Pulmonary amyloidosis and multiple myeloma mimicking lymphoma in a patient with Sjogren’s syndrome: A case report
2022-03-07 13:06:32KimKimYSLeeHJParkSG
World Journal of Clinical Cases 2022年3期
INTRODUCTION
We diagnosed the patient with pulmonary amyloidosis and multiple myeloma involving extramedullary organs (stomach, lymph nodes) associated with SS.
CASE PRESENTATION
Chief complaints
A 46-year-old male patient was admitted for treatment of an incidental gastric plasmacytoma.
History of present illness
根據一份針對大學生二手物品市場的調查報告,得知83.4%的大學生擁有閑置物品,并且多達38.6%的大學生擁有2~3件,僅2.7%的大學生宿舍閑置物品只有一件。由此可以看出,大學生二手市場具有不可小覷的規模,而且學生屬于一類特殊群體,其還沒有收入渠道,同時學生之間有一定相同的興趣愛好、具有類似的消費心理。共同的生活環境—宿舍,寢室-食堂-教室三點一線的生活起居使得大學生交易的商品具有共性(如:書本、生活用品、體育用品、代步工具等),學生之間的交易也愈加頻繁,這也是造成交易需求壓力增大的原因之一。
而在“英印人”獨特體驗的書寫上,研究者們更多地關注吉卜林在身份認同方面的焦慮與不安。殊不知,憑借獨特的人生經歷及智慧,吉卜林在主人公基姆身上實踐了對自己理想的身份的認同。
History of past illness
為便于驗證“千聊”對于MOOC結課率的影響,筆者將網絡公選課班級分為2個小組,其中,A組學生為60人,B組學生為58人。A組學生使用“千聊”進行自主學習,B組學生使用超星學習通APP進行學習,兩個平臺的課程的課件、習題、預習資料、微課資源完全一致。
第一,往大處想——定義一個更加寬泛的問題,不斷地問“這個問題背后更大的問題是什么?”和“我們要達到的更好的效果是什么?”讓思維獲得更多的自由,從而想出更多的解決方案。第二,換位思考——進入你想模仿的人或公司的思維模式,重新審視遇到的問題,放開平常的限制,會發掘出新的、未想到過的解決方法。第三,強加約束——給現狀引入一個強有力的限制,探索這樣做能帶來什么樣的好處。第四,選擇構架——怎么創造一種環境,讓人們在這種環境中選擇我們想要他們采取的行動。
Personal and family history
The patient had been diagnosed with SS four years ago due to dry eyes and dry mouth, and his symptoms improved after treatment with methotrexate, hydroxychloroquine. However, prednisolone was added two months ago due to swelling of the parotid glands and enlargement of lymph nodes.
Physical examination
A physical examination revealed painless lymph nodes of variable size in both inguinal areas and both neck areas.
