橫竇變異對完全/部分前循環梗死臨床轉歸影響的研究
2022-04-28 21:43:22吳連爽趙維納尹昌浩徐丹
中國現代醫生 2022年9期
吳連爽 趙維納 尹昌浩 徐丹
[摘要] 目的 探討有無橫竇變異對前循環梗死患者的臨床轉歸的影響。 方法 收集2019年2月至2020年12月發病且發病48 h內就診于牡丹江醫學院附屬紅旗醫院、第二醫院神經內科的已行頭顱CT/DWI/MRI檢查前經腦梗死牛津郡社區卒中項目(OCSP)臨床分型明確為完全前循環梗死(TACI)患者和部分前循環梗死(PACI)患者,最終對75例前循環梗死患者進行磁共振靜脈血管成像(MRV)及頸靜脈彩超檢查,根據檢查結果分為橫竇無變異與橫竇變異兩組,記錄橫竇變異分級、頸內靜脈管徑、梗死體積、基線NIHSS評分、90 d mRS評分。分析橫竇變異對完全/部分前循環梗死部位、梗死體積及臨床轉歸的影響。 結果 前循環梗死患者中,橫竇變異側與同側前循環梗死的形成有關,差異有統計學意義(P<0.05)。橫竇變異同側的頸內靜脈管徑顯著小,差異有統計學意義(P<0.05)。完全前循環梗死合并橫竇變異組患者的基線NIHSS和90 d mRS評分均高于部分前循環梗死合并橫竇變異組,差異均有統計學意義(P<0.05)。完全前循環梗死橫竇變異組90 d mRS評分高于無變異組,差異有統計學意義(P<0.05)。 結論 橫竇變異更容易發生同側前循環梗死,且橫竇變異同側的頸內靜脈管徑顯著小;合并橫竇變異的完全前循環梗死與部分前循環梗死比較,臨床癥狀重、預后差;完全前循環梗死合并橫竇變異組的預后更差。
[關鍵詞] 腦梗死;前循環;橫竇變異;轉歸預后
[中圖分類號] R743.3? ? ? ? ? [文獻標識碼] A? ? ? ? ? [文章編號] 1673-9701(2022)09-0021-05
Study on the impacts of transverse sinus variation on the clinical outcome of total/partial anterior circulation infarcts
WU Lianshuang1? ZHAO Weina2,3? ?YIN? Changhao2,3? ?XU? Dan2,3
1.Mudanjiang Medical University, Mudanjiang? ?157000, China; 2.Department of Neurology IV, Hongqi Hospital Affiliated to Mudanjiang Medical University, Mudanjiang? ?157000, China; 3.Key Laboratory of Ischemic Stroke Prevention and Control in Heilongjiang Province,Mudanjiang? ?157000,China
[Abstract] Objective To investigate the impacts of the presence or absence of transverse sinus variation on the clinical outcome of patients with anterior circulation infarcts. Methods Patients who were admitted to the Department of Neurology of Hongqi Hospital Affiliated to Mudanjiang Medical University and The Second Affiliated Hospital of Mudanjiang Medical University from February 2019 to December 2020 with onset within 48 hours and who had undergone cranial computed tomography (CT)/diffusion weighted imaging (DWI)/ magnetic resonance imaging (MRI), and clinically diagnosed with clinical typing of total anterior circulation infarcts (TACI) and partial anterior circulation infarcts (PACI) by the Oxfordshire Community Stroke Project (OCSP) for cerebral infarction were selected as the study subjects. 75 patients with anterior circulation infarcts who underwent magnetic resonance venography (MRV) and jugular vein ultrasound examination were divided into the non-transverse sinus variation group and the transverse sinus variation group according to the examination results. The grading of transverse sinus variation, internal jugular vein diameter, infarct volume, the score of National Institute of Health Stroke Scale (NIHSS) at baseline, and 90-day modified Rankin Scale (mRS) score were recorded. The impacts of transverse sinus variation on the site, infarct volume, and clinical outcome of TACI/PACI were analyzed. Results In patients with anterior circulation infarcts, the transverse sinus variant was associated with the formation of ipsilateral anterior circulation infarcts,with statistically significant difference(P<0.05). The diameter of the internal jugular vein on the ipsilateral side of the transverse sinus variant was significantly smaller, with statistically significant difference(P<0.05).The baseline NIHSS and 90-day mRS scores were higher in the TACI combined with transverse sinus variant group than those in the PACI combined with transverse sinus variant group, with statistically significant differences(P<0.05).The 90-day mRS score was higher in the TACI combined with transverse sinus variant group than that in the non-transverse sinus variation group, with statistically significant difference(P<0.05). Conclusion Transverse sinus variation is more likely to result in ipsilateral anterior circulation infarcts, and the internal jugular vein diameter on the ipsilateral side of transverse sinus variation is significantly smaller. Compared with the PACI combined with transverse sinus variant group, there are severer clinical symptoms and worse prognosis in the TACI combined with transverse sinus variation group. In addition, the prognosis of TACI combined with transverse sinus variation group is worse than that of the PACI combined with transverse sinus variant group.
