2型糖尿病患者眶額皮層相關功能連接的功能MRl研究
2017-09-29 08:30:38陳娟劉珺劉煌輝劉華生鄧靈靈李美嬌容鵬飛王維
磁共振成像 2017年5期
陳娟,劉珺,劉煌輝,劉華生,鄧靈靈,李美嬌,容鵬飛,王維
2型糖尿病患者眶額皮層相關功能連接的功能MRl研究
陳娟,劉珺,劉煌輝,劉華生,鄧靈靈,李美嬌,容鵬飛,王維*
作者單位:中南大學湘雅三醫院放射科長沙410013
目的 探索2型糖尿病對眶額皮層與其它腦區之間的相關功能連接是否存在異常。材料與方法 對27名不伴有腦血管病變影像征象的2型糖尿病患者及21名正常志愿者進行常規MRI及靜息態功能MRI掃描,計算雙側眶額皮層與全腦其它體素間的功能連接值,并進行組間比較,選取組間具有顯著差異的腦區,并計算其功能連接的平均值,與臨床指標做相關性分析。結果 與正常對照組相比,2型糖尿病患者左側眶額皮層內側后部與左側中腦、右側下丘腦、雙側丘腦的功能連接強度顯著減低。其中2型糖尿病患者左側眶額皮層內側后部與左側中腦之間的功能連接平均值與空腹血糖值存在正相關(t=2.3727,P=0.028)。結論 2型糖尿病患者眶額皮層與多個腦區的功能連接存在異常,其中左側眶額皮層內側后部與左側中腦之間的功能連接異常與血糖控制的好壞程度相關。說明2型糖尿病可能損傷了獎賞系統的相關通路,從而導致攝食紊亂。
糖尿病,2型;眶額皮層;靜息態功能連接;磁共振成像
2型糖尿病的致病因素眾多,超重或肥胖因其會導致胰島素抵抗而成為2型糖尿病的重要病因之一,而超重及肥胖常常由于過度攝食而引發[1]。許多的研究證明了攝食行為的紊亂與肥胖及2型糖尿病的出現有密切聯系[2-3]。攝食行為受大腦獎賞系統的調控,當獎賞系統異常時會引起過度飲食,進而導致肥胖[4]。眶額皮層作為獎賞系統的重要組成部分,能根據傳入和傳出信息來調節獎賞和攝食行為[5]。以往圍繞攝食以及能量平衡的研究發現:2型糖尿病患者、肥胖者眶額皮層灰質體積較正常人減小[6-7];功能MRI (functional MRI,fMRI)的研究顯示,超重的志愿者接受高熱量食物圖片刺激時,眶額皮層活動顯著減低[8];1型糖尿病患者在低血糖狀態時,眶額皮層、杏仁核等多個腦區的活動減低[9]。這些研究表明了肥胖或糖尿病患者眶額皮層的結構和區域活動存在異常。然而眶額皮層與其他腦區的功能連接在2型糖尿病患者中的改變情況仍不明確。
2型糖尿病常常合并有微血管病變。以往的研究發現腦微血管病變會損害認知功能、白質微結構以及腦網絡結構[10-12]。因此,本研究采用靜息態fMRI (resting-state fMRI,rs-fMRI)方法研究不伴有腦血管病變影像學征象的2型糖尿病患者眶額皮層與其他腦區間的功能連接情況,旨在明確2型糖尿病對眶額皮層的功能連接是否存在損傷,為進一步探索2型糖尿病的神經損傷機制提供依據。
1 材料與方法
1.1 研究對象
