利培酮對阿爾茨海默病患者吞咽障礙影響的研究
2019-09-29 06:54:17申永輝陳致宇陳斌華丁雯雯張學平
中國現代醫生 2019年21期
申永輝 陳致宇 陳斌華 丁雯雯 張學平
[摘要] 目的 探索非典型抗精神病藥物利培酮對阿爾茨海默病患者吞咽障礙的影響。 方法 納入2017年1~12月期間我院治療的阿爾茨海默病患者102例。根據癡呆病理行為評定量表(BEHAVE-AD)評定患者精神行為癥狀(behavioral and psychological symptoms of dementia,BPSD)的嚴重程度,BEHAVE-AD<20分納入對照組,BEHAVE-AD≥20分納入治療組。對照組使用多奈哌齊治療;治療組在多奈哌齊改善認知基礎上聯合使用利培酮治療,在BPSD控制后逐步減量利培酮,治療滿3個月時利培酮完全減停。兩組在治療前、治療3個月、6個月后分別采用洼田飲水試驗評估吞咽功能。 結果 治療3個月后治療組洼田飲水試驗評分較對照組顯著上升,兩組差異具有統計學意義(t=6.925,P<0.01);兩組治療前及治療6個月后的洼田飲水試驗評分比較差異無統計學意義(t=1.200,P>0.05);對照組、治療組洼田飲水試驗評分組內兩兩比較,組內差異均有統計學意義(F=169.651,P=0.001)、(F=75.356,P=0.001),其中對照組組內治療3個月、6個月后差異無統計學意義(P>0.05)。 結論 多奈哌齊可改善阿爾茨海默病患者的吞咽障礙,但長期使用對吞咽障礙的改善作用有限;利培酮可加重阿爾茨海默病患者吞咽障礙的嚴重程度,但及時停用利培酮,對阿爾茨海默病患者吞咽障礙的影響可恢復。
[關鍵詞] 阿爾茨海默病;吞咽障礙;多奈哌齊;利培酮
[中圖分類號] R749.1+6? ? ? ? ? [文獻標識碼] B? ? ? ? ? [文章編號] 1673-9701(2019)21-0102-04
Effect of risperidone on dysphagia in patients with Alzheimer's disease
SHEN Yonghui1 CHEN Zhiyu2 CHEN Binhua3 DING Wenwen3 ZHANG Xueping3
1.Ward 2nd,Department of Psychosomatic,Hangzhou Seventh People's Hospital,Mental Health Center Zhejiang University School of Medicine,Hangzhou? ?310013,China;2.Department of Psychiatry,Hangzhou Seventh People's Hospital,Mental Health Center Zhejiang University School of Medicine,Hangzhou? ?310013,China;3.Department of Geriatric Psychiatry,Hangzhou Seventh People's Hospital,Mental Health Center Zhejiang University School of Medicine,Hangzhou? ?310013,China
[Abstract] Objective Explore the effects of atypical antipsychotic drug risperidone on dysphagia in patients with Alzheimer's disease. Methods 102 patients with Alzheimer's disease who were admitted to our hospital from January to December 2017 were included. According to the dementia pathological behavior rating scale(BEHAVE-AD), the severity of behavioral and psychological symptoms of dementia(BPSD) was assessed. Patients with BEHAVE-AD<20 was included in the control group, and those with BEHAVE-AD≥20 was included in the treatment group. The control group was treated with donepezil; the treatment group was treated with risperidone on the basis of improved knowledge of donepezil, and risperidone was gradually reduced after BPSD control, and risperidone was completely reduced after 3 months of treatment. The swallowing function was evaluated by the Watian drinking water test before treatment, and after 3 months and 6 months of treatment. Results After 3 months of treatment, the score of the Watian drinking water test in the treatment group was significantly higher than that in the control group. The difference between the two groups was statistically significant(t=6.925, P<0.01). The differences in the scores of the Watian drinking water test before treatment and after 6 months of treatment were not significant(t=1.200, P>0.05). There were significant intra-group differences in the control group and the treatment group in the Watian drinking water test scores(F=169.651, P=0.001), (F=75.356, P=0.001), and there was no significant difference in the control group after 3 months and 6 months of treatment(P>0.05). Conclusion Donepezil improves dysphagia in patients with Alzheimer's disease, but long-term use has limited improvement in dysphagia; risperidone can aggravate the severity of dysphagia in patients with Alzheimer's disease, but if discontinued in time, the effect on dysphagia in Alzheimer's disease patients can be restored.
