產前超聲對胎兒動脈導管狹窄診斷價值的研究
2017-11-07 10:12:10白明
中國醫學工程 2017年8期
白明
(山東省青島經濟技術開發區第一人民醫院 B超室,山東 青島 266555)
.論 著.
產前超聲對胎兒動脈導管狹窄診斷價值的研究
白明
(山東省青島經濟技術開發區第一人民醫院 B超室,山東 青島 266555)
目的 探究胎兒動脈導管狹窄應用產前超聲檢查的診斷價值。方法 臨床選擇2014年1月‐2016年4月該院經產前彩色多普勒超聲檢查的胎兒動脈導管狹窄孕婦50例為觀察組,同期選擇產前彩色多普勒超聲檢查健康胎兒50例為研究對照,比較兩組動脈導管的舒張期流速、收縮期流速及動脈導管內徑等臨床指標;比較兩組動脈導管前向血流速度、三尖瓣反流速度及右心室壓力等臨床指標;觀察在不同超聲切面動脈導管的超聲特征。結果 在25~36孕周和孕周超過36周孕婦中,觀察組舒張期流速、收縮期流速等指標顯著高于對照組,差異有統計學意義(P <0.05);觀察組胎兒動脈導管內徑小于對照組,差異有統計學意義(P <0.05);在孕25~36周和超過36周觀察組動脈導管前向血流速度、三尖瓣反流速度及右心室壓力均顯著高于對照組,差異有統計學意義(P <0.05)。結論 胎兒產前彩色多普勒超聲檢查可全面、客觀評估其影像特征,對診斷胎兒動脈導管狹窄具有重要的臨床價值。
胎兒動脈導管狹窄;彩色多普勒超聲;臨床價值
隨著人們對于優生優育意識逐漸重視和經濟水平的提高,產前超聲檢查已成為篩查胎兒先天性疾病的重要檢查手段之一[1]。如在胚胎發育期因受家族性因素、代謝性疾病、大劑量的放射性物質的接觸等理化因素或孕婦早期服用某些禁忌藥物、病毒感染等因素可引發動脈導管缺如、早閉、逆行灌注、狹窄等病理性改變,導致胎兒血液循環異常變化[2]。有研究指出,胎兒產前彩色多普勒超聲檢查可全面、客觀評估其影像特征,對診斷胎兒動脈導管狹窄具有重要的臨床價值[3]。胎兒動脈導管狹窄應用產前超聲檢查的診斷價值十分重要,故2014年1月‐2016年4月本院選擇臨床收治的胎兒動脈導管狹窄孕婦經產前多普勒超聲檢查,觀察其產前超聲影像特征,現報道如下。
1 資料與方法
1.1 一般資料
本院選擇2014年1月‐2016年4月臨床收治的50例胎兒動脈導管狹窄孕婦為觀察組,經產前多普勒超聲檢查,年齡25~36歲,平均(27.4±2.5) 歲;孕周25~37周,平均(29.2±2.4)周,均為單胎;初產婦30例,經產婦20例。納入標準:符合中華醫學會婦產科學會制定的胎兒產前動脈導管狹窄的診斷標準[4];經產前超聲檢查確診。同期選擇產前彩色多普勒超聲檢查健康胎兒50例為研究對照,年齡25~36歲,平均(27.3±2.4)歲;孕周25~37周,平均(29.1±2.3)周,均為單胎,初產婦29例,經產婦21例。排除標準:合并妊娠并發癥者、精神疾患者。兩組的平均年齡、平均孕周等臨床資料大體一致(P>0.05),具有可比性。
1.2 方法
對所有研究對象予以彩色多普勒超聲檢查,探頭頻率為2.2~4.2 MHz,應用凸陣式腹部探頭,孕婦取仰臥位,操作視野下顯露腹部,腹部表面放置探頭進行順序追蹤法檢查,觀察基礎為胎兒四腔心,仔細探查胎兒腔/肺靜脈回流切面、左心室流出道切面,右心室流出道切面,三血管、主動脈弓以及動脈導管弓切面等。分析其心房/心室的相互關系、大血管之間的關系,聯合頻譜多普勒超聲檢查和彩色多普勒超聲檢查,檢測動脈導管和主肺動脈的內徑、肺動脈瓣的反流速度、血流速度等臨床指標。追蹤隨訪孕婦的分娩情況;比較兩組動脈導管的舒張期流速、收縮期流速、動脈導管內徑等臨床指標;比較兩組動脈導管前向血流速度、三尖瓣反流速度、右心室壓力等臨床指標;觀察在不同超聲切面的動脈導管的超聲特征。
1.3 儀器
飛利浦EnVisor非凡超聲彩色多普勒超聲診斷 儀。
1.4 統計學方法
采用SPSS 18.0軟件系統分析所有數據。計量資料以均數±標準差(±s)表示,計量資料組間比較采用t檢驗。P<0.05為差異有統計學意義。
2 結果
2.1 兩組不同孕周的胎兒動脈導管血流參數指標及動脈導管內徑指標評估比較