本研究共招募了27名不伴有腦血管病變影像征象的2型糖尿病患者以及21名正常志愿者。2型糖尿病患者入組標準:(1)確診為2型糖尿病,病程1年以上;(2)年齡:30~70歲;(3)右利手;(4)溝通無障礙;(5)生活自理;(6)眼底檢查無眼底血管異常。排除標準:(1)既往患腦腫瘤、腦外傷、中風、癡呆、中樞神經系統感染、多發性硬化以及精神類疾病(精神分裂癥、抑郁癥等);(2) MRI檢查存在血管并發癥及其他腦部器質性疾病,如腦白質變性、腔梗、腦軟化灶、腦微出血等;(3)有酗酒史及藥物濫用史;(4)患有冠心病及高血壓;(5)MRI檢查各項禁忌證。本研究已通過中南大學湘雅三醫院倫理委員會批準,所有志愿者均簽署知情同意書。
1.2 MRI數據采集
所有受試者均由同一名操作熟練的技師在Avanto 1.5 T MRI掃描儀(西門子公司,德國)進行頭部MRI,掃描過程中囑受試者安靜、清醒,保持頭部靜止、閉眼。掃描序列如下:(1)頭部MRI掃描常規序列:包括T1WI,T2WI及T2壓水序列;(2)高分辨率全腦3D T1WI結構像,掃描參數:TR 1900 ms,TE 2.93 ms,FA 15°,層厚1.0 mm,層間距0 mm,層數176,矩陣128×128,FOV 240 mm×240 mm,NEX為1.0,掃描時間7 min 3 s;(3) rs-fMRI,EPI,掃描參數設置為:TR 2000 ms,TE 40 ms,FA 90°,層厚4.0 mm,層間距1.0 mm,層數28,矩陣64×64,FOV 240 mm×240 mm,NEX為1.0,掃描時間8 min 26 s,共掃描250個全腦圖像。
1.3 MRI數據處理
靜息態數據采用DPARSF (http://restfmri.net)軟件進行預處理:(1)排除前10個全腦EPI數據(排除掃描開始時被試不適應對圖像質量造成的影像),對余下的240個全腦EPI數據進行圖像層校準和運動校正;(2)采用仿射變換把數據轉換到標準MNI(montreal neurological institute,MNI)空間,并把體素大小重采樣設定為3 mm×3 mm×3 mm;(3)采用0.01~0.10 Hz的數據濾波去除噪聲干擾;(4)根據Friston 24參數模型[13]剔除頭動的影響。
采用基于體素的方法,選取雙側眶額皮層為種子點,計算種子點與大腦其他各體素之間的功能連接,獲得大腦功能連接圖。種子點來源于SPM結構工具箱(SPM Anatomy toolbox,http://www.fz-juelich.de/inm/inm-1/DE/Forschung/_docs/SPMAnatomyToolbox/-SPMAnatomyToolbox_node.html),該工具箱結合細胞組織形態和fMRI數據對大腦進行分區,將雙側眶額皮層分成外側、內側前部、內側后部共6個區域(圖1),以這6個區域為種子點,計算它們與大腦其他體素間的功能連接,并采用Fisher轉換把計算得到的功能連接值轉換為z值。
1.4 統計分析
采用SPSS 20.0軟件對兩組受試者的一般指標(年齡、受教育年限、體重指數、收縮壓、舒張壓)和生化指標(空腹血糖、餐后2 h血糖、空腹胰島素、糖化血紅蛋白、空腹C肽)行兩樣本t檢驗,對性別行χ2檢驗。
