上海某社區甲狀腺結節人群隨訪結果分析
2020-12-10 06:49:59魯青夏建兵陳海英金志萍
上海醫藥 2020年22期
魯青 夏建兵 陳海英 金志萍

摘 要 目的:通過對甲狀腺結節患者的隨訪,評估甲狀腺結節大小、性質的變化。方法:在社區451名常住居民中經甲狀腺超聲檢測發現375例甲狀腺結節患者,其中男性142例,平均年齡(65.3±8.1)歲,女性233例,平均年齡(62.8±8.3)歲。每年進行隨訪,為期3年。觀察甲狀腺結節的個數、結節大小以及對結節性質的初步判斷。結果:在隨訪的3年中,在初次評估的375例甲狀腺結節患者的977個甲狀腺結節中,發現結節體積有增長的180個,占18.61%。有35例(9.33%)出現新增結節,有6例(1.60%)因發現甲狀腺惡性腫瘤而進行了手術治療。多元logistic回歸分析顯示,BMI、懷孕次數(女性)、腦力工作者與甲狀腺結節體積增長有關(P<0.05)。結論:大多數甲狀腺結節在3年隨訪期間基本保持結節體積及性質的穩定,并不會對甲狀腺結節患者人群的正常生活帶來影響。
關鍵詞 甲狀腺結節;社區;隨訪
中圖分類號:R736.1 文獻標志碼:A 文章編號:1006-1533(2020)22-0039-04
Analysis of follow-up results of thyroid nodule population in a community in Shanghai
LU Qing1, XIA Jianbing2, CHEN Haiying1, JIN Zhiping3**(1. General Practice Department of Fengpu Community Health Service Center of Fengxian District, Shanghai 201401, China; 2. General Surgery Department of Fengcheng Hospital, Fengxian District, Shanghai 201411, China; 3. General Practice Department of Nanqiao Community Health Service Center of Fengxian District, Shanghai 201499, China)
ABSTRACT Objective: By following up patients with thyroid nodules, to evaluate the size and nature of thyroid nodules. Methods: Among 451 permanent residents in the community, 375 patients with thyroid nodules were detected by thyroid ultrasound, there were 142 males with an average age of (65.3 ± 8.1) years and 233 females with an average age of (62.8 ±8.3) years. The patients were followed up every year for 3 years. The number and size of thyroid nodules and the preliminary determination of the nature of nodules were observed. Results: During the 3 years of follow-up, among the 977 thyroid nodules in 375 patients with thyroid nodules in the initial evaluation, 180 nodules were found to have increased in volume, accounting for 18.61%. There were 35 cases (9.33%) with new nodules, and 6 cases (1.60%) underwent surgical treatment due to the discovery of thyroid malignant tumor. Multivariate logistic regression analysis showed that BMI, number of pregnancies (female), and mental workers were related to the increase in the volume of thyroid nodules (P <0.05). Conclusion: Most thyroid nodules remain stable in volume and nature during the 3-year follow-up period, and would not affect the normal life of thyroid nodules patients.
KEY WORDS thyroid nodule; community; follow-up