在25~36孕周和孕周超過36周孕婦中,觀察組舒張期流速、收縮期流速等指標顯著高于對照組(P<0.05);而觀察組胎兒動脈導管內徑與對照組相比,顯著降低(P<0.05),見表1。
2.2 兩組動脈導管前向血流速度、三尖瓣反流速度、右心室壓力等臨床指標評估比較
在孕周25~36周和超過36周觀察組的動脈導管前向血流速度、三尖瓣反流速度及右心室壓力均顯著高于對照組,差異有統計學意義(P<0.05),見表2。
2.3 觀察不同超聲切面動脈導管的超聲特征
圖1為動脈導管前向血流速度增快頻譜聲像圖,圖2為動脈導管狹窄彩色聲像圖,及時剖腹產,產后1 d動脈導管關閉。
表1 兩組不同孕周胎兒動脈導管血流參數指標及動脈導管內徑指標評估比較 (±s)

表1 兩組不同孕周胎兒動脈導管血流參數指標及動脈導管內徑指標評估比較 (±s)
>36孕周舒張期流速/(m/s)收縮期流速/(m/s) 內徑/mm 舒張期流速/(m/s)收縮期流速/(m/s) 內徑/mm觀察組 50 0.25±0.09 0.46±0.22 4.28±0.13 0.17±0.07 0.50±0.39 2.26±0.65對照組 50 0.17±0.04 0.33±0.13 4.56±0.18 0.12±0.04 0.31±0.21 2.65±0.87 t值 5.74 3.60 8.92 4.39 3.03 2.54 P值 0.015 0.043 0.001 0.020 0.045 0.010組別 例數 25~36孕周
表2 兩組動脈導管前向血流速度、三尖瓣反流速度及右心室壓力等臨床指標評估比較 (±s)

表2 兩組動脈導管前向血流速度、三尖瓣反流速度及右心室壓力等臨床指標評估比較 (±s)
25~36孕周右心室壓力/mmHg觀察組 50 1.91±0.92 1.76±0.72 18.28±1.13 3.17±0.07 3.52±0.39 34.26±4.65對照組 50 1.17±0.04 1.33±0.33 10.56±0.18 2.12±0.04 2.31±0.21 22.65±2.87 t值 5.68 3.84 47.71 92.09 19.32 15.02 P值 0.015 0.042 0.000 0.000 0.000 0.000組別 例數>36孕周動脈導管前向血流速度/(m/s)三尖瓣反流速度/(m/s)右心室壓力/mmHg動脈導管前向血流速度/(m/s)三尖瓣反流速度/(m/s)
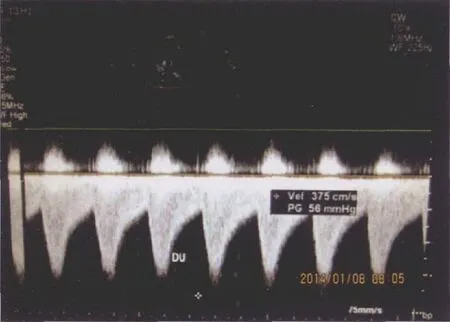
圖1 動脈導管前向血流速度增快頻譜聲像圖

圖2 動脈導管狹窄彩色聲像圖
3 討論
在孕初期2~3個月內處于胚胎發育期,此時為大血管和心臟形成的時期,若大血管或心臟形成障礙,引起解剖結構異常,或胎兒出生后,應自動關閉的通道未閉合則稱為先天性心臟病[5-6]。母體患有早期妊娠出現感染性病毒感冒高熱服藥史、酒精慢性中毒、糖尿病結締組織病、先心病家族史、羊水異常、胎兒宮內發育遲緩、心律失常及染色體異常等均會導致先天性心臟病的發生[7-8]。彩色多普勒超聲檢查是一種影像學檢查手段,對宮內胎兒疾病具有診斷作用。一般孕婦在孕20~34 周由于羊水較多,是超聲檢查的最佳時間,胎兒心影清晰、胎兒肋骨未骨化、活動度較佳,先心病畸形大多數已經形成,孕婦得知胎兒先天性心臟病的診斷及嚴重程度后,可適當做出下一步選擇[9-10]。
胎兒動脈導管是降主動脈分叉和肺動脈之間的重要連接通路,約有超過80%的肺動脈內血液通過動脈導管流入降主動脈,在胎兒出生后10~15 h后,動脈導管開始功能性閉合,60 d~1歲,大部分已經閉合,成為動脈韌帶[11-12]。胎兒期的動脈導管狹窄和缺如十分少見,胎兒期動脈導管可引發動脈導管早閉或先天性狹窄[13-14]。大部分研究指出前列腺素合成酶抑制劑促使胎兒動脈導管收縮,且隨著孕周的逐漸增加其效果更佳顯著[15-16]。孕周34周后口服非甾體藥物,胎兒動脈導管收縮的發生情況會呈指數式升高。但大部分研究對象在停止服用該抗炎藥物后,動脈導管收縮是可逆性的[17-18]。且有研究指出,當胎兒的右心室壓力、肺動脈壓升高超過60 mmHg時,可導致心律失常或右心功能衰竭,嚴重者可導致胎兒死亡。目前,對于產前超聲對胎兒動脈導管狹窄的診斷價值研究已成為醫學學者的重要研究內容[19]。