[Key words] Cerebral infarction; Anterior circulation; Transverse sinus variation; Outcome and prognosis
前循環梗死(anterior circulation infarction,ACI)是導致患者具有更高的缺血性卒中發生率及預后差的梗死類型[1-2]。根據OCSP臨床分型前循環腦梗死分為完全前循環梗死(TACI)和部分前循環梗死(PACI)[3]。研究表明[4-5],急性腦梗死中,TACI患者的神經功能損害最重,康復時間最長,預后最差。腦循環包括動脈和靜脈系統,既往研究過多的關注于動脈血管變化,但靜脈、靜脈竇在腦血流及顱內壓力改變中居主要地位[6]。顱內靜脈變異較多,但大多數患者無臨床癥狀[7]。橫竇(transverse sinus,TS)是正常人靜脈竇變異的最常見類型[8],且越來越多的研究表明[5],TS變異在整個腦靜脈及靜脈血流動力學中有重要作用。
筆者認為TS變異在動脈梗死事件中的作用可能涉及以下2個方面:①先天橫竇變異影響動脈血液回流,長年累月使動脈粥樣硬化的進程加重;②橫竇變異影響動脈回流,導致大面積前循環梗死急性期的水腫加重,直接影響預后。本研究通過對前循環梗死患者的橫竇變異分析,評估其對前循環梗死的發生率、疾病嚴重程度的影響以及臨床轉歸等方面的臨床價值,現報道如下。
1 資料與方法
1.1 一般資料
收集2019年2月至2020年12月發病且發病48 h內就診于牡丹江醫學院附屬紅旗醫院、第二醫院神經內科的已行頭顱DWI/MRI證實為前循環梗死的75例患者,并在48 h之內完成頭MRV及頸內靜脈彩超檢查,檢查結果由一名有經驗的影像、超聲科醫師和一名神經科醫師經過培訓后進行盲法評估。課題研究通過牡丹江醫學院醫學倫理委員會的審批,所有被試者均需簽署知情同意書。
1.2 磁共振成像方法
均采用荷蘭飛利浦公司3.0T TX磁共振儀進行影像學系統掃描,常規行T1WI、T2WI、Flair、DWI、MRV檢查,MRV檢查參數:采用三維相位對比(phase contrast,PC),流速編碼Venc=15 cm/s,TR/TE=25 ms/6 ms,翻轉角10°,矩陣256×256,層厚0.8 mm。
1.3 診斷標準
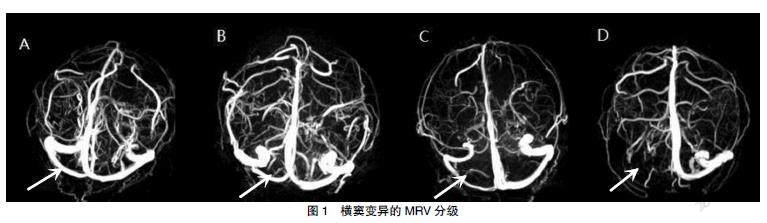
TS變異不對稱分級標準:由于TS中段易于識別及測量,故選擇中段測量TS管徑(cm)。在MRV中,根據雙側TS是否不對稱,被分成4級[9]。TS變異是指2級及3級。MRV見圖1。
根據TS是否對稱MRV分為4級。A:0級(TS雙側不對稱≤10%,箭頭);B:1級(TS不對稱>10%,且≤50%,箭頭);C:2級(TS不對稱>50%,箭頭;D:3級(TS纖細或者缺失,箭頭)。
靜脈彩超評定標準:雙源彩色超聲通過7-MHz線性傳感器(iU22;美國飛利浦醫藥系統)傳導,技術人員對患者臨床信息行盲法評定。在頸內靜脈中段(J2)和上段(J3)記錄以下參數:時間平均中位流速和管腔橫截面積。
1.4 統計學方法
應用SPSS 25.0統計學軟件處理數據,計量資料用均數±標準差(x±s)表示,采用t檢驗。計數資料用[n(%)]表示,采用χ2檢驗。P<0.05為差異有統計學意義。
2 結果