近年來,甲狀腺結節的發病率持續上升。人群中甲狀腺結節患病率可達到50%~80%左右,這一趨勢可能與甲狀腺超聲檢查分辨率及檢查者水平的提高有關[1-3]。這一現象給甲狀腺結節患者帶來一定心理壓力。社區層面對甲狀腺疾病的管理未引起足夠重視,多數甲狀腺結節患者有一定恐慌情緒。但根據文獻報道,絕大多數甲狀腺結節為良性結節,對于人體影響甚小[4-6]。本研究旨在通過社區甲狀腺結節患者的動態隨訪,觀察甲狀腺結節大小、性質的變化,以及影響甲狀腺結節大小發生變化的相關因素,為甲狀腺結節患者的隨訪管理提供依據。
1 對象與方法
1.1 對象
從2015年9月1日起在上海奉賢區西渡、奉浦兩個社區任選8個村(居)委中共451名常住居民,通過甲狀腺超聲檢查檢出375名甲狀腺結節患者。對375名甲狀腺結節患者每年隨訪復查一次,至2018年9月結束。在超聲評估前檢查血甲狀腺功能指標,排除甲狀腺功能異常者。
375例甲狀腺結節患者的平均年齡(63.8±8.3)歲。其中男性142例,平均年齡(65.3±8.1)歲,女性233例,平均年齡(62.8±8.3)歲。
1.2 方法
甲狀腺超聲檢查固定由3名甲狀腺超聲醫生按照統一標準對甲狀腺結節進行評估。檢查采用多普勒超聲,淺表部位采用12 MHz探頭,深部組織采用7.5~10 MHz探頭。超聲檢查者仔細測量并記錄每個結節水平徑、前后徑及上下徑。并且觀察每個結節的內部情況(實性、海綿狀、囊性、混合性),回聲情況,結節邊界情況以及結節周圍血流情況等超聲特征,并進行描述性統計[7]。若出現低回聲,不規則邊界,結節長徑大于寬徑,點狀鈣化,結節內點狀血流等超聲征象,則懷疑甲狀腺結節性質問題,需轉診至上級醫院進一步明確結節性質。甲狀腺結節大小變化,采用甲狀腺結節體積(三徑相乘)變化超過50%來確定[8]。
1.3 統計學方法
采用SPSS 15.0軟件進行統計分析。計數資料用百分率(%)表示,比較采用χ2檢驗。使用logistic回歸方法分析影響甲狀腺結節體積增長的相關因素。P<0.05為差異有統計學意義。
2 結果
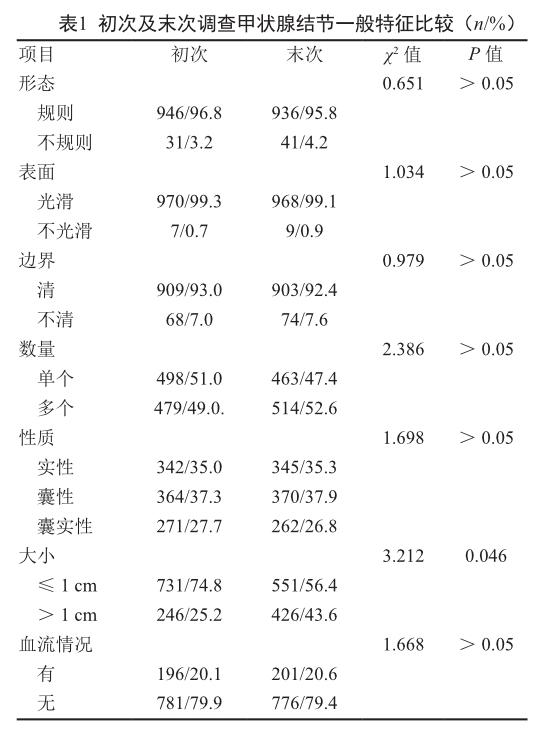
2.1 初次及末次調查甲狀腺結節一般特征
初次評估甲狀腺結節為977個,在隨訪過程中,發現體積增長的結節為180個,占所有結節的18.61%。有35人出現新增結節,占9.33%。有6人發現甲狀腺惡性腫瘤,占1.60%,均進行了手術治療。
大多數甲狀腺結節形態規則,表面光滑,邊界清楚。而對于結節性質來說,結節實性,囊性,囊實性各占約 1/3。在初次及末次調查甲狀腺結節特征中發現,直徑>1 cm的結節數量隨著時間的推移出現增長,直徑≤1cm的結節數量減少,差異有統計學意義(P<0.05)。見表1。
2.2 影響甲狀腺結節體積增長的單因素分析
甲狀腺結節體積增長與年齡、體重指數(BMI)、懷孕次數、職業、吸煙史、食海帶類、食用加碘鹽有關(P<0.05);與性別、飲酒史無關(P>0.05)。見表2。
2.3 影響甲狀腺結節體積增長的多因素分析
以有無甲狀腺結節體積增長為因變量,以年齡,BMI,懷孕次數(女性),職業,食用加碘鹽,食海帶類,吸煙史(男)為自變量進行多元logistic回歸分析。結果顯示,BMI、懷孕次數(女性)、腦力工作者與甲狀腺結節體積增長相關(P<0.05);年齡、食用海帶類、使用加碘鹽、吸煙史與甲狀腺結節體積增長無關(P>0.05)。見表3。
3 討論
雖甲狀腺結節患者日益增多,但尚未有直接證據證明何種因素與甲狀腺結節發生密切相關;同時甲狀腺結節如何發展,如何轉歸也是一個臨床空白[9-10]。
本研究發現,BMI增高是甲狀腺結節體積發生增大的危險因素之一。相關文獻也有同樣報道,這可能與人體內脂肪代謝,同時出現胰島素抵抗現象,影響了下丘腦-垂體激素軸,促使甲狀腺結節發生及生長有關[11-13]。本次研究發現,缺少體力活動(腦力工作者)的人群比較容易出現甲狀腺結節體積增長的情況。這可能與工作壓力大、長期處于精神緊張狀態,易導致失眠、焦慮、免疫力下降和內分泌紊亂等因素有關。本研究還顯示,女性懷孕次數的增加也是甲狀腺結節體積增大的危險因素,這可能是懷孕次數的增加影響人體激素代謝的改變,與甲狀腺激素之間存在一定相關性。普遍認為碘攝入可能是甲狀腺結節發生及發展的重要環境因素,但本研究顯示食海帶類及攝入含碘鹽與甲狀腺結節的體積增大無明顯相關性,這可能與本次研究對象的人體差異、樣本量有限等因素有關。以往臨床經驗都認為,甲狀腺結節體積會隨著時間的推移而逐漸增長[14-15]。有作者認為大多數甲狀腺結節體積會增長(39%~61.2%),但另一些研究卻認為大多數甲狀腺結節大小會保持穩定,甚至結節會縮小、消失[16-18]。這可能與既往研究絕大多數為回顧性研究有關。其次對于結節體積變化并沒有統一標準,從而使得研究結果可能會出現較大的誤差,得出并不一致的研究結果。目前廣泛接受的是甲狀腺結節體積大小發生50%的變化,這一變化衡量標準也被美國甲狀腺協會指南所推薦[19, 7]。本次研究發現社區僅18.61%的甲狀腺結節出現增大情況。因此,大多數的甲狀腺結節還是相對穩定,沒有必要引起過度的恐慌和臨床干預。同時,基于超聲診斷的良性甲狀腺結節在一定隨訪期內大小變化相對穩定,對該人群可采取長期隨訪和相對保守的臨床策略。
本研究存在一些不足。首先本研究為單中心研究,研究對象對總體的代表性相對有限;其次,所有結節的良惡性判斷基于超聲結果,可能存在數據測量結果的偏倚;第三,隨訪時間相對較短,樣本量相對較小。要進一步證實以上結論還需有更大樣本的多中心的隊列研究來支持。
參考文獻
[1] Davies L, Ouellette M, Hunter M, et al. The increasing incidence of small thyroid cancers: where are the cases coming from?[J]. Laryngoscope, 2010, 120(12): 2446-2451.
