不同封管方式預防血液透析導管相關并發癥的Meta分析
2018-06-05 06:31:34,,,
循證護理 2018年5期
,,,
目前,對于自身血管條件差、無法建立自體或移植動靜脈內瘺的血液透析病人將中心靜脈導管(central venous catheters,CVC)作為其血管通路的比例越來越高[1],有25%~50%的病人在CVC置入1年內就會發生導管功能失用[2];此外,CVC的置入與病人抗生素耐藥的發生、住院時間延長、醫療成本增加及其死亡率密切相關[3],這可能是與CVC導管功能障礙(catheter malfunction,CM)、導管相關感染,尤其是導管相關血流感染(catheter-related bloodstream infection,CRBI)的發生有關。美國CRBI的發生使病人平均住院日延長5 d~20 d,花費高達8 000~50 000美金[4],因此,在每次透析治療結束后,使用抗凝劑進行封管保持導管通暢,預防血栓形成,避免透析間期發生感染是目前公認的做法。已有研究證實,肝素封管與非肝素封管相比,可明顯降低導管阻塞、CRBI和導管微生物定植的發生風險[5-6]。但有研究發現,封管肝素從管腔內溢出會增加病人全身抗凝的危險性[1]。因此,探尋一種替代肝素封管的方式勢在必行。有研究探討使用枸櫞酸鹽封管在改善導管通暢性,減少CM發生方面的作用,結果顯示,使用枸櫞酸鹽封管可降低病人出血和CRBI的發生率[7-8],但在維持導管通暢性方面,枸櫞酸鹽封管和肝素封管的作用則沒有顯著差異。但也有學者研究發現,枸櫞酸鹽聯合抗生素封管可降低CRBI發生率及拔管率[9-10],而單純枸櫞酸鹽封管則無此療效。事實上,沒有一種封管方式可以同時降低CRBI和CM的發生率,因此,本研究擬通過Meta分析探索抗凝劑(肝素、枸櫞酸鹽)聯合或不聯合抗生素對血液透析病人CVC置管封管,在預防CRBI、出血等方面的作用。
1 資料與方法
1.1 納入標準和排除標準
1.1.1 納入標準
研究為前瞻性隨機對照試驗(RCT);對照組為單純肝素封管,試驗組為肝素聯合抗生素封管或肝素/其他抗凝劑聯合/不聯合抗生素;計算風險比率(RR)和95%置信區間(confidence interval,CI);隨訪時間大于30 d。
1.1.2 排除標準
CVC置管不用于血液透析;研究為回顧性研究或動物實驗、體外試驗。
1.2 檢索策略
2名研究者分別以“血液透析”“抗凝”和“導管”作為主題詞,檢索發表于Medline、EMbase、PubMed數據庫的研究。不限定發表時間,語言限定為英文。
1.3 結局指標
主要評價指標為CRBI發生率;次要評價指標為出血、導管出口感染(ESI)發生率。
1.4 數據提取
2名研究者分別獨立評估每項研究并記錄文獻質量及其納入、排除標準。數據提取內容包括病人基線水平、干預方式、病人數量、導管留置天數、隨訪時間以及其他可能影響研究結果的干預措施,并以Cochrane質量評價標準對文獻進行評估[11]。
1.5 統計學方法
采用Review Manger 5.0軟件進行統計分析,對照組和試驗組的二分類變量和連續變量分別采用RR和95%置信區間(confidence intenal,CI)的加權平均差表示。考慮到研究中固有的異質性,假設存在統計異質性,并使用隨機效應模型合并數據。測量結果的異質性使用Q檢驗,量化異質性用I2表示[11]。使用亞組分析探索異質性來源,并評估結果的靈敏度;使用漏斗圖檢測發表偏倚;以P<0.05為差異有統計學意義。
2 結果
2.1 文獻檢索結果
文獻檢索共檢索到224篇相關研究,經篩選共納入17項研究[8,10,12-26]進行系統綜述和Meta分析。文獻檢索流程圖見圖1。

圖1 文獻檢索流程圖
2.2 納入研究的基本特征
共納入17項研究[8,10,12-26]中所有研究的對照組均為單純肝素封管。納入研究的基本特征見表1,納入研究的方法學質量評價見表2。

表1 納入研究的基本特征

表2 納入研究的方法學質量評價
2.3 結果分析
2.3.1 CRBI
所有研究[8,10,12-26]均報道了CRBI的發生率,與單純肝素封管相比,聯合抗生素封管可顯著降低CRBI的發生率[OR=0.36,95%CI(0.28,0.46),P<0.001],見圖1。