[Key words] Alzheimer's disease; Dysphagia; Donepezil; Risperidone
吞咽障礙是阿爾茨海默病的常見癥狀,是預后的不良因素,國外研究顯示,一半以上癡呆患者有不同程度的吞咽障礙[1]。吞咽障礙增加誤吸風險,進而導致肺炎,嚴重時甚至死亡[2]。肺炎是癡呆患者死亡的首位原因[3]。多奈哌齊是臨床上改善輕中度癡呆認知功能的首選藥物;利培酮多做為抗精神病藥物控制癡呆患者的BPSD而廣泛使用[4]。在使用抗精神病藥物治療的同時不可避免的會出現錐體外系副反應,而吞咽障礙是在老年癡呆人群中常見的副反應之一。抗精神病藥物可引起咽喉肌群功能失調,發生吞咽困難,導致嗆咳或噎食,是危及患者生命安全的原因之一[5]。本研究探討非典型抗精神病藥利培酮對阿爾茨海默病患者吞咽障礙的影響,為優化臨床治療提供參考依據。
1 對象與方法
1.1 研究對象
選取我院在2017年1~12月期間接受住院治療的阿爾茨海默病患者,同時存在吞咽障礙。納入標準:①阿爾茨海默病符合《疾病和有關健康問題的國際統計分類第十版》(The international statistical classification of diseases and related health problems 10th revision,ICD-10)的診斷標準[6],癡呆嚴重程度為輕到中度,由2位主治及以上職稱的精神科醫師診斷;②存在洼田飲水試驗評定有3~5分的吞咽障礙;③既往未曾使用過改善認知藥物及抗精神病藥物;④意識清楚,生命體征平穩,對基本要求指令能理解并配合。排除標準:①合并有其他可能影響吞咽功能的疾病,如腦卒中、頭頸部腫瘤、食道腫瘤、顱腦損傷、重癥肌無力、格林-巴利綜合征等;②入院前已發生肺部感染者或重要器官功能衰竭者;③拒食、拒水等帶鼻飼入院者。共納入102例患者。
采用癡呆病理行為評定量表(BEHAVE-AD)評定患者BPSD的嚴重程度[7],BEHAVE-AD≥20分納入治療組,BEHAVE-AD<20分納入對照組。簡易智力狀態檢查量表(MMSE)評估患者癡呆嚴重程度。
本研究程序和內容符合杭州第七人民醫院倫理委員會所制定的倫理學標準,研究開展前已經獲得該倫理委員會的審查和批準。全部研究被試及其監護人對本研究項目知情,均已簽署知情同意書。
1.2 治療方法
兩組均使用多奈哌齊改善認知功能;治療組聯合使用非典型抗精神病藥利培酮控制患者的BPSD。多奈哌齊片(蘇州衛材制藥有限公司,5 mg/片,生產批號1603044、1607021)5 mg/d為起始治療劑量,治療4周后可根據情況調整劑量至10 mg/d。利培酮片(西安楊森制藥有限公司,1 mg/片,生產批號161009236、170206384)0.5 mg/d 起始劑量治療,依據患者的病情調整用藥劑量至1~4 mg/d;控制BPSD后漸減利培酮,至使用3個月時完全停用。
1.3 判斷標準
洼田飲水試驗在臨床吞咽障礙診斷中可作為吞咽障礙的診斷工具[8]。兩組在治療前及治療3個月、6個月后采用洼田飲水試驗評估患者的吞咽功能。洼田飲水試驗實施流程:患者取坐位,要求在5 s內喝下30 mL的溫開水,注意觀察記錄喝水所需時間、喝水次數及發生嗆咳情況。試驗結果評定標準:在5 s內喝下30 mL溫開水且1次咽下,記1分;在5 s內喝下30 mL溫開水并分2次咽下,記2分;在5 s內喝下30 mL溫開水且1次咽下,有出現嗆咳,記3分;在5 s內喝下30 mL溫開水但分1次以上咽下,有出現嗆咳,記4分;在5 s內難以喝完30 mL溫開水,頻繁出現嗆咳,記5分。
