磁共振準連續動脈自旋標記技術在不隨意運動型腦癱患者中的初步研究
2017-09-29 08:30:38韓秉艷瑪依拉夏坎王皓賈文霄王云玲
磁共振成像 2017年5期
韓秉艷,瑪依拉·夏坎,王皓,賈文霄,王云玲
磁共振準連續動脈自旋標記技術在不隨意運動型腦癱患者中的初步研究
韓秉艷,瑪依拉·夏坎,王皓,賈文霄,王云玲*
作者單位:新疆醫科大學第二附屬醫院影像中心,烏魯木齊 830063
目的 應用磁共振準連續動脈自旋標記(pseudo-continuous arterial spin labeling,pCASL)技術觀察不隨意運動型腦癱患者腦部運動區(內囊后肢皮質脊髓束)的血流特點,通過血流變化來研究腦癱患兒運動區的功能病理基礎,為臨床治療效果及早期診斷提供影像支持。材料與方法 回顧性分析經臨床診斷為不隨意運動型腦癱患者與志愿者各20例,觀察不隨意運動型腦癱患者雙側內囊后肢皮質脊髓束運動區腦血流量的變化,通過t檢驗分析志愿者、患兒及志愿者與患兒雙側腦血流的的情況。結果 志愿者、不隨意運動型腦癱患者左、右兩側內囊后肢的皮質脊髓束運動區局部腦血流量差異有統計學意義(P<0.05),左側腦血流量高于右側。志愿者與腦癱患者左、右兩側局部腦血流量比較差異有統計學意義(P<0.05),志愿者局部腦血流量高于不隨意運動型腦癱患者。結論 雙側內囊后肢功能運動區腦血流減低是導致不隨意運動型腦癱運動區的功能病理基礎之一,可以通過磁共振pCASL技術對不隨意運動型腦癱運動區的血流量進行定量分析。
腦性癱瘓;內囊;磁共振成像
不隨意運動型腦性癱瘓是錐體外系受損 引起的腦性癱瘓之一,它占所有腦癱發病率的10%~30%,其導致的運動殘疾程度往往較重,治療難度較大[1]。臨床表現主要表現為手足徐動、舞蹈樣動作、震顫等。筆者應用磁共振準連續動脈自旋標記(pseudo-continuous arterial spin labeling,pCASL)技術對不隨意型運動型腦癱患者雙側內囊后肢區域腦血流量 (regional cerebral blood flow,rCBF)進行初步研究,研究腦癱患兒運動區的功能病理基礎,通過該區域腦血流的變化為臨床治療效果進行評價,同時為常規MRI表現為陰性患者早期診斷提供影像支持,使患者得到及時診斷及相應治療。
1 材料與方法
1.1 一般資料
搜集本院2016年5月至10月被臨床診斷為不隨意運動型腦癱患者20例,志愿者20例,年齡4~15歲,平均年齡6歲。志愿者均為右利手。
1.2 方法
1.2.1 儀器與掃描方法
使用Philips公司3.0 T聚源磁共振16通道頭顱線圈,所有不配合患者經水合氯醛灌腸后進行檢查。先進行短激發 T1WI、T2WI 序列掃描后進行pCASL掃描,全部掃描時間約為7 min。具體參數:TR 4000 ms,TE 15 ms, FOV 240 mm×240 mm,層數16,層厚5.0 mm,層間距1 mm。感興趣區(ROI)為雙側內囊后肢后3/4處,面積約為16 mm×16 mm,同一部位測量三次,取平均值進行統計學分析。
1.2.2 統計方法
用SPSS 19.0軟件包對腦癱患者組及正常志愿者對照組所測量的雙側內囊后肢rCBF值進行統計分析,各組數據采用表示,先進行正態性檢驗,再進行配對及獨立樣本t檢驗進行分析比較,P<0.05為差異有統計學意義。
2 結果
志愿者、腦癱患者左、右兩側內囊后肢的皮質脊髓束運動區局部腦血流量有差異性(P<0.05),左側局部腦血流量高于右側。志愿者與腦癱患者雙側內囊后肢局部腦血流量比較差異有統計學意義(P<0.05),志愿者高于腦癱患者(表1,2;圖1)。
3 討論
不隨意運動型腦癱主要是由錐體外系損傷引起的。錐體外系統主要是指基底神經節(基底核),各核團之間通過神經纖維和神經遞質相聯系,為自主運動所必需的肌張力和姿勢做好準備。以基底節為主的錐體外系受損可引起隨意運動障礙而不隨意運動增多,表現為扭轉痙攣張力障礙,舞蹈及手足徐動等癥狀。不隨意運動型腦癱的主要病因為缺氧缺血性腦損傷和膽紅素腦病,病變主要在基底神經節區[2-3]。也有文獻報道,部分原因造成腦損傷可選擇性損傷蒼白球[4],在雙側內囊后肢后3/4處(相當于蒼白球的后緣水平)為皮質脊髓束所在區域,該區域受損會影響神經纖維的傳導,從而會引起相關臨床癥狀。