圖1 CRBI發生率的Meta分析
2.3.2 出血
3項RCT研究[8,12,26]評價了出血的發生率。單純枸櫞酸鹽封管的病人,每個導管日任何類型出血的發生率均低于肝素封管的病人[OR=0.46,95%CI(0.30,0.72),P<0.001],異質性在可接受范圍,見圖2。但無證據表明,聯合抗生素封管可以降低出血事件的發生率,見圖3。

圖2 出血發生率的Meta分析

圖3 出血發生率的Meta分析
2.3.3 ESI發生率
10項RCT研究[8,12,14,16-18,20-21,23,26]描述了ESI的發生率,采用固定效應模型進行分析,單純枸櫞酸封管與肝素封管相比,[OR=0.54,95%CI(0.34,0.85),P=0.007];根據導管類型進行進一步亞組分析,NTCC組間OR值有顯著差異[OR=0.28,95%CI(0.12,0.68),P=0.005],TCC組間OR值無顯著差異[OR=0.73,95%CI(0.42,1.27),P=0.26]。由此可見,導管類型是異質性的來源,見圖4。聯合抗生素封管與單純肝素封管在降低ESI方面無顯著差異,見圖5。

圖4 ESI發生率的Meta分析
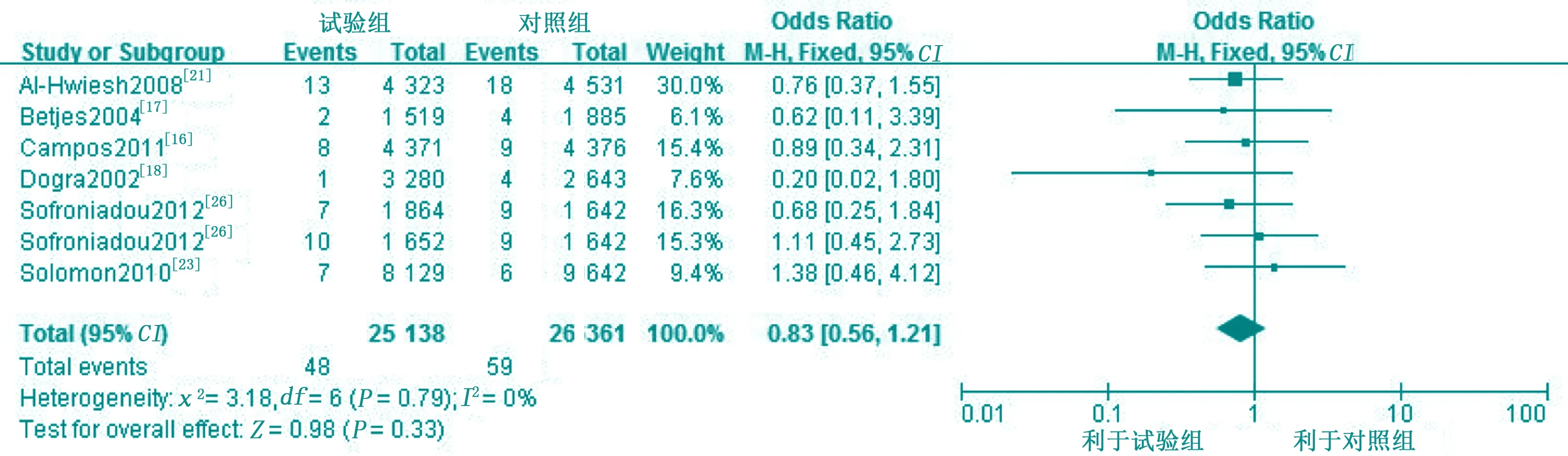
圖5 ESI發生率的Meta分析
2.4 發生偏倚分析
對納入研究不同封管方式對CRBI的發生率進行分析,結果見圖6。