他拖著膠鞋,啪噠啪噠走向外屋,又摸索著抓起幾粒鹽,把指頭伸到嘴里,用上個月才安的門牙咬破水泡,在傷口撒上鹽。他的整張臉痛得糾在一起,兩根手指緊緊捏著那根受傷的指頭。疼痛慢慢消減了,他又爬到床上,關掉電筒。
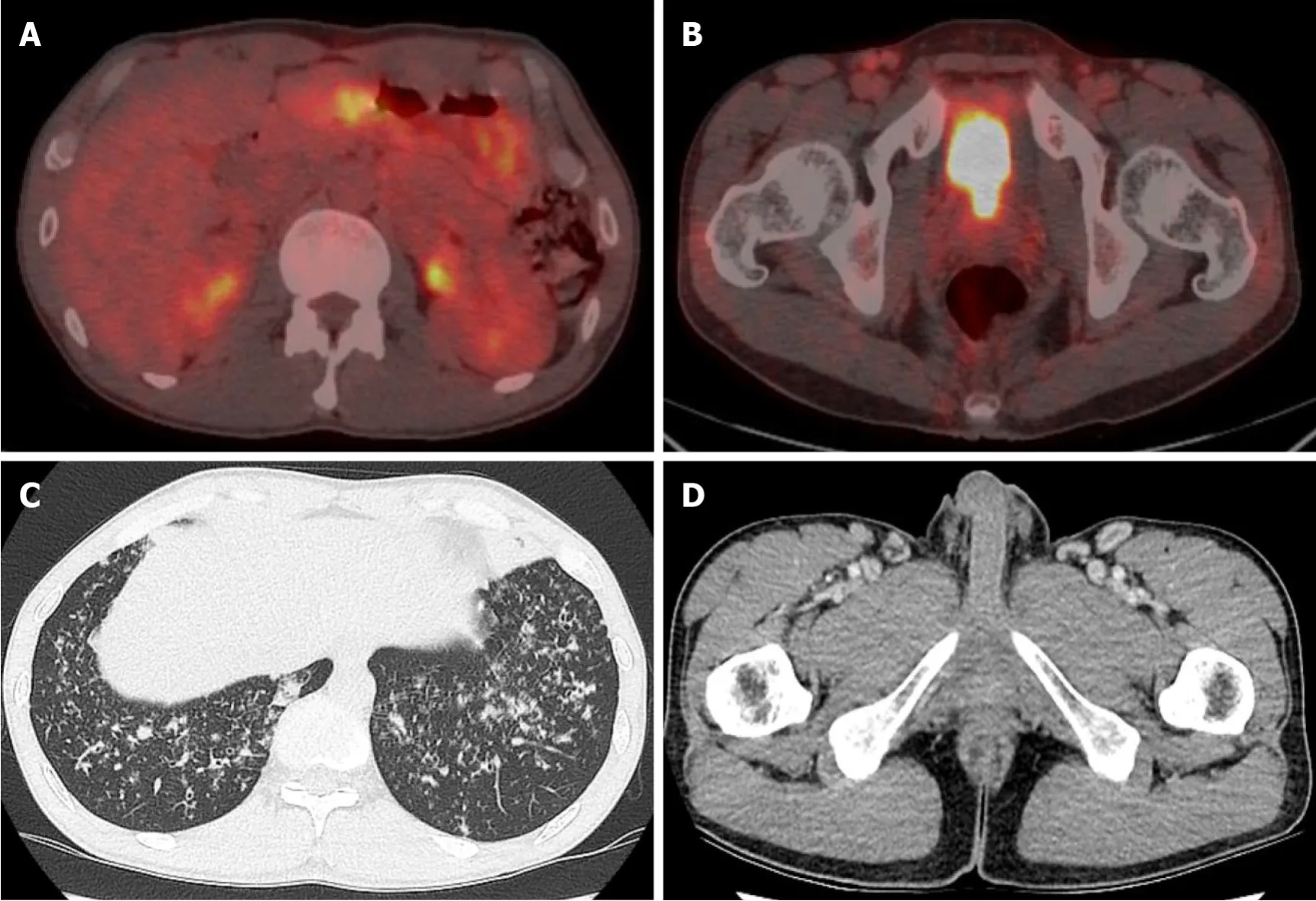
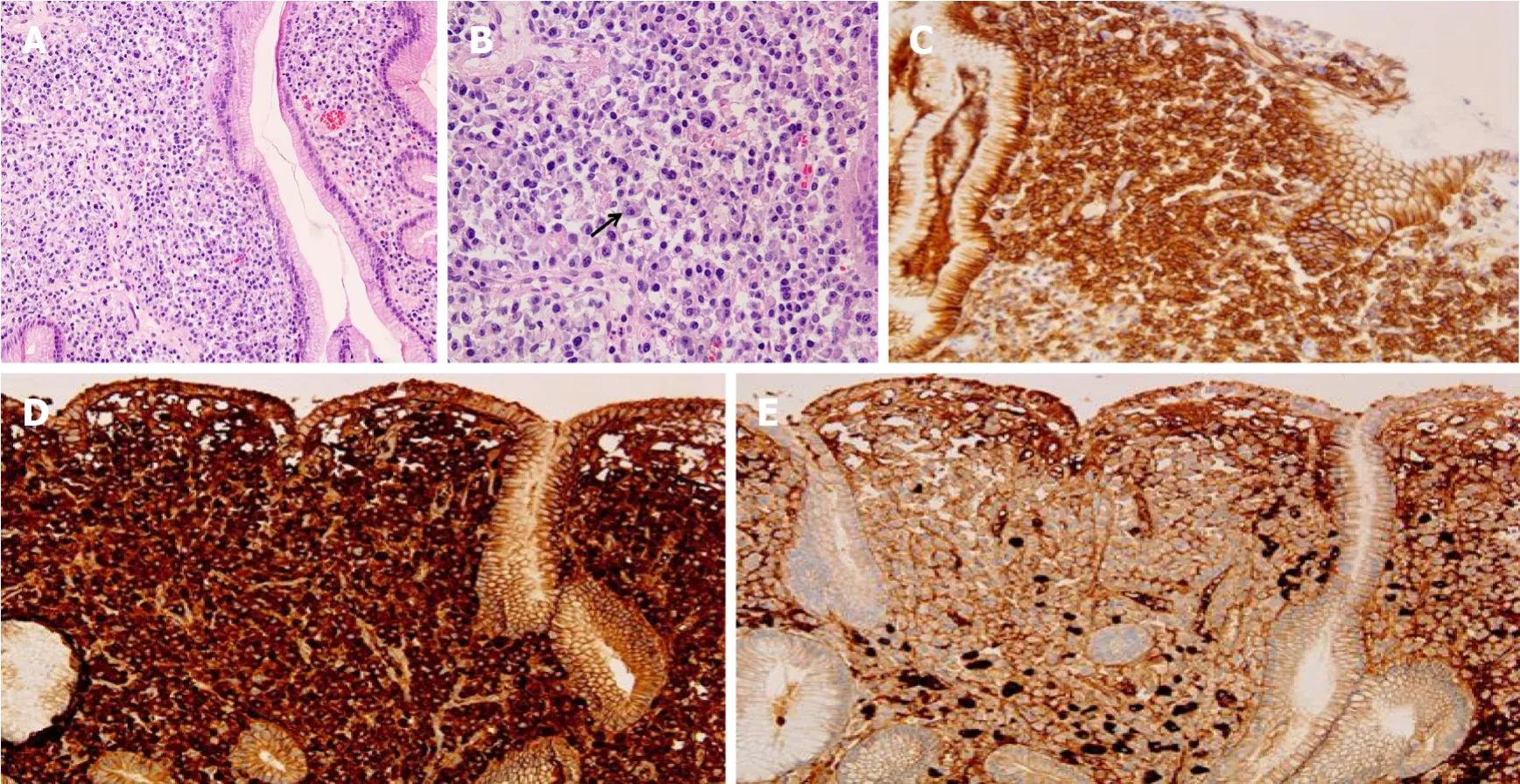
The patient was checked by a positron emission tomography (PET) scan due to enlargement of both inguinal lymph nodes more than two months ago. The PET scan revealed hypermetabolic activity in the gastric body, both inguinal lymph nodes(Figure 1A). A gastroscopic biopsy of the stomach lesion was performed and diagnosed with plasmacytoma (Figure 2).
Laboratory examinations
Although SS is typically known as an autoimmune disorder, it can also present as lymphoproliferative disease. The form of lymphoproliferative disease can present as polyclonal lymphocytic infiltration of the salivary glands, oligo- or monoclonal B cell proliferation resulting in clonally derived lymphoproliferative disorders such as monoclonal gammopathy, light-chain amyloidosis, and malignant lymphoma[3,4,6-9].SS often involves interstitial lung disease, sometimes primary pulmonary lymphoma,pleuritis, but occurrence of pulmonary amyloidosis is very rare[14].