筆者通過PCASL研究不隨意運動型腦癱患者該區域的血流情況,rCBF值具有明確的臨床及生理學意義,是臨床工作中認可度較高的常用檢查技術[5],它結合了連續式 ASL 和脈沖式 ASL 優點,是一種全新無創容積灌注成像技術[6],它的短脈沖能夠減少受檢者的能量吸收率,同時還可以減輕磁化轉移效應,采集時間更短,能有效克服磁敏感及運動偽影,大大提高了圖像信噪比和標記效率,灌注圖像更均勻[7-8]。Gevers等[9]對10例健康志愿者在3個影像中心均進行pCASL、CASL和PASL檢查,結果發現pCASL聯合背景抑制法得到的數據差異性最小。目前關于pCASL的應用相關研究較多,主要應用在成人腦血管性病變、腫瘤性病變及阿爾茨海默病等中樞系統疾病較多[10-14],而在腦癱患兒中的應用研究十分少見。筆者通過對志愿者與不隨意運動型腦癱內囊后肢后3/4處局部腦血流的研究初步探討腦癱患兒的局部腦血流情況,在研究中發現正常兒童左、右兩側內囊后肢后3/4處血流情況左側局部血流高于右側,P<0.05,差異有統計學意義,可能的原因是本研究全部受試者均為右利手,長期的右手運動導致左側腦神經活動增強,從而引起左側血流量選擇性增加有關,這與劉世文等[15]手部運動可以導致腦血流相對增加的結果基本一致。另外,本研究中發現不隨意型腦癱患者左、右兩側內囊后肢后 3/4處區域性腦血流是有差別的,P<0.05,左側腦血流還是高于對側,這與志愿者局部血流表現基本一致,這是否與腦癱患兒大腦本身腦血流灌注有關還有待進一步研究,但其與正常人比較,左、右兩側腦血流量是有差別的,P<0.05,患者左、右兩側腦血流均低于正常組,腦血流量的減低導致該區域的神經纖維的發育不全或缺失從而導致錐體外系傳導通路的損傷從而造成腦損傷,引起患兒的不隨意運動增加,這也說明雙側內囊后肢后3/4處區域的腦血流對錐體外系傳導有著很重要的意義,也是導致不隨意運動型腦癱患者發病的因素之一。通過測量局部腦血流的變化,特別是在MRI常規掃描表現為陰性的患者,pCASL更能夠檢測到異常,其測量結果則更有意義,但也有局限性,由于研究對象為腦癱患兒,體位及腦部病變存在差異較大,這可能會影響部分測量的真實性,需在今后的研究中對腦部影像表現為陰性的患兒進行專門研究,來彌補這方面的缺陷,再者還需要增加樣本量來進行進一步定量研究,從而為臨床不隨意運動型腦癱患兒運動區的功能病理基礎及早期診斷及治療提供可靠的影像支持。

表1 正常組、患者組雙側內囊后肢rCBF比較Tab.1 Normal group, the patient group bilateral internal capsule hind limb rCBF comparison

表2 雙側內囊后肢患者于正常組間的rCBF比較Tab. 2 Comparison of rCBF between the bilateral hind limb patients and the normal group
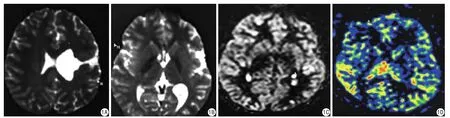
圖1 患者,女,5歲。肢體功能障礙并智力低下4年。A、B為ADC圖,A:患者診斷為左側頂葉腦裂畸形,左頂葉增寬的腦溝與左側側腦室相通;B:感興趣區選擇雙側內囊后肢后3/4處,信號相對較高的部位;C:pCASL原始圖;D:偽彩圖,左側感興趣區血流量低于右側,紅色為高灌注區,右側感興趣區紅色范圍明顯大于左側Fig. 1 Female, 5 years old, and limb dysfunction and mental retardation for 4 years, A, B: ADC figures. A: Patient with left parietal lobe cleft, sulcus and left lateral ventricle with left parietal lobe broadening. B: Region of interest selection of bilateral posterior limb of the internal capsule 3/4, signal relatively high position. C: pCASL figure. D: The original pseudo color, the left side of blood flow in the region of interest was lower than the right, red for high perfusion area, right ROI red range was signi ficantly larger than the left.
