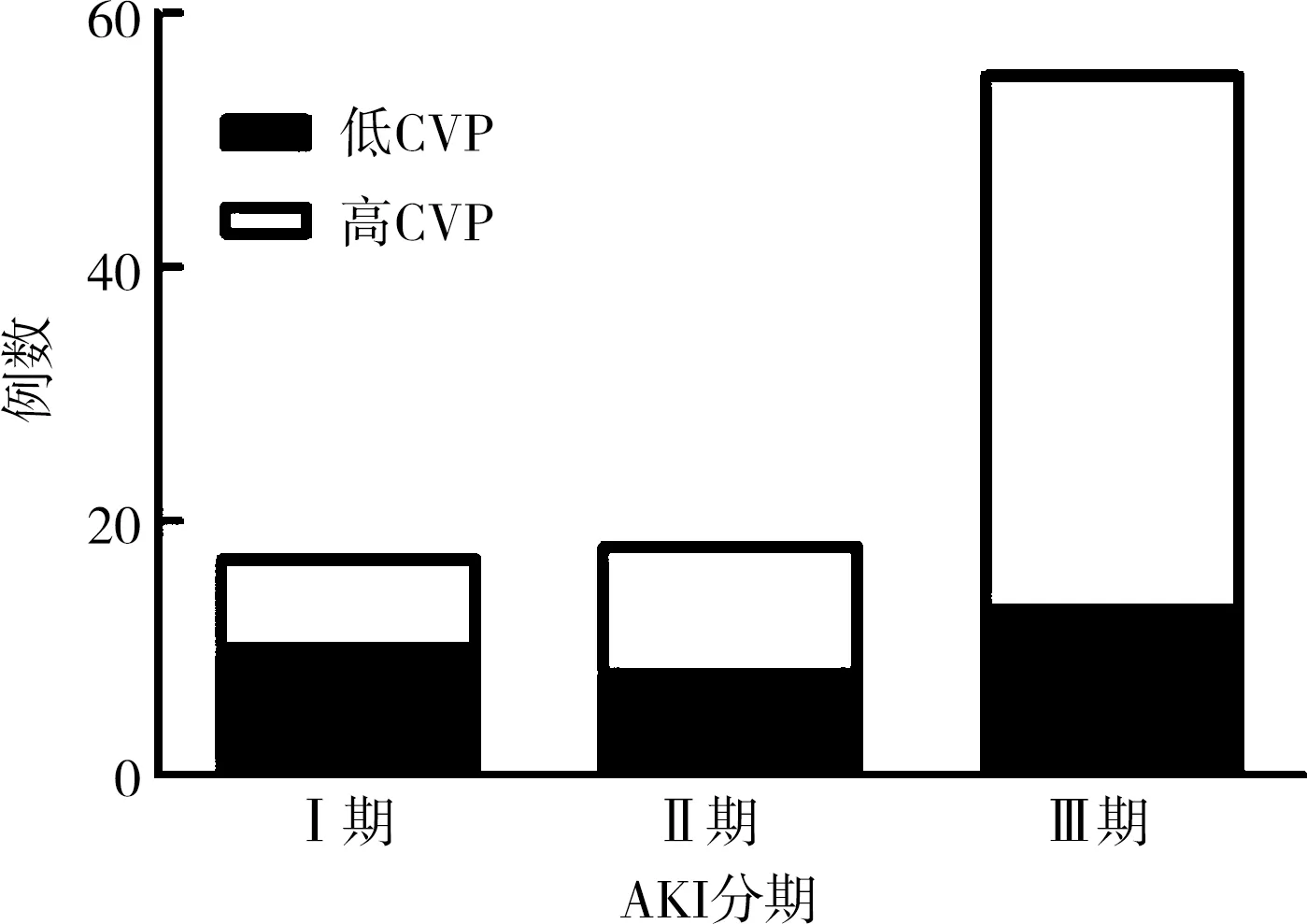
圖1 兩組感染性休克致AKI不同分期比較
4 兩組患者治療比較
為維持血壓和心輸出量,兩組患者均給予了去甲腎上腺素和多巴酚丁胺。兩組中共有47例使用了多巴酚丁胺,低CVP組30例,高CVP組17例,χ2=4.63,P<0.05,差異有統計學意義。而去甲腎上腺素的使用例數差異無統計學意義,χ2=0.02,P=0.88(圖2)。
表2 兩組感染性休克患者進行CNAP監測24h后血流動力學比較
圖2 兩組患者去甲腎上腺素和多巴酚丁胺使用比較
與此同時,低CVP組使用利尿劑33例,甘露醇5例,萬古霉素24例,血管緊張素轉化酶抑制劑/血管緊張素受體阻滯劑3例,造影劑3例,氨基糖苷類3例,非甾體抗炎藥18例以及兩性霉素16例;高CVP組使用利尿劑36例,甘露醇1例,萬古霉素21例,血管緊張素轉化酶抑制劑/血管緊張素受體阻滯劑4例,造影劑3例,氨基糖苷類7例,非甾體抗炎藥19例以及兩性霉素20例;但在兩組患者中差異無統計學意義。
5 兩組患者死亡率比較
在低CVP組患者中,ICU中死亡13例(20.6%),28d內死亡16例(25.4%);在高CVP組患者中,ICU死亡32例(42.7%),28d內死亡37例(49.3%)。ICU中高CVP組死亡率顯著高于低CVP組(χ2=3.93,P<0.05)。28d內高CVP組死亡率高于低CVP組(P>0.05),見圖3。與此同時,AKI患者的死亡率(31.2%)顯著高于非AKI患者的死亡率(7.3%),χ2=4.59,P<0.05。以28d內死亡率為橫坐標,以中心靜脈壓為縱坐標,進行相關分析表明,隨著CVP升高,死亡率逐漸增加,相關系數r=0.80,P<0.01(圖4)。

a.ICU和28d死亡率;b.AKI和非AKI死亡病例數
圖3 兩組患者死亡率比較
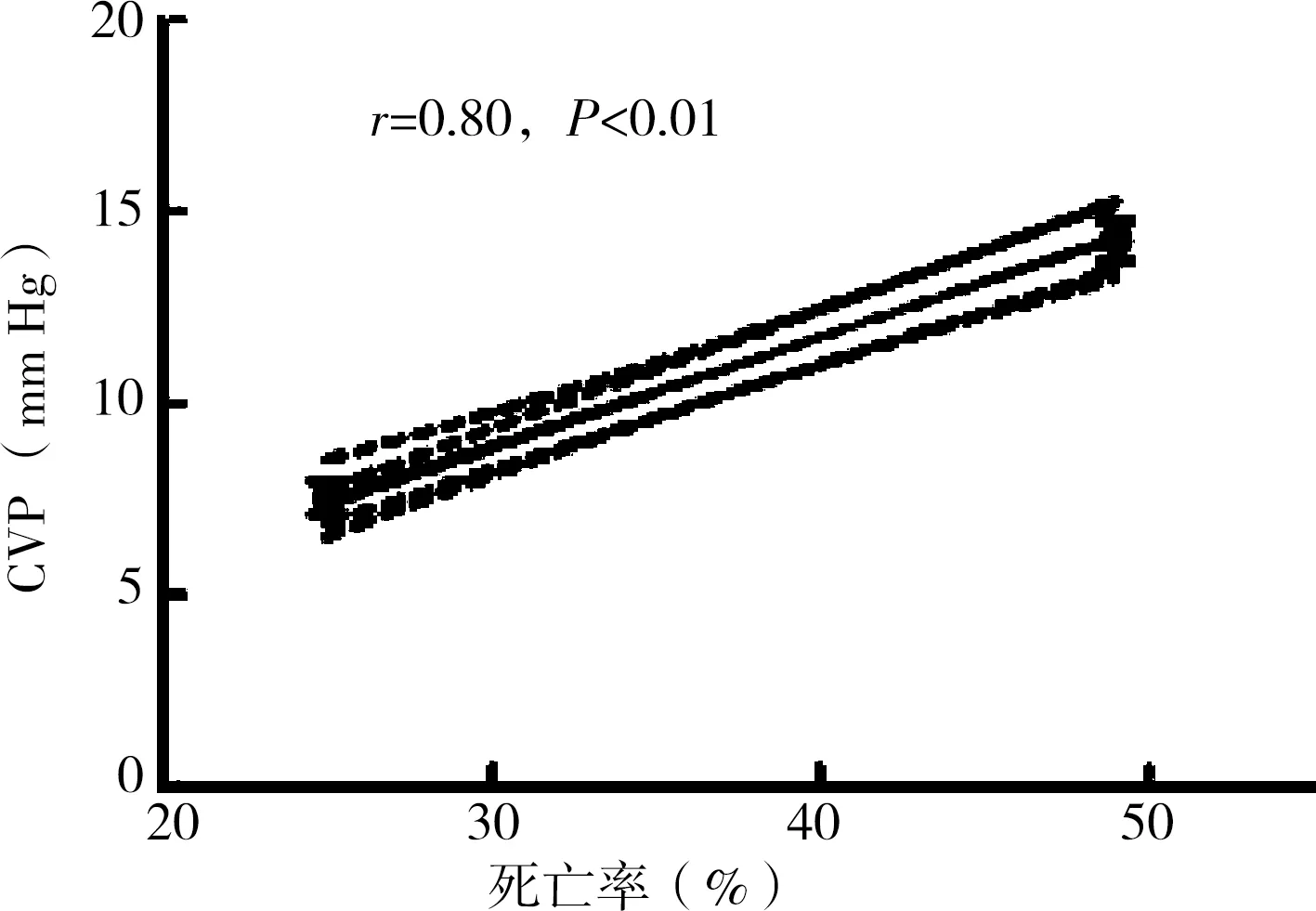
圖4 死亡率和CVP相關分析