圖6 CRBI發生率的漏斗圖
3 討論
盡管K/DOQI指南推薦使用自體動靜脈內瘺或移植動靜脈內瘺作為血液透析病人血管通路的首要選擇[27],但隨著老齡化和糖尿病、高血壓、肥胖等疾病人數不斷增加,CVC越來越廣泛地應用于血液透析病人中[28]。據相關統計資料顯示,全球每年新增CVC數量高達3百萬~4百萬[29];在美國的透析人群中,1/3的終末期病人選擇長期留置導管作為他們的血液透析通路。在中國經濟發達地區的血液凈化中心,至少有10%以上的病人選擇長期留置導管作為血管通路進行維持性血液透析治療。然而,長期使用CVC作為血液透析血管通路,其感染及血栓形成相關功能障礙的發生率較高[30],因此,我們迫切需要探索出有效的策略,以減少CVC相關并發癥發生率。使用肝素進行封管是避免CVC透析間期血栓形成的常規方法[20],但近年來,越來越多的學者指出,肝素從管腔中溢出會增加病人出血的風險[31],因此,許多新的封管方式不斷涌現,如聯合抗生素封管以降低CRBI的發生率及拔管率[9,32],但使用抗生素封管存在造成耐藥菌產生的風險,其安全性尚未得到證實,所以目前不推薦常規預防使用[4]。枸櫞酸鹽是迅速代謝、不引起全身出血的碳酸氫鹽[1],且具有一定的抗菌效果[33],聯合抗生素封管與單純枸櫞酸鹽封管可降低CRBI的發生率,這與之前的一些Meta分析結果相似[4,32,34],但單純枸櫞酸鹽封管的方式卻存在爭議,因此,還需進一步的RCT研究證實單純枸櫞酸鹽封管在預防CRBI發生率方面的作用。對于ESI的發生率,有1項RCT研究證實,枸櫞酸鹽封管可降低ESI的發生率[8]。然而,按照導管的不同類型進行亞組分析,發現枸櫞酸鹽封管并不是ESI發生的保護因素,這與之前的Meta分析結果有所不同[1]。單純枸櫞酸鹽封管可以降低出血的發生風險,這與以往研究結果一致[33]。另外,也有研究報道,高濃度的枸櫞酸鹽(46.7%)可引起心臟驟停,因此,美國食品和藥物管理局不推薦其作為導管封管液,它是否可以用于避免出血的發生也還需要大樣本RCT證實。
綜上所述,聯合抗生素或單純枸櫞酸鹽封管在降低CRBI、出血發生率方面的效果優于肝素,但其安全性還有待于進一步驗證。
參考文獻:
[1] Zhao Y,Li Z,Zhang L,etal.Citrate versus heparin lock for hemodialysis catheters:a systematic review and meta-analysis of randomized controlled trials[J].Am J Kidney Dis,2014,63(3):479-490.
[2] Firwana BM,Hasan R,Ferwana M,etal.Tissue plasminogen activator versus heparin for locking dialysis catheters:a systematic review[J].Avicenna J Med,2011,1(2):29-34.
[3] Safdar N,Maki DG.Use of vancomycin-containing lock or flush solutions for prevention of bloodstream infection associated with central venous access devices:a meta-analysis of prospective,randomized trials[J].Clin In-fect Dis,2006,43(4):474-484.
[4] O'grady NP,Alexander M,Dellinger EP,etal.Guidelines for the prevention of intravascular catheter-related infections[J].John Wiley & Sons,2002,52(9):e162-e193.
[5] Pettigrew M,Soltys GI,Bell RZ,etal.Tinzaparin reduces health care resource use for anticoagulation in hemodialysis[J].Hemodial Int,2011,15(2):273-279.
[6] Shah PS,Shah N.Heparin-bonded catheters for prolonging the patency of central venous catheters in children[J].Cochrane Database Syst Rev,2014,2(2):Cd005983.
[7] Grudzinski L,Quinan P,Kwok S,etal.Sodium citrate 4% locking solution for central venous dialysis catheters-an effective,more cost-efficient alternative to heparin[J].Nephrol Dial Transplant,2007,22(2):471-476.
[8] Weijmer MC,van den Dorpel MA,Van de Ven PJ,etal.Randomized,clinical trial comparison of trisodium citrate 30% and heparin as catheter-locking solution in hemodialysis patients[J].J Am Soc Nephrol,2005,16(9):2769-2777.
[9] Yahav D,Rozen-Zvi B,Gafter-Gvili A,etal.Antimicrobial lock solutions for the prevention of infections associated with intravascular catheters in patients un-dergoing hemodialysis:systematic review and meta-analysis of randomized,controlled trials[J].Clin Infect Dis,2008,47(1):83-93.
[10] Hemmelgarn BR,Moist LM,Lok CE,etal.Prevention of dialysis catheter malfunction with recombinant tissue plasminogen activator[J].N Engl J Med,2011,364(4):303-312.
[11] Higgins J,Green S.Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0[J].The Cochrane Collaboration,2011,5(2):S38.
[12] Macrae JM,Dojcinovic I,Djurdjev O,etal.Citrate 4% versus heparin and the reduction of thrombosis study (CHARTS)[J].Clin J Am Soc Nephrol,2008,3(2):369-374.
[13] Saxena AK,Panhotra BR,Sundaram DS,etal.Enhancing the survival of tunneled haemodialysis catheters using an antibiotic lock in the elderly:a randomised,double-blind clinical trial[J].Nephrology (Carlton),2006,11(4):299-305.
[14] Buturovic J,Ponikvar R,Kandus A,etal.Filling hemodialysis catheters in the interdialytic period:heparin versus citrate versus polygeline:a prospective randomized study[J].Artif Organs,1998,22(11):945-947.
[15] McIntyre CW,Hulme LJ,Taal M and Fluck RJ.Locking of tunneled hemodialysis catheters with gentamicin and heparin[J].Kidney Int,2004,66(2):801-805.