[2] Sosa JA, Hanna JW, Robinson KA, et al. Increases in thyroid nodule fine-needle aspirations, operations, and diagnoses of thyroid cancer in the United States[J]. Surgery. 2013, 154(6): 1420-1426.
[3] Smith-Bindman R, Lebda P, Feldstein VA, et al. Risk of thyroid cancer based on thyroid ultrasound imaging characteristics: results of a population-based study[J]. JAMA Intern Med, 2013, 173(19): 1788-1796.
[4] 中華醫學會內分泌學分會, 中華醫學會外科學分會, 中國抗癌協會頭頸腫瘤專業委員會, 等. 甲狀腺結節和分化型甲狀腺癌診治指南[J]. 中國腫瘤臨床, 2012, 39(17): 1249-1272.
[5] Mandel SJ. Diagnostic use of ultrasonography inpatients with nodular thyroid disease[J]. Endocr Pract. 2004, 10(3): 246-252.
[6] Gharib H, Papini E, Paschke R, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association Medical Guidelines for Clinical Practice for the Diagnosis and Management of Thyroid Nodules[J]. Endocr Pract, 2010, 16(suppl 1): 1-43.
[7] Knudsen N, Bols B, Bülow I, et al. Validation of ultrasonography of the thyroid gland for epidemiological purposes[J]. Thyroid, 1999, 9(11): 1069-1074.
[8] Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer[J]. Thyroid. 2009, 19(11): 1167-1214.
[9] 陳士偉, 孔凡國, 湯冬琴, 等. 浙江上海地區健康人群甲狀腺結節發病情況分析[J]. 實驗與檢驗醫學, 2014, 32(2): 214-216
[10] 邱蕾, 孫明曉, 汪耀, 等. 中年至超高齡老年人甲狀腺結節的發病特點[J].中華內分泌代謝雜志, 2014, 30(2): 115-118.
[11] 余開選, 胡朝恩, 宋曉峰, 等. 260例中老年甲狀腺結節患者3年超聲觀察結果分析[J]. 中華保健醫學雜志, 2015, 17(4): 305-328.
[12] Sousa PA, Vaisman M, Carneiro JR, et al. Prevalence of goiter and thyroid nodular disease in patients with class III obesity[J]. Arq Bras Endocrinol Metabol. 2013, 57(2): 120-125.
[13] Rendina D, De Filippo G, Mossetti G, et al. Relationship between metabolic syndrome and multinodular non-toxic goiter in an inpatient population from a geographic area with moderate iodine deficiency[J]. J Endocrinol Invest. 2012, 35(4): 407-412.
[14] Pacini F, Schlumberger M, Dralle H, et al. European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium[J]. Eur J Endocrinol. 2006. 154(6): 787-803.
[15] Filetti S, Durante C, Torlontano M. Nonsurgical approaches to the management of thyroid nodules[J]. Nat Clin Pract Endocrinol Metab. 2006, 2(7): 384-394.
[16] Quadbeck B, Pruellage J, Roggenbuck U, et al. Long-term follow-up of thyroid nodule growth[J]. Exp Clin Endocrinol Diabetes. 2002, 110(7): 348-354.
[17] Alexander EK, Hurwitz S, Heering JP, et al. Natural history of benign solid and cystic thyroid nodules[J]. Ann Intern Med. 2003, 138(4): 315-318.
[18] Erdogan MF, Gursoy A, Erdogan G. Natural course of benign thyroid nodules in a moderately iodine-deficient area[J]. Clin Endocrinol (Oxf). 2006, 65(6): 767-771.
[19] Brauer VF, Eder P, Miehle K, et al. Inter observer variation for ultrasound determination of thyroid nodule volumes[J]. Thyroid. 2005, 15(10): 1169-1175.