討 論
感染性休克致急性腎損傷是一種常見而重要的器官功能障礙,許多學者[8-10]進行了感染性休克致AKI的發病機制和治療的研究,但其發病率和致死率仍很高[11]。本研究發現AKI占感染性休克患者比例為65.2%(90例)。AKI的死亡率顯著高于非AKI患者,這使得感染性休克致AKI的發病機制的研究十分重要。
本文通過中心靜脈壓對感染性休克致AKI患者進行分組進行研究,結果表明,隨CVP升高,AKI發病率和損傷程度加重,同時伴有死亡率增加(高CVP組49.3%vs. 低CVP組25.4%)。但是CVP不同的兩組患者在其他生理生化、血流動力學監測指標等方面并無差異[12]。
Lopes等[13-14]研究顯示,高心輸出量使得腎血流量顯著升高。但是在低輸出量下,腎灌注顯著減少,AKI發生率顯著增加。這表明心輸出量和AKI關系密切[8,15-16],但是在本研究中兩組患者使用去甲腎上腺素和多巴酚丁胺并無差異,這暗示AKI發病率與腎灌注及CVP均有相關性。
簡而言之,AKI在感染性休克患者中的發病率較高,且血流動力學在AKI的預防中有重要的意義[17]。同時還應該注意中心靜脈壓升高在AIK發生中的作用,較高的CVP暗示可能有較高的AKI發病率和死亡率。
[1] Sasai T,Tokioka H,Fukushima T,et al. Reliability of central venous pressure to assess left ventricular preload for fluid resuscitation in patients with septic shock[J].J Intensive Care,2014,2(1):1-7.
[2] Baratloo A,Rahmati F,Rouhipour A,et al.Correlation of blood gas parameters with central venous pressure in patients with septic shock: a pilot study[J].Bulletin Emergency Trauma,2014,2(2):77-81.
[3] Bagshaw SM,Cruz DN.Fluid overload as a biomarker of heart failure and acute kidney injury [J].Contrib Nephrol,2010,164:54-68.
[4] Wang XT,Yao B,Liu DW,et al.Central venous pressure dropped early is associated with organ function and prognosis in septic shock patients: a retrospective observational study[J].Shock,2015,44(5):426-430.
[5] Mamani M,Hashemi SH,Hajilooi M,et al. Evaluation of fibronectin and C-reactive protein levels in patients with sepsis: a case-control study [J].Acta Medica Iranica,2012,50(6):404-410.
[6] Hayashi K,Enomoto Y,Nishimura N,et al.Higher central venous pressure is associated with development of acute kidney injury in septic pediatric patients [J].J Crit Care,2015,30(4):851.
[7] 殷俊,俞鳳.感染性休克伴急性腎損傷的臨床研究[J].安徽醫藥,2015,19(8):1499-1502.