[16] Campos RP,Nascimento MM,Chula DC,etal.Minocycline-EDTA lock solution prevents catheter-related bacteremia in hemodialysis[J].J Am Soc Nephrol,2011,22(10):1939-1945.
[17] Betjes MG,Agteren M.Prevention of dialysis catheter-related sepsis with a citratetaurolidine-containing lock solution[J].Nephrol Dial Transplant,2004,19(6):1546-1551.
[18] Dogra GK,Herson H,Hutchison B,etal.Prevention of tunneled hemodialysis catheter-related infections using catheter-restricted filling with gentamicin and citrate:a randomized controlled study[J].J Am Soc Nephrol,2002,13(8):2133-2139.
[19] Kim SH,Song KI,Chang JW,etal.Prevention of uncuffed hemodialysis catheter-related bacteremia using an antibiotic lock technique:a prospective,randomized clinical trial[J].Kidney Int,2006,69(1):161-164.
[20] Power A,Duncan N,Singh SK,etal.Sodium citrate versus heparin catheter locks for cuffed central venous catheters:a single-center ran-domized controlled trial[J].Am J Kidney Dis,2009,53(6):1034-1041.
[21] Al-Hwiesh AK.Tunneled catheter-antibiotic lo-ck therapy for prevention of dialysis catheter-related infections:a single center experience[J].Saudi J Kidney Dis Transpl,2008,19(4):593-602.
[22] Maki DG,Ash SR,Winger RK,etal.A novel antimicrobial and antithrombotic lock solution for hemodialysis catheters:a multicenter,controlled,randomized trial[J].Crit Care Med,2011,39(4):613-620.
[23] Solomon LR,Cheesbrough JS,Ebah L,etal.A randomized double-blind controlled trial of taurolidinecitrate catheter locks for the prevention of bacteremia in patients treated with hemodialysis[J].Am J Kidney Dis,2010,55(6):1060-1068.
[24] Moran J,Sun S,Khababa I,etal.A randomized trial comparing gentamicin/citrate and heparin locks for cen-tral venous catheters in maintenance hemodialysis patients[J].Am J Kidney Dis,2012,59(1):102-107.
[25] Nori US,Manoharan A,Yee J and Besarab A.Comparison of low-dose gentamicin with minocycline as catheter lock solutions in the pre-vention of catheter-related bacteremia[J].Am J Kidney Dis,2006,48(4):596-605.
[26] Sofroniadou S,Revela I,Smirloglou D,etal.Linezolid versus vancomycin antibiotic lock solution for the preven-tion of nontunneled catheter-related blood stream infections in hemodialysis patients:a prospective randomized study[J].Semin Dial,2012,25(3):344-350.
[27] National Kidney Foundation.K/DOQI Clinical Practice Guidelines for Vascular Access[J].Am J Kidney Dis,2006,48(suppl 1):S176-S322.
[28] Mandolfo S,Acconcia P,Bucci R,etal.Hemodialysis tunneled central venous catheters:five-year outcome analysis[J].J Vasc Access,2014,15(6):461-465.
[29] Causes of deaht:USRDS:United States Renal Data System[J].AmJ KidneyDis,1997,30(2Suppl ):5107-511.
[30] Van Der Meersch H,De BD,Vandecasteele SJ,etal.Catheter Design and Catheter Performance:A Randomized Controlled Trial[J].Am J Kidney Dis,2014,64(6):902-908.
[31] Mandolfo S.Central venous catheter lock to prevent thrombosis and bacterial infection[J].G Ital Nefrol,2012,29(3):301-307.
[32] Snaterse M,Ruger W,Lucas C,etal.Antibiotic-based catheter lock solutions for prevention of catheter-related bloodstream infection:a systematic review of randomised controlled trials[J].J Hosp Infect,2010,75(1):1-11.
[33] Pierce DA,Rocco MV.Trisodium citrate:an al-ternative to unfractionated heparin for hemodialysis catheter dwells[J].Pharmacotherapy,2010,30(11):1150-1158.
[34] Moore CL,Besarab A,Ajluni M,etal.Comparative effectiveness of two catheter locking solutions to reduce catheter-related bloodstream infection in hemodialysis patients[J].Clin J Am Soc Nephrol,2014,9(7):1232-1239.
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
天津外國語大學學報(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
科技傳播(2019年22期)2020-01-14 03:06:54
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
電子制作(2018年18期)2018-11-14 01:48:24
汽車工程學報(2017年2期)2017-07-05 08:13:02
山東工業技術(2016年15期)2016-12-01 05:31:22
中國中醫藥現代遠程教育(2014年11期)2014-08-08 13:23:44