pCASL技術不僅可以對全腦灌注還可以對區域性血流灌注進行定量分析,其作為一種無創的影像學檢查方法將對腦癱的血流動力學研究有著十分重要的價值。
[References]
[1] Li XJ, Tang JL, Ma BX et al. The definition of cerebral palsy,diagnostic criteria and clinical classification. Chin J Appl Clin Pediatr, 2014, 29(19): 1520.李曉捷, 唐久來, 馬丙祥, 等. 腦性癱瘓的定義、診斷標準及臨床分型. 中華實用兒科臨床雜志, 2014, 29(19): 1520.
[2] Ahlfors CE, Wennberg RP, Ostrow JD, et al. Unbound (free)bilirubin: improving the paradigm for evaluating neonatal jaundice.Clin Chem, 2009, 55(7): 1288-1299.
[3] Johnston MV,Hoon AH Jr. Possible mechanisms in infants for selective basalganglia damage from asphyxia, kemicterus, or mitochondrial encephalopathies. J Child Neurol, 2000, 15(9):588-591.
[4] Sugama S, Soeda A, Eto Y. Magnetic resonance imaging in three with children kernicterus. Pediatric Neurolog, 2001, 25(4): 328-331.
[5] Zhu YF, Lu Q, Li GQ, et al. Feasibility of applying arterial spin labeling to the study of post - acupuncture fMRI. Chin J Comb Trad Chin West Med Imag, 2016, 14(4): 373-375.朱一芳, 盧琦, 李國強, 等. 動脈自旋標記技術在針刺fMRI后效應研究中的可行性分析. 中國中西醫結合影像學雜志, 2016, 14(4):373-375.
[6] Huang D, Wu B, Shi K, et al. Reliability of three-dimensional pseudo-continuous arterial spin labeling MR imaging for measuring visual cortex perfusion on two 3 T scanners. PLoS One, 2013, 8(11):e79471.
[7] Wheaton AJ, Miyazaki M. Non-contrast enhanced MR angiography:physical principles. Magn Reson Imaging, 2012, 36(2): 286-304.
[8] Wu H, Block WF, Turski PA, et al. Noncontrast-enhanced three-dimensional (3D) intracranial MR angiography using pseudocontinuous arterial spin labeling and accelerated 3D radial acquisition. Magn Reson Med, 2013, 69(3): 708-715.
[9] Gevers S, van Osch MJ, Bokkers RP, et a1. Intra- and muhicenter reprod- ucibility of pulsed, continuous and pseudo-continuous arterial spin labeling methods for measuring cerebral perfusion. J Cereb Blood Flow Metab, 2011, 31(8): 1706-1715.