比較兩組被試眶額皮層功能連接的差異,統計模型采用雙樣本t檢驗和FDR校正,P<0.05有統計學意義,最小連續體素簇(continuous voxels)設為10。顯著性結果用軟件xjview(http://www.alivelearn.net/xjview8/)呈現。提取存在顯著組間差異的腦區的功能連接平均值,與患者的糖尿病指標(如空腹血糖、腰圍、糖化血紅蛋白等)作線性回歸分析(功能連接值作為因變量,糖尿病指標作為自變量)。
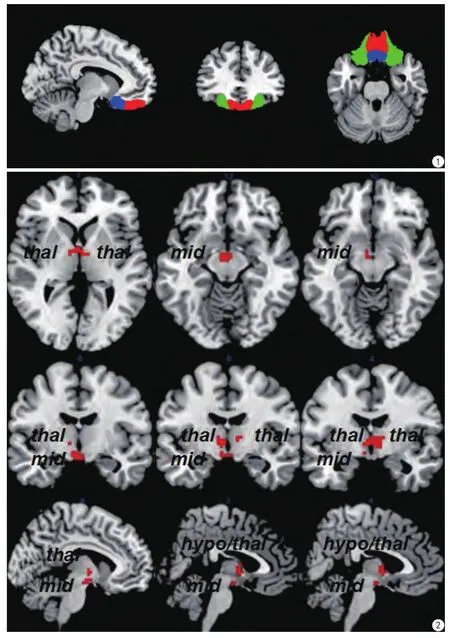
圖1 種子點示意圖。綠色:眶額皮層外側;紅色:眶額皮層內側前部;藍色:眶額皮層內側后部 圖2 與左側眶額皮層內側后部功能連接存在顯著組間差異的腦區。thal:丘腦;mid:中腦;hypo/thal:下丘腦和丘腦Fig. 1 Seed point diagram. Green: the lateral of OFC. Red: the anterior of medial OFC. Blue: the posterior of medial OFC. Fig. 2 Brain regions with signi ficantly altered functional connectivity with the posterior of left medial OFC (left orbitofrontal cortex). thal: thalamus. mid: midbrain. hypo/thal:hypothalamus/thalamus.
2 結果
2.1 一 般資料
共有48例對象納入實驗,2型糖尿病組(以下簡稱糖尿病組)27例(男18例,女9例),正常對照組21例(男14例,女7例),兩組的性別匹配,年齡、受教育年限、體重指數、收縮壓及舒張壓均沒有明顯差異,空腹血糖、餐后2 h血糖、糖化血紅蛋白(HbA1c)、胰島素抵抗指數等指標有顯著差異(表1)。
2.2 眶額皮層的功能連接結果
兩組比較結果顯示:糖尿病組患者左側眶額皮層與多個腦區間的功能連接情況存在顯著性差異,其中左側眶額皮層內側后部與左側中腦、右側下丘腦、雙側丘腦的功能連接強度低于正常組(P<0.05 )(表2,圖2)。
2.3 眶額皮層連接異常與糖尿病指標相關性分析結果
分析糖尿病組左側眶額皮層功能連接強度的減低與BMI、空腹血糖、糖化血紅蛋白、胰島素抵抗指數間的相關性,結果顯示左側眶額皮層內側后部與左側中腦間的功能連接強度與空腹血糖值存在正相關(t=2.3727,P=0.028),與BMI、糖化血紅蛋白、胰島素抵抗等指數差異無統計學意義(P>0.05)。
3 討論
本研究采用rs-fMRI的方法,探討了未發現腦血管病變影像學征象的2型糖尿病患者眶額皮層相關功能連接的改變。結果發現,2型糖尿病患者左側眶額皮層與雙側丘腦、左側中腦及右側下丘腦之間的功能連接強度顯著低于正常對照組,其中左側眶額皮層內側后部與左側中腦的功能連接平均值與空腹血糖值存在相關性。