本文對本院孕婦進行產前超聲檢查,分析產前超聲對胎兒動脈導管狹窄的診斷價值,結果顯示:在25~36孕周和孕周超過36周孕婦中,觀察組舒張期流速、收縮期流速等指標顯著高于對照組(P<0.05);而觀察組胎兒動脈導管內徑顯著低于對照組(P<0.05);在 25~36 周和超過 36周觀察組的動脈導管前向血流速度、三尖瓣反流速度及右心室壓力均顯著高于對照組,差異有統計學意義(P<0.05),與Patra等[20]的研究結果大體一致,在胎兒動脈導管的超聲檢查時,可通過分析“曲棍球桿狀”、“Z”形征、“V”形征及三指征等超聲特征,進而辨別動脈導管對其血流和形態狀態,更加全面、客觀地評估動脈導管;本研究結果顯示,觀察組在孕周25~36周和超過36周者動脈導管內徑均顯著低于對照組,說明超聲檢查可檢測動脈導管內徑進而判斷動脈導管狹窄;而舒張期流速和收縮期流速、動脈導管前向血流速度、三尖瓣反流速度均顯著高于正常對照組,說明可綜合評估動脈導管的血流參數、動脈導管的形態、內徑等指標,在評估動脈導管有無狹窄,臨床需結合動脈導管內是否出現高速血流、檢測內徑。胎兒循環中動脈導管起到十分重要的作用,如持續這種狀態,會引發胸腹水、胎兒水腫及右心室功能不全等情況。綜上所述,胎兒產前彩色多普勒超聲檢查可全面、客觀評估其影像特征,對診斷胎兒動脈導管狹窄具有重要的臨床價值。
[1]張家敏, 馬永紅, 沈艷, 等. 超聲心動圖對胎兒動脈導管狹窄及早閉的診斷[J]. 中國臨床醫學影像雜志, 2017, 28(3):204- 207.
[2]李玉燕. 3例超聲診斷晚孕期胎兒動脈導管狹窄的病例追蹤及討論[J]. 中國醫藥指南, 2016, 14(1): 197-198.
[3]陳慧明, 張麗范, 趙麗娟. 中孕中期胎兒動脈導管參考值范圍的建立及其對胎兒先天性心臟病的診斷價值[J]. 中國實用醫藥, 2015, 27(8): 13-15.
[4]繆偉, 代培峰, 黃進, 等. 動脈導管產前超聲心動圖表現異常在診斷先天性心臟病的價值[J]. 中國婦幼保健, 2015, 30(31):5433-5434.
[5]張燁, 何怡華, 孫琳, 等. 胎兒動脈導管血流頻譜與右室梗阻性疾病肺動脈發育相關分析[J]. 中國超聲醫學雜志, 2015,31(4): 355-357.
[6]高霞, 王海松, 張貴平, 等. 彩色多普勒超聲早期篩查胎兒先天性心臟病的臨床價值分析[J]. 中國婦幼保健, 2010, 25(18):153-156.
[7]代海燕, 王文韜, 田艾軍, 等. 產前超聲診斷胎兒動脈導管提前收縮或早閉的病例分析[J]. 中國婦幼保健, 2015, 30(30):5256-5257.
[8]郭寧, 王玲. 胎兒先天性心臟病超聲篩查的體會及高危因素分析[J]. 中國超聲醫學雜志, 2012, 28(12): 127-128.
[9]劉春陽, 劉宏曼, 馬麗. 彩色多普勒超聲診斷胎兒先天性心臟病的價值[J]. 中國婦幼保健, 2010, 25(25): 153-156.
[10]王宗英. 彩色多普勒超聲診斷在胎兒先天性心臟病中的臨床價值[J]. 中國當代醫藥, 2013, 20(26): 215-216.
[11]Haponiuk I, Paczkowski K, Chojnicki M, et al. Iatrogenic obstruction of the aorta - a sequence of delayed, fatal complications after 'off-label' interventional persistent ductus arteriosus closure[J]. Wideochir Inne Tech Maloinwazyjne, 2016, 11(1):44- 48.