1.4 統計學方法
數據采用IBM SPSS Statistics 20.0進行統計分析。本研究資料近似服從正態分布,性別為計數型資料比較采用χ2檢驗;年齡、病程、MMSE評分、洼田飲水試驗評分為計量型資料采用均數±標準差(x±s)描述,組間均數分析運用兩獨立樣本t檢驗;組內均數分析使用Bonfferoni t檢驗進行兩兩比較。統計檢驗均為雙側檢驗,檢驗水準α=0.05。P<0.05為差異有統計學意義。
2 結果
2.1 兩組一般資料比較
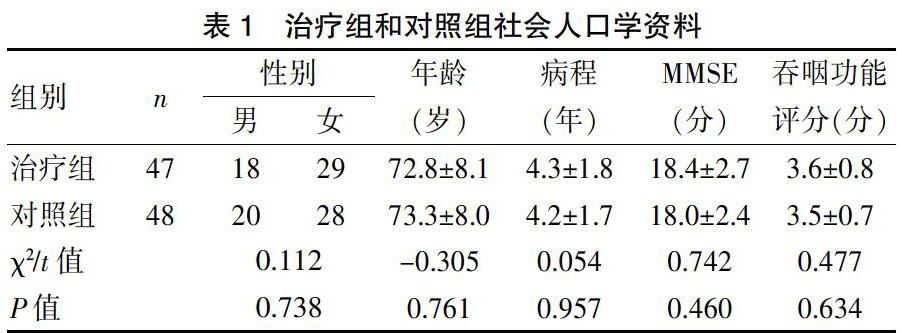
共入組患者102例。治療組54例,其中因不耐受利培酮所致錐體外系等副反應排除7例,47例完成本研究,其中男18例,女29例;對照組48例,其中男20例,女28例。兩組性別(χ2=0.112,P=0.738)、年齡(t=-0.305,P=0.761)、病程(t=0.054,P=0.957)、MMSE評分(t=0.742,P=0.460)等一般資料及治療前洼田飲水試驗評分(t=0.477,P=0.634)比較,差異無統計學意義(P>0.05)。見表1。
2.2 兩組吞咽功能評分比較
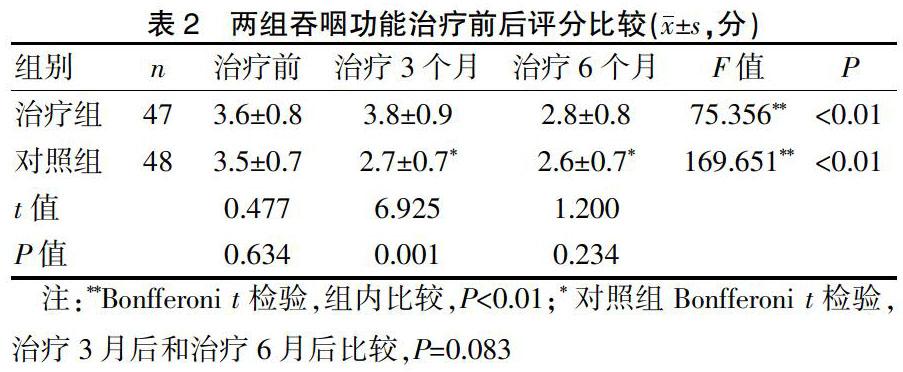
兩組組間進行兩獨立樣本t檢驗,治療3個月后治療組洼田飲水試驗評分較對照組顯著上升,差異有統計學意義(P<0.05);治療前及治療6個月后兩組的洼田飲水試驗評分差異均無統計學意義(P>0.05)。兩組組內進行Bonfferoni t檢驗以兩兩比較,治療前后差異具有統計學意義(P<0.01);其中對照組治療3個月后和治療6個月后比較,差異無統計學意義(P>0.05)。見表2。
3 討論
約75%阿爾茨海默病患者咽喉部肌群具有吞咽困難的電生理特征,輕度或中度的阿爾茨海默病患者也可能出現吞咽困難的亞臨床癥狀[9]。阿爾茨海默病患者的吞咽障礙持續時間長且康復困難,持續的吞咽障礙勢必嚴重影響患者的生存質量和生活體驗。尤其是吞咽障礙所致的噎食、誤吸、營養不良、肺部感染等也是臨床上癡呆患者預后死亡的主要危險因素[10-11]。故而對癡呆患者的吞咽障礙進行積極有效的干預,一直被臨床醫生所重視。因抗精神病藥物對吞咽功能有一定影響,有必要評估其對癡呆患者吞咽功能的影響程度。Abdelhamid A等[12]納入43項研究的薈萃分析指出,對有吞咽困難的癡呆患者目前尚沒有發現有確切證據的特定干預措施。盡管缺乏有效干預措施,癡呆患者及其照顧者仍亟需解決進食問題,積極的預防和改善吞咽障礙,能顯著改善患者營養狀態,提高抵抗力,降低吸入性肺炎發生率及感染所致死亡率等,有利于提高患者的生存質量,減輕照料者負擔。
超過90%的癡呆患者會出現不同程度的BPSD,如攻擊行為、易激惹、妄想、行為脫抑制、情緒不穩定等,嚴重的BPSD是護理人員和照料者日常生活中所面對的主要挑戰和最大壓力因素[13-14]。控制癡呆患者的BPSD,是治療需解決的首要問題之一。Jin B等[15]納入146例研究的Meta分析指出利培酮、阿立哌唑、氟哌啶醇和喹硫平等抗精神病藥物應該是治療BPSD的首選,且其安全性被認為是可接受的。國際老年精神病協會共識指出,對伴有BPSD癡呆患者的藥物選擇中,評估潛在風險后應優先考慮使用利培酮治療[16]。目前在臨床上使用非典型抗精神病藥控制BPSD已較為普遍,但需關注的是,有多項研究表明,長期使用非典型抗精神病藥會增加癡呆患者嚴重不良事件的高風險和死亡率[17-19]。但也有研究[20]表明,在臨床中權衡利弊使用非典型抗精神病藥物,可減少伴有BPSD癡呆患者的死亡率。故而本研究也在控制癡呆患者BPSD后漸減停利培酮治療。