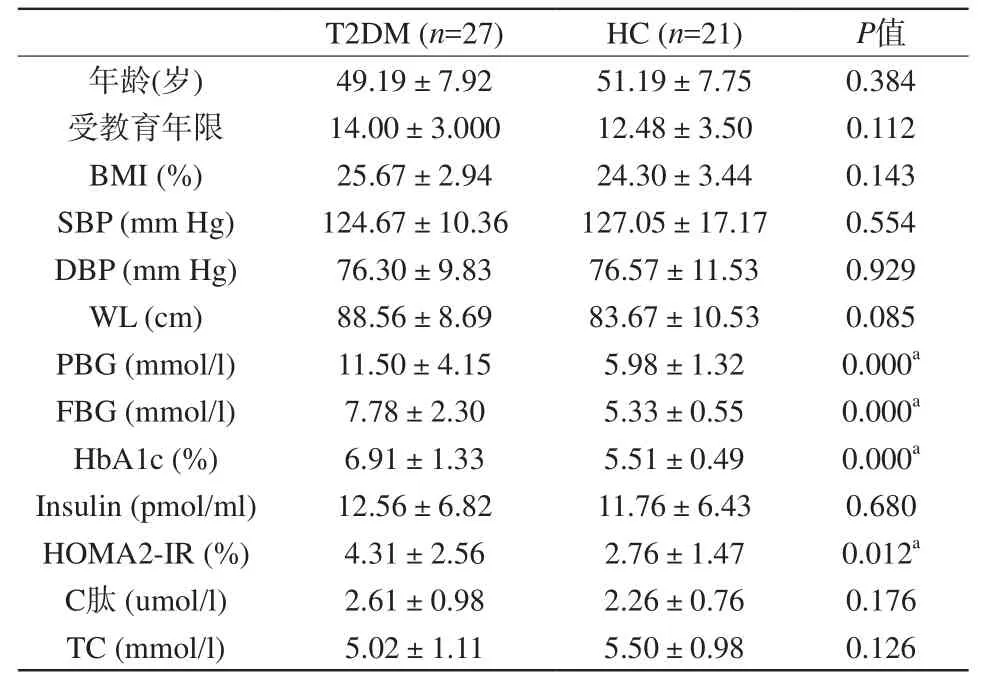
表1 2型糖尿病組與正常對照組基本臨床資料比較Tab. 1 Demographic information and part clinical data of two groups
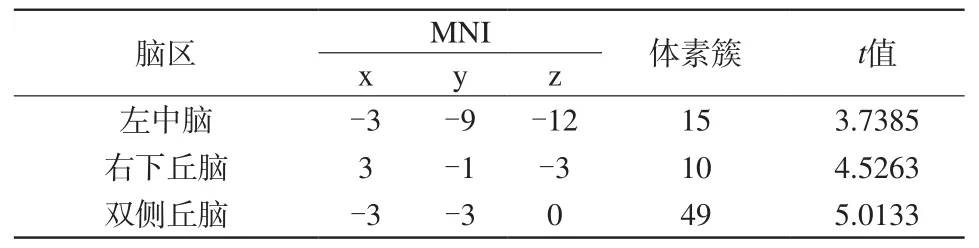
表2 2型糖尿病患者中與左側眶額皮層存在異常連接的腦區Tab. 2 Brain regions with signi ficant altered functional connection with left orbitofrontal cortex in T2DM group
眶額皮層(orbitofrontal cortex,OFC)是位于額葉前下方的前額皮層,接受來自多個腦區的直接神經傳入,包括杏仁核、背內側丘腦、顳葉、腹側背蓋區以及嗅覺系統,它的傳出神經可投射至杏仁核、下丘腦外側、海馬、扣帶回及顳葉。研究發現眶額皮層參與了包括味覺、嗅覺以及視覺相關的多種信息傳遞[7]。以往的動物及人體的MRI研究證實了眶額皮層與多個腦區之間存在功能連接[14-16],其中包括下丘腦、杏仁核、腦干等,這與筆者的發現是一致的。也有研究證實,在肥胖者、糖尿病患者中眶額皮層結構和功能受損:Kumar等[6]發現2型糖尿病患者眶額皮層灰質體積減少;Wessels等發現2型糖尿病患者低血糖狀態下眶額皮層的活動減低[9]。研究發現肥胖者腦功能網絡存在異常,涉及的腦區有:代謝感知和整合作用的腦區,如腦島、下丘腦[1];處理獎賞事件的腦區,如紋狀體、眶額皮層[17]。這些結果表明肥胖和糖尿病確實能損傷眶額皮層的結構和功能,這為本研究的發現提供了實驗證據,同時本研究結果也豐富了眶額皮層在2型糖尿病中異常改變的表現。
本研究結果顯示2型糖尿病患者左側眶額皮層內側后部與右側下丘腦的功能連接強度顯著低于正常組,說明左側眶額皮層與下丘腦之間的協同作用可能出現異常。下丘腦在能量平衡控制中起著至關重要的作用,它能直接感知血糖等營養物質的刺激并調節其代謝[18]。早期的研究發現,正常人口服或靜脈注射葡萄糖后下丘腦的活動被抑制[19]。在肥胖動物模型中發現下丘腦對營養物質的感受功能是受損的[20]。在肥胖者15以及2型糖尿病患者16中也發現,當血糖升高時,下丘腦對葡萄糖的抑制作明顯減弱[21-22]。Hirose等[23]證明了眶額皮層與下丘腦之間存在直接或間接聯系。近期的研究也發現2型糖尿病患者下丘腦與眶額皮層間功能連接強度顯著低于正常對照組[24]。因此推測眶額皮層與下丘腦之間的通路可能參與攝食行為相關的調控。