Imaging examinations
The PET-computed tomography (CT) revealed hypermetabolic activity in the gastric body, a mild increase in metabolic activity in both inguinal areas, and ground glass opacities (GGO) and centrilobular nodules in both lung fields (Figure 1A). A chest CT showed patch GGO and multiple nodules in both lung fields (Figure 1C) and an abdominal CT showed multiple enlarged lymph nodes in the bilateral inguinal area(Figure 1D).
FURTHER DIAGNOSTIC WORK-UP
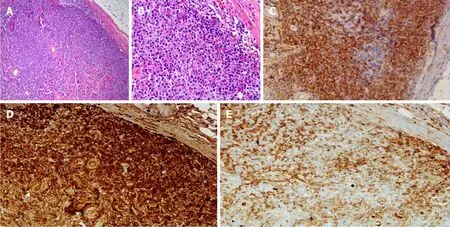
An excisional lymph node biopsy was performed for differential diagnosis of pulmonary tuberculosis with tuberculous lymphadenitis from lymphoma. Biopsy of the right inguinal lymph node revealed diffuse infiltration of plasma cells, which were positive for CD 138, Kappa, and lambda chain immunohistochemical staining(Figure 3). The results of a bone marrow biopsy showed that plasmas cells were increased to 34% and immunostain of IgG, IgA, kappa, and lambda was positive.
突出表現為生態系統產出下降,特別是漁業資源顯著下降,長江干流的年捕撈產量由20世紀50年代的40多萬t下降到現今的不足10萬t,且魚類資源小型化趨勢明顯。水生態系統結構受損,環境承載力和對污染的處理能力下降,局部江段和湖泊污染嚴重、水華時有發生,影響飲用水安全。
Systemic chemotherapy was planned for the multiple myeloma, however the patient was transferred to a larger hospital.
FINAL DIAGNOSIS
Primary Sjogren’s syndrome (SS) is a chronic systemic autoimmune disease characterized by decreased organ function by lymphocyte infiltration, not only exocrine gland but also extraglandular organ[1]. Major B cell activation is the main pathogenesis of SS and continuous activation of B cells can lead to clonal proliferation and malignant lymphoma[2-4]. Clonal proliferation of B cells may lead to both monoclonal gammopathy of undetermined significance, a benign monoclonal gammopathy, and multiple myeloma (MM), a hematologic malignancy[5-9]. However,in practice, multiple myeloma is very rare[6,7,10]. Amyloidosis is a heterogeneous group of disorders characterized by deposits in the extracellular matrix of abnormal protein material. The incidence of amyloidosis is low and that of amyloidosis with involvement of only the respiratory system is extremely low[11,12]. In particular,amyloidosis is a rare cause of pulmonary infiltration in SS[13]. Simultaneous occurrence of pulmonary amyloidosis and multiple myeloma associated with SS is extremely rare.
TREATMENT
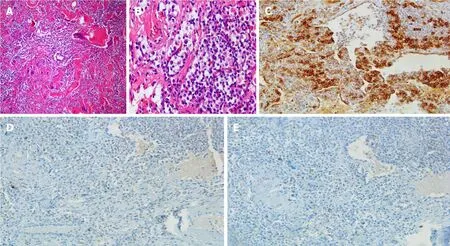
A lung biopsy was also performed to rule out pulmonary tuberculosis, interstitial lung disease, or lung involvement of multiple myeloma. Lung biopsy revealed chronic inflammation showing multinucleated giant cells and deposition of amorphous proteinaceous material (Figure 4A). Infiltration of lymphoplasmacytes was observed in the interstitium and perivascular area (Figure 4B). In addition, Congo-red stain for amorphous proteinaceous material revealed apple green birefringence under a polarized microscope. Mycobacterium tuberculosis nested polymerase chain reaction to exclude pulmonary tuberculosis was negative.
OUTCOME AND FOLLOW-UP
The patient was transferred to another hospital and underwent chemotherapy. He is on regular follow up for SS to our rheumatology department and is on medication.