本研究發現,與對照組相比較使用利培酮治療3個月會加重癡呆患者的吞咽障礙,洼田飲水試驗評分差異有統計學意義。與以往研究一致,有納入36項研究的薈萃分析[21]認為,抗精神病藥可增加吞咽障礙患病率。因吞咽障礙對癡呆患者預后影響巨大,有必要進一步評估停用利培酮后癡呆患者吞咽功能受到的影響是否仍持續。本研究進一步發現,控制BPSD后及時停用利培酮,治療6個月時患者的吞咽功能較對照組洼田飲水試驗評分差異無統計學意義。與Miarons M等[22]研究結果一致,該研究對114例癡呆患者運用金標準電視熒光檢查評估吞咽功能,發現使用抗精神病藥物治療沒有顯著惡化患者的吞咽障礙。但老年人群服用抗精神病藥物更易出現錐體外系不良反應,并且因藥物抗膽堿作用影響咽喉部環狀括約肌的正常運動,導致咽喉部肌群運動共濟失調,這可能是抗精神病藥物導致吞咽障礙的主要原因。提示我們在臨床工作中,盡量減少抗精神病藥物的使用時間,進而減少抗精神病藥對吞咽功能可能造成的不良影響。
同時,本研究發現對照組使用多奈哌齊改善癡呆患者認知功能,治療3個月、6個月時洼田飲水試驗評分均較治療前下降且差異有統計學意義;但組內分析顯示治療3個月、6個月比較洼田飲水試驗評分差異無統計學意義。表明改善癡呆患者認知功能對吞咽障礙的改善有益,但長期服用多奈哌齊可能對癡呆患者吞咽障礙的益處是有限的,這與國內田閃等[23]、王愛霞等[24]研究相一致。
本研究探討了以利培酮為代表的非典型抗精神病藥對癡呆患者吞咽障礙的影響,但也存在一定的缺陷,使用洼田飲水試驗評估患者的吞咽功能雖然操作簡便易于實施,但遠不如金標準電視熒光檢查的精確,同時本研究樣本量較小,采用方便取樣的方法選取被試,取樣范圍有限,可能研究結果不具備代表性。未來可進一步完善抽樣方法和吞咽功能評估方法。
[參考文獻]
[1] Alagiakrishnan K,Bhanji RA,Kurian M. Evaluation and management of oropharyngeal dysphagia in different types of dementia:A systematic review[J]. Archives of Gerontology & Geriatrics,2013,56(1):1-9.
[2] Puisieux F,D'Andrea C,Baconnier P,et al. Swallowing disorders,pneumonia and respiratory tract infectious disease in the elderly[J]. Revue Des Maladies Respiratoires, 2011,28(8):e76-93.
[3] 胡瀟云,龍盛雙,邱隆敏,等.阿爾茲海默病患者醫院感染危險因素的Meta分析[J]. 中華醫院感染學雜志,2017, 27(8):1780-1784.