本研究的另一個重要結果是,2型糖尿病患者左側眶額皮層內側后部與左側中腦的功能連接減低。中腦介于間腦和腦橋之間,作為腦干的重要組成部分,在內臟活動調節中起到了重要作用[25]。大腦的獎賞系統由多巴胺邊緣系統調控。而已有研究證實,邊緣系統與中腦被蓋、中央灰質間存在著密切聯系[26-27]。嚙齒動物實驗發現中腦腹側被蓋區(VTA)和伏隔核(NAc)對瘦素和生長素釋放肽有反應,而瘦素能激活中腦多巴胺能神經元,表明中腦及伏隔核通過整合穩態信號,從而參與調節機體攝食及獎賞活動[28]。Cole等[29]利用PET和fMRI相結合的方法,證實了中腦多巴胺D3受體信號是參與機體目標導向行為的重要信號分子,他們的研究還發現,眶額皮層與獎賞結構(包括扣帶回、島葉及海馬旁回等)腦區網絡連接的差異與中腦多巴胺D3受體的有效性具有相關性。因此,筆者大膽推測,左側眶額皮層與左側中腦間的功能連接強度減低可能是2型糖尿病患者攝食調節受損的神經基礎之一。另外,筆者發現左側眶額皮層與左側中腦間的功能連接強度與空腹血糖值呈正相關,說明這種受損與2型糖尿病患者血糖控制的好壞有關,同時可能與高血糖的神經毒素作用相關,這為臨床上解釋居高不下的血糖水平會對中樞神經系統造成損害提供了一定依據。
另外,2型糖尿病患者左側眶額皮層內側后部與雙側丘腦的功能連接強度亦顯著減低。丘腦是間腦中最大的卵圓形灰質核團,其內包含了許多具有特定功能的小核團,左、右丘腦借中間塊相連。最近,有研究認為丘腦室旁核(paraventricular nucleus of the thalamus,PVT)參與了獎賞-尋求行為的調節[30]。丘腦室旁核在介導大腦對食物的反應中起到重要作用[31]。Haight等[32]的小鼠實驗從傳入及傳出通路的角度更準確地驗證了這一作用。研究發現肥胖者丘腦以及下丘腦的活動顯著降低[33];Arbelaez等[34]發現正常人在低血糖狀態時丘腦的活動會增加,而Mangia等[35]進一步發現在1型糖尿病患者中,丘腦針對低血糖狀態的這一反應功能是受損的。這些研究表明,丘腦在進食行為和能量平衡中具有重要作用,而肥胖、糖尿病等以代謝紊亂為特點的疾病會導致丘腦相關功能的損傷。而本研究的發現從功能連接的層面證實了這一點。
綜上所述,本研究采用靜息態腦功能成像的方法,對2型糖尿病患者的全腦功能連接進行了分析,結果發現2型糖尿病患者左側眶額皮層與下丘腦、中腦以及丘腦之間的功能連接存在異常。下丘腦、中腦以及丘腦均在獎賞系統中具有重要作用,其與眶額皮層之間功能連接的異常,說明2型糖尿病獎賞系統中的部分通路可能受到了損傷,從而導致攝食紊亂。左側眶額皮層與左側中腦之間的功能連接強度與血糖水平呈正相關,說明獎賞環路的受損在一定程度上與血糖控制的好壞程度相關,提示臨床早期發現糖尿病、積極控制血糖、合理飲食具有非常重要的意義。
[References]
[1] Kullmann S, Heni M, Veit R, et al. The obese brain: association of body mass index and insulin sensitivity with resting state network functional connectivity. Human Brain Mapping, 2012, 33(5):1052-1061.