DISCUSSION
The complete blood count results, with normal ranges in parentheses, were as follows:white blood cells, 5160 × 10/μL (4.0–10.0 × 10/μL); hemoglobin, 13.3 g/dL (12–16 g/dL); platelets, 305 × 10/μL (150–400 × 10/μL). Blood biochemistry results were as follows: total protein 9.03 g/dL (5.3-7.4 g/dL); albumin 3.74g/dL (3.5-5.2 g/dL), A/G ratio 0.71 (1.0-2.0); C-reactive protein, 0.49 mg/dL (0–0.3 mg/dL). The results of serum protein electrophoresis showed an increase in the total protein amount, a decrease of albumin, and a slightly sharp increase of gamma-globulin. The results of serum immunofixation electrophoresis revealed oligoclonal gammopathy; multiple dense bands were observed in IgG, IgA, kappa, and lambda antisera. The results of Ig quantification showed IgG 2540 mg/dL (700-1600); IgM 18.3 mg/dL (40-230 mg/dL);IgA 1220 mg/dL (70-400 mg/dL). B2-microglobulin level was increased to 2.8 mg/L(0.0-2.4 mg/L). The results of a serum free light chain assay revealed increased kappa light chain (420.60 mg/L, normal 3.3-19.40 mg/L) and an increased kappa/lambda light chain ratio (34.9, normal 0.26-1.65). Alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, lactate dehydrogenase, calcium, and creatinine were all within normal limits.
Amyloidosis is a disease group; certain proteins such as amyloid fibrils are deposited in extracellular tissue. Amyloidosis can be classified as primary and secondary. Primary amyloidosis is caused by clonal plasma cell proliferation which appears in monoclonal gammopathy or myeloma and the associated abnormal proteins consist of fragments of immunoglobulin light chain such as kappa and lambda (light chain amyloidosis)[15]. Secondary amyloidosis is the reactive systemic amyloidosis usually associated with chronic inflammatory diseases or neoplasms and the associated fibrils are composed of fragments of the acute phase reactant serum amyloid A (reactive amyloidosis)[15]. These two types are the most common form of amyloidosis. Amyloid deposition is rare in SS patients, but when it does occur,multiple organs are affected, such as skin, kidney, breast, tongue, and lymph nodes, as well as the lung[16-21]. However, only about 50 cases related to primary SS and pulmonary amyloidosis have been reported so far[22]. Amyloidosis of the lungs has three different clinicopathologic forms: diffuse alveolar-septal amyloidosis (diffuse parenchymal amyloidosis), nodular pulmonary amyloidosis (nodular parenchymal amyloidosis), and tracheobronchial amyloidosis[23]. Diffuse alveolar-septal amyloidosis is characterized by amyloid deposition in the alveolar septa and vessel walls, and transbronchial amyloidosis is characterized by amyloid deposition in various segments of the tracheobronchial tree[23]. Nodular pulmonary amyloidosis can be defined as one or more tumor-like amyloid deposits involving the lungs[23].Pathologically, well circumscribed nodules with homogeneous and dense eosinophilic material, lymphocytes and plasma cells are generally found within or nearby nodules[23]. Other pathologic findings that may appear include foreign body giant cells,calcifications, and bony or cartilaginous areas[23]. Lung biopsy of our patient revealed chronic inflammatory nodules showing multinucleated giant cells and deposition of amorphous proteinaceous material (Figure 4A). Infiltration of lymphoplasmacytes was observed in the interstitium and perivascular area (Figure 4B). Congo-red stain for amorphous proteinaceous material revealed apple green birefringence under a polarized microscope.
In MM, monoclonal immunoglobulin is produced by plasma cell neoplastic proliferation of plasma cells. There are two categories of MM, according to diagnostic criteria for plasma cell proliferative disorders. The first is asymptomatic multiple myeloma (smoldering multiple myeloma), which is serum monoclonal protein more than 3 g/dL and/or clonal bone marrow plasma cells more than 10% but absence of end-organ damage[5]. Symptomatic multiple myeloma satisfies all of the following:more than 10% clonal bone marrow plasma cells and presence of serum and/or urinary monoclonal protein and evidence of end-organ damage[5].