[8] Flynn A,Mani BC,Mather PJ.Sepsis-induced cardiomyopathy: a review of pathophysiologic mechanisms [J].Heart Failure Rev,2010,15(6):605-611.
[9] Ye HW,Xu CY,Feng Y,et al.Comparison analysis of stroke volume variation and central venous pressure monitoring in fluid resuscitation of elderly patients with septic shock[J].J Clin Emerg,2014,15(4):210-213.
[10] 謝逢春,劉鳳鳴,黃彬,等.感染性休克致急性腎損傷的危險因素分析[J].海南醫學,2015,26(1):98-100.
[11] 李峰,顧維立,陳立明.感染性休克預后的影響因素分析[J].南通大學學報(醫學版),2014,34(5):372-374.
[12] Richard J C,Bayle F,Bourdin G,et al.Preload dependence indices to titrate volume expansion during septic shock: a randomized controlled trial [J].Crit Care,2015,19(1):1-13.
[13] Lopes JA,Jorge S,Resina C,et al.Acute kidney injury in patients with sepsis: a contemporary analysis[J]. Int J Infect Dis,2009,13(2):176-181.
[14] Mikor A,Trásy D,Németh MF,et al.Continuous central venous oxygen saturation assisted intraoperative hemodynamic management during major abdominal surgery: a randomized,controlled trial [J].BMC Anesthesiol,2015,15(1):1-10.
[15] 寧波,馬宇潔,黃進,等. 萬古霉素對膿毒癥患者腎功能的影響[J].中華臨床醫師雜志,2013,7(1):93-95.
[16] 楊榮利,王小亭,劉大為.感染性休克致急性腎損傷的血流動力學特征及對預后的意義[J].中華內科雜志,2009,48(9):715-719.
[17] Legrand M,Dupuis C,Simon C,et al.Association between systemic hemodynamics and septic acute kidney injury in critically ill patients: a retrospective observational study[J].Crit Care,2013,17(6):1-8.
(本文編輯:黃利萍)
Effect of central venous pressure on septic shock induced acute kidney injury
WANGYan-jun1,GAORui2,JIAWen-yuan1,ZHANGSong-tao1,ZHAOWei1,LIUZhuo3,YINWen1
(1.Department of Emergency,Xijing Hospital,Fourth Military Medical University,Xi’an 710042,China; 2.Department of Respiration,Xi’an Children’s Hospital,Xi’an 710043,China; 3.Department of Neurosurgery,Xidian Group Hospital,Xi’an 710077,China)
Objective To explore the correlation between central venous pressure (CVP) on septic shock induced by acute kidney injury (AKI). Methods Patients diagnosed with septic shock admitted to emergency department of Xijing Hospital (Xi’an) between Jan.2012 and Jan.2015 were retrospectively studied. A total of 138 patients with septic shock were included, and they were divided into low central venous pressure (LCVP) group and high central venous pressure (HCVP) group. The death rate, incidence of AKI, and hemodynamics indexes were measured. The correlation between CVP and AKI was analyzed by SPSS. Results While there was a significant difference in the CVP between the two groups (P<0.01), other physiological and biochemical indexes (age, Scr) were not significantly different. The morbidity of AKI was higher in HCVP group (n=59) than LCVP group (31),χ2=8.12,P<0.05. Moreover, the number of AKIN3 was significantly more in HCVP group (n=42) than LCVP group (n=13,χ2=8.12,P<0.05). During the treatment process, there was no significant difference in the application of norepinephring and dobutamine. The death rate was also higher in HCVP group(48.0%) than LCVP group(30.2%,χ2=3.93,P<0.05). Correlation analysis showed that CVP and the death rate of AKI were positively correlated (r=0.80,P<0.01). Conclusion High CVP increases the morbidity and mortality of AKI. Decreased CVP may reduce mortality in septic shock-induced AKI.
kidney injury; central venous pressure; shock
1009-4237(2017)08-0566-04
710032 西安,第四軍醫大學西京醫院急診科(王彥軍,賈文元,張松濤,趙威,尹文);710043 西安,西安市兒童醫院(高蕊);710077 西安,西安市西電醫院(劉卓)
尹文,E-mail:xjyyyw@fmmu.edu.cn
R 631.4
A
10.3969/j.issn.1009-4237.2017.08.002
2016-07-14;
2016-10-11)