[2] Mannucci E, Tesi F, Ricca V, et al. Eating behavior in obese patients with and without type 2 diabetes mellitus. Int J Obes Relat Metab Disord, 2002, 26(6): 848-853.
[3] Herpertz S, Albus C, Lichtblau K, et al. Relationship of weight and eating disorders in type 2 diabetic patients: a multicenter study. Int J Eat Disord, 2000, 28(1): 68-77.
[4] Kenny PJ. Reward mechanisms in obesity: new insights and future directions. Neuron, 2011, 69(4): 664-679.
[5] Farr OM, Chiang-shan RL, Mantzoros CS. Central nervous system regulation of eating: insights from human brain imaging.Metabolism, 2016, 65(5): 699-713.
[6] Kumar A, Haroon E, Darwin C, et al. Gray matter prefrontal changes in type 2 diabetes detected using MRI. J Magn Reson Imaging, 2008,27(1): 14-19.
[7] Shott ME, Cornier MA, Mittal VA, et al. Orbitofrontal cortex volume and brain reward response in obesity. Int J Obes, 2015, 39(2):214-221.
[8] Killgore WD, Yurgelun-Todd DA. Body mass predicts orbitofrontal activity during visual presentations of high-calorie foods.Neuroreport, 2005, 16(8): 859-863.
[9] Dunn JT, Cranston I, Marsden PK, et al. Attenuation of amydgala and frontal cortical responses to low blood glucose concentration in asymptomatic hypoglycemia in type 1 diabetes a new player in hypoglycemia unawareness? Diabetes, 2007, 56(11): 2766-2773.
[10] Reijmer YD, Brundel M, De Bresser J, et al. Microstructural white matter abnormalities and cognitive functioning in type 2 diabetes a diffusion tensor imaging study. Diabetes Care, 2013, 36(1): 137-144.
[11] Lawrence AJ, Chung AW, Morris RG, et al. Structural network efficiency is associated with cognitive impairment in small-vessel disease. Neurology, 2014, 83(4): 304-311.
[12] Zhong YX, Zhao JN, Zhou ZM, et al. The preliminary study of resting-state functional magnetic resonance in patients with leukoaraiosis. Chin J Magn Reson Imaging, 2015, (6): 411-415.鐘毅欣, 趙建農, 周治明, 等. 腦白質疏松癥患者靜息態功能磁共振成像的初步研究. 磁共振成像, 2015 (6): 411-415.
[13] Cui Y, Jiao Y, Chen YC, et al. Altered spontaneous brain activity in type 2 diabetes: a resting-state functional MRI study. Diabetes, 2014,63(2): 749-760.
[14] Rolls ET. The functions of the orbitofrontal cortex. Brain Cogn,2004, 55(1): 11-29.
[15] Cavada C, Tejedor J, Cruz-Rizzolo RJ, et al. The anatomical connections of the macaque monkey orbitofrontal cortex: a review.Cerebral Cortex, 2000, 10(3): 220-242.