This patient had increased serum protein IgG, IgA, and Kappa light chain, and plasma cells in the bone marrow were increased to 34%. Although there was no endorgan damage such as anemia, renal insufficiency, hypercalcemia, and bone lesions,plasmacytomas were observed in multiple lymph nodes and stomach as end-organ involvement. This patient was expressed as the type of extramedullary plasmacytoma in multiple myeloma.
Plasmacytomas, tumors composed of plasma cells, are histologically identical to those observed in MM[24]. Those that occur solely in the bone are designated solitary plasmacytoma of bone[25]. Those that arise outside bone in soft tissues are called solitary extramedullary plasmacytoma (EMP)[25]. EMP can arise anywhere in the body. The incidence of extramedullary disease with newly diagnosed MM is variable,ranging from 7%-13%[26]. EMP arise most commonly from direct extension of primary bone tumors, but rarely they may also result from hematogenous spread involving distant organs[26].
The incidence of benign monoclonal gammopathy in SS patients is relatively high and a prevalence of monoclonal gammopathy in primary SS patients of 7% to 22% was recently reported[6-8], however, the prevalence of MM is very rare[6,7,10]. IgG is the most common class associated with MM[7]. This report describes a patient with SS associated with IgG and IgA-kappa-type MM.
Amyloidosis and MM associated primary SS is rare but can occur respectively.However, no cases of simultaneous occurrence of MM and amyloidosis in patients with SS have been reported. Of course, there is a limitation which cannot rule out the occurrence of pulmonary amyloidosis caused by MM. However, abnormal proteins of pulmonary amyloidosis caused by MM consist of fragments of immunoglobulin light chains such as kappa and lambda. Pulmonary amyloidosis was diagnosed in our patient’s lung biopsy, but immunohistochemistry of kappa and lambda was negative.Therefore, we report a rare case diagnosed simultaneously with pulmonary amyloidosis and multiple myeloma associated with SS.
CONCLUSION
SS is a chronic inflammatory disease characterized by decreased organ function by lymphocyte infiltration, not only exocrine gland but also extraglandular organ.Interstitial lung disease is the most common pulmonary abnormality in primary SS,but pulmonary amyloidosis is rare. Monoclonal gammopathy can also occur, but progression to MM is rare in primary SS. To the best of our knowledge, simultaneous development of MM and pulmonary amyloidosis in primary SS patients has not been reported so far. Herein, we report the extremely rare case of pulmonary amyloidosis and multiple myeloma associated with SS.
猜你喜歡
小雪花·初中高分作文(2021年4期)2021-08-27 09:21:34
中老年保健(2021年12期)2021-08-24 03:30:40
中國傳媒大學學報(自然科學版)(2021年1期)2021-06-09 08:43:00
中國生殖健康(2020年6期)2020-02-01 06:28:50
下一代英才(酷炫少年)(2019年3期)2019-03-25 02:34:18
中國生殖健康(2019年11期)2019-01-07 01:28:02
小雪花·初中高分作文(2018年4期)2018-12-12 10:32:28
絲路藝術(2018年8期)2018-09-27 09:24:40
黃河之聲(2017年14期)2017-10-11 09:03:59
小雪花·初中高分作文(2016年2期)2016-05-30 16:36:19
 World Journal of Clinical Cases2022年3期
World Journal of Clinical Cases2022年3期
- World Journal of Clinical Cases的其它文章
- Mycoplasma hominis meningitis after operative neurosurgery: A case report and review of literature
- Recurrence of sigmoid colon cancer–derived anal metastasis: A case report and review of literature
- New method to remove tibial intramedullary nail through original suprapatellar incision: A case report
- Metastasis to the thyroid gland from primary breast cancer presenting as diffuse goiter: A case report and review of literature
- Gastric submucosal lesion caused by an embedded fish bone: A case report
- Epibulbar osseous choristoma: Two case reports