[4] Mcneal KM,Meyer RP,Lukacs K,et al. Using risperidone for Alzheimer's dementia-associated psychosis[J]. Expert Opinion on Pharmacotherapy,2008,9(14):2537-43.
[5] 沈漁邨.精神病學[M].第5版. 北京:人民衛生出版社,2009:964.
[6] 世界衛生組織.ICD-10精神與行為障礙分類[M]. 范肖冬,汪向東,于欣,等.北京:人民衛生出版社,1993:41-44.
[7] 張明園,何燕玲.精神科評定量表手冊[M]. 長沙:湖南科學技術出版社,2016:292-293.
[8] 武文娟,畢霞,宋磊,等.洼田飲水試驗在急性腦卒中后吞咽障礙患者中的應用價值[J]. 上海交通大學學報(醫學版),2016,36(7):1049-1053.
[9] Se?觭il Y,Ar?覦c?覦 S,Incesu TK,et al. Dysphagia in Alzheimer's disease[J]. Neurophysiol Clin,2016,46(3):171-178.
[10] Hessler JB,Sch?覿ufele M,Hendlmeier I,et al. Behavioural and psychological symptoms in general hospital patients with dementia,distress for nursing staff and complications in care:Results of the General Hospital Study[J]. Epidemiol Psychiatr Sci,2018,27(3): 278-287.
[11] Houttekier D,Reyniers T,Deliens L,et al. Dying in hospital with dementia and pneumonia:A nationwide study using death certificate data[J]. Gerontology,2014,60(1):31.
[12] Abdelhamid A,Bunn D,Copley M,et al. Effectiveness of interventions to directly support food and drink intake in people with dementia:Systematic review and Meta-analysis[J]. BMC Geriatr,2016:16-26.
[13] Kratz T. The diagnosis and treatment of behavioral disorders in dementia[J]. Dtsch Arztebl Int,2017,114(26): 447-454.
[14] Arthur PB,Gitlin LN,Kairalla JA,et al. Relationship between the number of behavioral symptoms in dementia and caregiver distress:What is the tipping point[J]. Int Psychogeriatr,2018,30(8):1099-1107.
[15] Jin B,Liu H. Comparative efficacy and safety of therapy for the behavioral and psychological symptoms of dementia:A systemic review and Bayesian network meta-analysis[J]. J Neurol,2019,266(1):680-690.
[16] Kales HC,Lyketsos CG,Miller EM,et al. Management of behavioral and psychological symptoms in people with Alzheimer's disease:An international Delphi consensus[J].Int Psychogeriatr,2019,31(1):83-90.
[17] Sturm AS,Trinkley KE,Porter K,et al. Efficacy and safety of atypical antipsychotics for behavioral symptoms of dementia among patients residing in long-term care[J]. Int J Clin Pharm,2018,40(1):135-142.
[18] Freund-Levi Y,Bloniecki V,Auestad B,et al. Galantamine versus risperidone for agitation in people with dementia:A randomized,twelve-week,single-center study[J].Dementia & Geriatric Cognitive Disorders,2014,38(3-4):234-244.
[19] Dyer SM,Harrison SL,Laver K,et al. An overview of systematic reviews of pharmacological and non-pharmacological interventions for the treatment of behavioral and psychological symptoms of dementia[J]. Int Psychogeriatr,2018,30(3):295-309.
[20] Howard R,Costafreda SG,Karcher K,et al. Baseline characteristics and treatment-emergent risk factors associated with cerebrovascular event and death with risperidone in dementia patients[J]. British Journal of Psychiatry the Journal of Mental Science,2016,209(5):378.
[21] Miarons M,Rofes L. Systematic review of case reports of oropharyngeal dysphagia following the use of antipsychotics[J]. Gastroenterol Hepatol,2018,11(8):532-535.
[22] Miarons M,Clavé P,Wijngaard R,et al. Pathophysiology of oropharyngeal dysphagia assessed by videofluoroscopy in patients with dementia taking antipsychotics[J]. J Am Med Dir Assoc,2018,19(9): 812.e1-812.e10.
[23] 田閃,徐邵紅,胡瑞萍,等.認知功能訓練對腦損傷后吞咽功能障礙并發認知功能障礙患者吞咽功能改善程度的影響[J]. 上海醫藥,2017,38(13):17-21.
[24] 王愛霞,唐起嵐,郭麗娜,等.心理及認知行為干預對腦卒中吞咽障礙患者功能恢復的影響[J]. 中國實用神經疾病雜志,2018,21(12):1373-1378.