[16] Kahnt T, Chang LJ, Park SQ, et al. Connectivity-based parcellation of the human orbitofrontal cortex. J Neuroscience, 2012, 32(18):6240-6250.
[17] Coveleskie K, Gupta A, Kilpatrick LA, et al. Altered functional connectivity within the central reward network in overweight and obese women. Nutr Diabetes, 2015, 5(1): e148.
[18] Schwartz MW, Woods SC, Porte D, et al. Central nervous system control of food intake. Nature, 2000, 404(6778): 661-671.
[19] Smeets PA, Vidarsdottir S, De Graaf C, et al. Oral glucose intake inhibits hypothalamic neuronal activity more effectively than glucose infusion. Am J Physiol Endocrinol Metab, 2007, 293(3):E754-E758.
[20] Thaler JP, Yi CX, Schur EA, et al. Obesity is associated with hypothalamic injury in rodents and humans. J Clin Invest, 2012,122(1): 153-162.
[21] Parton LE, Ye CP, Coppari R, et al. Glucose sensing by POMC neurons regulates glucose homeostasis and is impaired in obesity.Nature, 2007, 449(7159): 228-232.
[22] Vidarsdottir S, Smeets PA, Eichelsheim DL, et al. Glucose ingestion fails to inhibit hypothalamic neuronal activity in patients with type 2 diabetes. Diabetes, 2007, 56(10): 2547-2550.
[23] Hirose S, Osada T, Ogawa A, et al. Lateral–medial dissociation in orbitofrontal cortex–hypothalamus connectivity. Front Hum Neurosci, 2016,10(5): 244.
[24] Deng LL, Liu J, Liu HH, et al. The functional connectivity of hypothalamus in T2DMpatients: a resting-state fMRI study. Chin J Magn Reson Imaging, 2016, 7(4): 270-276.鄧靈靈, 劉珺, 劉煌輝, 等. 2 型糖尿病患者下丘腦功能連接的靜息態功能磁共振研究. 磁共振成像, 2016, 7(4): 270-276.
[25] Broberger C, H?kfelt T. Hypothalamic and vagal neuropeptide circuitries regulating food intake. Physiol behav, 2001, 74(4):669-682.
[26] Fulton S, Pissios P, Manchon RP, et al. Leptin regulation of the mesoaccumbens dopamine pathway. Neuron, 2006, 51(6):811-822.
[27] O'Doherty JP, Deichmann R, Critchley HD, et al. Neural responses during anticipation of a primary taste reward. Neuron, 2002, 33(5):815-826.
[28] Abizaid A, Liu ZW, Andrews ZB, et al. Ghrelin modulates the activity and synaptic input organization of midbrain dopamine neurons while promoting appetite. J Clin Invest, 2006, 116(12):3229-3239.
[29] Cole DM, Beckmann CF, Searle GE, et al. Orbitofrontal connectivity with resting-state networks is associated with midbrain dopamine D3 receptor availability. Cereb Cortex, 2012, 22(12): 2784-2793.
[30] Vertes RP, Linley SB, Hoover WB. Limbic circuitry of the midline thalamus. Neurosci Biobehav Rev, 2015,54(7): 89-107.
[31] Matzeu A, Cauvi G, Kerr TM, et al. The paraventricular nucleus of the thalamus is differentially recruited by stimuli conditioned to the availability of cocaine versus palatable food. Addict Biol, 2017,22(1): 70-77.
[32] Haight JL, Fuller ZL, Fraser KM, et al. A food-predictive cue attributed with incentive salience engages subcortical afferents and efferents of the paraventricular nucleus of the thalamus.Neuroscience, 2017, 340(1): 135-152.
[33] Gautier JF, Chen K, Salbe AD, et al. Differential brain responses to satiation in obese and lean men. Diabetes, 2000, 49(5): 838-846.