[10] Wolk DA, Detre JA. Arterial spin labeling MRI: an emerging biomarker for Alzheimer's disease and other neurodegenerative conditions. Curr Opin Neurol, 2012, 25(4): 421-428.
[11] Binnewijzend MA, Kuijer JP, Benedictus MR, et al. Cerebral blood flow measured with 3D pseudocontinuous arterial spin-labeling MR imaging in Alzheimer disease and mild cognitive impairment: a marker for disease severity. Radiology, 2013, 267(1): 221-230.
[12] Chen W, Song X, Beyea S, et al. Advances in perfusion magnetic resonance imaging in Alzheimer's disease. Alzheimers Dement, 2011,7(2): 185-196.
[13 ] Ozsunar Y, Mullins ME, Kwong K, et al. Glioma recurrence versus radiation necrosis? A pilot comparison of arterial spin-labeled,dynamic susceptibility contrast enhanced MRI, and FDG-PET imaging. Acad Radiol, 2010, 17(3): 282-290.
[14] Hendrikse J, Petersen ET, Golay X. Vasculardisorders: insights from arterial spin labeling. Neuroimaging Clin N Am, 2012, 22(2):259-269.
[15] Liu SW, Lü Z, Liu YJ, et al. A study of CBF of the cortical area activated by simple hand motor performance in normal subject as revealed by SPECT. Chin J phys Med Rehabil, 2014, 26(11):671-674.劉世文, 呂政, 劉亞杰, 等. 正常人手指簡單運動時腦功能區被激活的SPECT腦血流研究. 中華物理醫學與康復雜志, 2014, 26 (11):671-674.
The preliminary study of magnetic resonance pCASL technique in dyskinetic cerebral palsy patients
HAN Bing-yan, Mayila·Xiakan, WANG Hao, JIA Wen-xiao, WANG Yun-ling*
Department of Radiology, the Second Affiliated Hospital of Xinjiang Medical University, Urumchi 830028, China
*Wang YL, E-mail: 2824059816@qq.com
Objective: To observe the blood flow characteristics of brain movement area (posterior capsule cortex spinal cord bundle) in patients with involuntary movement of cerebral palsy by magnetic resonance pseudo-continuous arterial spin labeling(pCASL). To study the functional and pathological basis of the motor area of children with cerebral palsy by blood flow changes, and to provide the image support for clinical treatment and early diagnosis. Materials and Methods: Retrospective analysis of the clinical diagnosis of dyskinetic cerebral palsy patients and normal volunteers 20 cases,respectively, observed the change of dyskinetic cerebral palsy patients with bilateral posterior corticospinal motor area of cerebral blood flow, cerebral blood flow analysis of local motion area. t test was used to analyze the cerebral blood flow of bilateral cerebral blood flow in volunteers, children, volunteers and children. Results: There were signi ficant differences in local cerebral blood flow and corticospinal motor area volunteers dyskinetic cerebral palsy patients with left and right sides of the posterior limb of the internal capsule (P<0.05), left cerebral blood flow was higher than right.There was significant differences in cerebral blood flow between the left and right side of the patients with cerebral palsy (P<0.05). Conclusions: The function of motor area of cerebral blood flow to reduce the bilateral posterior limb of the internal capsule which is one of the basic functions of pathological dyskinetic cerebral palsy movement area, can make quantitative analysis on the blood flow through magnetic resonance pCASL technique of dyskinetic cerebral palsy movement area analysis.
Cerebral palsy; Internal capsule; Magnetic resonance imaging
Received 22 Dec 2016, Accepted 22 Mar 2017
王云玲,E-mail:2824059816@qq.com
2016-12-22
接受日期:2017-03-22
R445.2;R742
A
10.12015/issn.1674-8034.2017.05.002
韓秉艷, 瑪依拉·夏坎, 王皓, 等. 磁共振準連續動脈自旋標記技術在不隨意運動型腦癱患者中的初步研究. 磁共振成像, 2017, 8(5): 327-330.