[12]Laborda-Vidal P, Pedro B, Baker M, et al. Use of ECG-gated computed tomography, echocardiography and selective angiography in five dogs with pulmonic stenosis and one dog with pulmonic stenosis and aberrant coronary arteries[J]. J Vet Cardiol, 2016,18(4): 418-426.
[13]Ackerman JP, Smestad JA, Tester DJ, et al. Whole exome sequencing, familial genomic triangulation, and systems biology converge to identify a novel nonsense mutation in TAB2-encoded TGF-beta activated kinase 1 in a child with polyvalvular syndrome[J]. Congenit Heart Dis, 2016, 11(5): 452-461.
[14]Hayes DA. Constriction of the ductus arteriosus, severe right ventricular hypertension, and a right ventricular aneurysm in a fetus after maternal use of a topical treatment for striae gravidarum[J].Cardiol Young, 2016, 26(4): 796-798.
[15]Wei H, Mingxing X, Cheng TO, et al. The vital role the ductus arteriosus plays in the fetal diagnosis of congenital heart disease:evaluation by fetal echocardiography in combination with an innovative cardiovascular cast technology[J]. Int J Cardiol, 2016,202(1): 90-96.
[16]Datt V, Tempe DK, Lalwani P, et al. Perioperative management of a patient with Dandy Walker malformation with tetralogy of Fallot undergoing total correction and fresh homologous pericardial pulmonary valve conduit implantation: report of a rare case[J]. Ann Card Anaesth, 2015, 18(3): 433-436.
[17]Ratanasit N, Karaketklang K, Jakrapanichakul D, et al. Prenatal sonographic diagnosis of premature constriction of the fetal ductus arteriosus after maternal self-medication with benzydamine hydrochloride: report of 3 cases and review of the literature[J]. J Ultrasound Med, 2015, 34(3): 531-535.
[18]Van Middendorp LB, Maessen JG, Sardari Nia P. A patent ductus arteriosus complicating cardiopulmonary bypass for combined coronary artery bypass grafting and aortic valve replacement only discovered by computed tomography 3D reconstruction[J]. Interact Cardiovasc Thorac Surg, 2014, 19(6): 1071-1073.
[19]Ozyilmaz I, Ergul Y, Guzeltas A, et al. Possible link between right ventricular coronary sinusoids and noncompaction sinusoids in pulmonary atresia with intact ventricular septum patients that later develop left ventricular noncompaction[J]. Med Hypotheses, 2014,83(1): 53-55.
[20]Patra S, Kumar B, Sadananda KS, et al. Juvenile severe mitral stenosis predisposing Eisenmenger syndrome in a case with ventricular septal defect, patent ductus arteriosus, coarctation of aorta & hypoplastic aortic arch: report of first case of rare association[J]. J Cardiovasc Dis Res, 2013, 4(3): 195-197.
(張立芳 編輯)
Value of prenatal ultrasound in diagnosis of fetal ductus arteriosus stenosis
BAI Ming
(B Ultrasound Room, The First People's Hospital of Qingdao Economic and Technological Development Zone,Qingdao, Shandong 266555, China)
【Objective】To study the value of prenatal ultrasound in diagnosis of fetal ductus arteriosus stenosis.【Methods】Fifty cases of fetal ductus arteriosus stenosis diagnosed by prenatal color Doppler ultrasound in our hospital from January 2014 to April 2016 were selected as the observation group, and 50 healthy fetuses were selected by prenatal color Doppler ultrasound as the control group, the clinical indexes such as the diastolic fl ow velocity, the systolic fl ow velocity, and the diameter of the ductus arteriosus were compared between the two groups; the arterial velocity, the velocity of three cusp regurgitation, and the pressure of the right ventricle were compared between the two groups; the ultrasonic characteristics of the ductus arteriosus in different ultrasonic sections were observed.【Results】During the 25~36 week gestation and 36 week gestation, the diastolic fl ow velocity and systolic fl ow velocity of the observation group were signi fi cantly higher than those of the control group, and the differences were statistically signi fi cant(P<0.05); the diameter of fetal ductus arteriosus in the observation group was smaller than that in the control group, and the difference was statistically signi fi cant (P<0.05); at the 25~36 week of gestation and more than 36 weeks, the blood fl ow velocity, the three tricuspid regurgitation velocity and the right ventricular pressure in the observation group were signi fi cantly higher than those in the control group, and the differences were statistically signi fi cant (P<0.05).【Conclusion】Prenatal color Doppler ultrasonography can evaluate its imaging features comprehensively and objectively, and has important clinical value in the diagnosis of fetal ductus arteriosus stenosis.
fetal ductus arteriosus stenosis; color Doppler ultrasonography; clinical value
R714.5
A
10.19338/j.issn.1672-2019.2017.08.006
2017-05-18