[34] Arbelaez AM, Powers WJ, Videen TO, et al. Attenuation of counterregulatory responses to recurrent hypoglycemia by active thalamic inhibition a mechanism for hypoglycemia-associated autonomic failure. Diabetes, 2008, 57(2): 470-475.
[35] Mangia S, Tesfaye N, De Martino F, et al. Hypoglycemia-induced increases in thalamic cerebral blood flow are blunted in subjects with type 1 diabetes and hypoglycemia unawareness. J Cereb Blood Flow Metab, 2012, 32(11): 2084-2090.
The functional connectivity of orbitofrontal cortex in type 2 diabetes : a resting-state fMRI study
CHEN Juan, LIU Jun, LIU Huang-hui, LIU Hua-sheng, DENG Ling-ling, LI Mei-jiao,RONG Peng-fei, WANG Wei*
Department of Radiology, the Third Xiangya Hospital of Central South University,Changsha 410013, China
*Wang W, E-mail: cjr.wangwei@vip.163.com
Objective: Our aim was to detect weather the functional connectivity between the orbitofrontal cortex (OFC) and other brain regions were impaired in type 2 diabetes mellitus (T2DM). Materials and Methods: Conventional magnetic resonance imaging (MRI) and blood oxygen level dependent resting-state functional MRI were obtained from 27 diabetic patients without cerebrovascular diseases on imaging, and from 21 age-matched healthy volunteers. The functional connectivity between the bilateral OFC and other voxels of the whole brain was calculated and compared between the two groups. The brain regions with signi ficant differences between the groups were selected, then, the mean value of the functional connectivity between these regions was calculated. The correlations were analyzed with the clinical indexes. Results: Compared to the control group, the patients showed signi ficantly reduced functional connectivity between the posterior of left medial OFC and left midbrain, right hypothalamus and bilateral thalamus. In the patients group, the mean value of functional connectivity between the posterior of left medial OFC and the left midbrain was positively correlated with the value of fasting plasma glucose (t=2.3727, P=0.028). Conclusions: The functional connectivity between the left OFC and multiple brain regions in patients with type 2 diabetes mellitus was impaired, and the reduced functional connectivity value between the left OFC and the left midbrain was signi ficantly associated with the controlling of the plasma glucose, which indicated that type 2 diabetes mellitus may impaire some reward -related pathways, leading to eating disorders.
Diabetes Mellitus, Type 2; Orbitofrontal cortex; Resting-state functional connectivity; Magnetic resonance imaging
Received 16 Jan 2017, Accepted 3 Mar 2017
ACKNOWLEDGMENTSThis work was part of project of National Key Clinical Specialty (No. 2013-544). National Natural Science Foundation of China (No.81471715).
國家臨床重點專科基金項目(編號:2013-544)、國家自然科學基金項目(編號:81471715)
王維,E-mail:cjr.wangwei@vip.163.com
2017-01-16
接受日期:2017-03-03
R445.2;R338.25
A
10.12015/issn.1674-8034.2017.05.001
陳娟, 劉珺, 劉煌輝, 等. 2型糖尿病患者眶額皮層相關功能連接的功能MRI研究. 磁共振成像, 2017, 8(5): 321-326.
猜你喜歡
中華詩詞(2022年6期)2022-12-31 06:41:24
中老年保健(2022年5期)2022-08-24 02:35:42
中老年保健(2022年1期)2022-08-17 06:14:56
保健醫苑(2022年6期)2022-07-08 01:26:34
家庭科學·新健康(2022年3期)2022-05-10 00:32:13
中老年保健(2021年5期)2021-08-24 07:07:20
中老年保健(2021年11期)2021-08-22 03:15:16
中國科技論壇(2017年7期)2017-07-25 08:49:53
媽媽寶寶(2017年3期)2017-02-21 01:22:30
飼料與畜牧(規模養豬)(2016年5期)2016-12-01 03:48:40