2.1 橫竇變異率及橫竇變異的意義
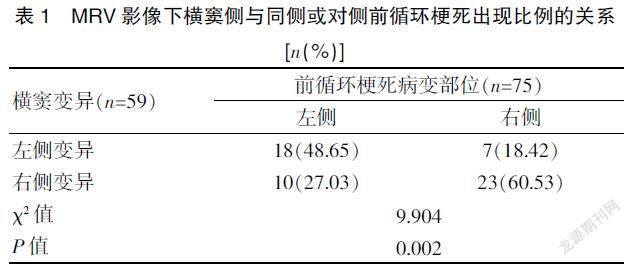
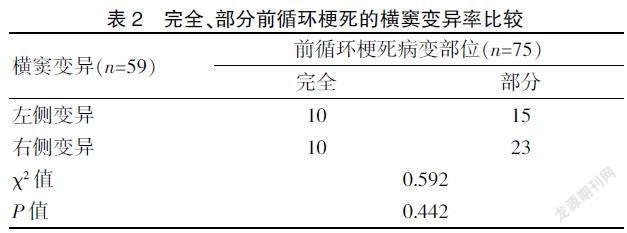
在所有前循環梗死患者中,橫竇變異在同側前循環梗死的發生率高,差異有統計學意義(P<0.05)。在完全、部分前循環梗死患者中橫竇變異率比較,差異無統計學意義(P>0.05)。見表1~2。
2.2 完全前循環梗死患者的橫竇變異情況
一例78歲老年男性患者,DWI示左側完全前循環梗死(圖2A,箭頭),入院第3天臨床癥狀加重,行頭CT示:梗死面積較前增大(圖2B,箭頭),MRV顯示同側橫竇變異(圖2C,箭頭)。一例67歲老年女性患者DWI示左側完全前循環梗死(圖2D,箭頭),入院第5天臨床癥狀加重,行頭CT示:梗死面積較前增大,出現腦水腫且同側側腦室受壓(圖2E,箭頭),MRV顯示對側橫竇變異(圖2F,箭頭)。
2.3 頸內靜脈管徑不對稱的意義
橫竇變異同側的頸內靜脈管徑顯著小,其與非變異橫竇側比較,差異有統計學意義(χ2=33.446,P<0.001)。見表3。
2.4 前循環梗死合并有無橫竇變異與責任病灶體積的關系
在前循環梗死患者中,合并TS變異的梗死體積明顯增大(表現為大、中、小梗死灶均較無橫竇變異組人數增多)。見圖3。橫竇無變異與橫竇變異組中各種梗死灶體積的大小比較,差異無統計學意義(P>0.05)。見表4。
2.5 前循環梗死患者與橫竇有無變異間臨床轉歸分析
與PACI組比較,合并橫竇變異的TACI組具有更差的NIHSS及90 d mRS評分,差異均有統計學意義(P<0.05),TACI合并橫竇變異組與無橫竇變異組比較,90 d的mRS評分更差,差異有統計學意義(P<0.05)。見表 5。
注 *TACI橫竇變異與PACI橫竇變異組相比,P<0.05,且NIHSS、mRS評分,分別為t=8.108,P=0.000;t=8.108,P=0.001;#TACI橫竇無變異與PACI橫竇無變異組相比,P<0.05,但NIHSS、mRS評分的統計值分別為t=3.799,P=0.055;t=2.267,P=0.053;^TACI橫竇變異與TS無變異組相比,P<0.05,而NIHSS、mRS評分的統計值分別為t=0.219,P=0.829;t=3.213,P=0.012;&PACI橫竇變異與無變異組相比,P<0.05,但NIHSS、mRS評分的統計值分別為t=0.781,P=0.438;t=0.612,P=0.543
3 討論
3.1 前循環梗死與TS變異相關性分析
3.1.1 前循環梗死與TS變異率? 本研究中右側TS變異33例,變異率為56.0%,但與完全/部分前循環梗死的發生率比較,差異無統計學意義(P>0.05)。研究結果與既往文獻一致,認為TS通常不對稱,TS發育不良或發育不全是一種常見的解剖學變異,約30%左右的病例會出現TS一側閉鎖或發育不良,且半數以上的病例以右側TS為主[10]。TS變異可能與先天解剖結構、發育異常有關。如果TS在發育過程中迅速增大和減小,可能會發生TS的變異,如直徑和邊緣不規則、間隔形成和節段缺失[11]。
3.1.2 前循環梗死形成與TS變異? 本研究結果顯示,TS變異更容易發生同側前循環梗死,即TS變異與同側ACI的形成有關,其與非變異橫竇側比較,差異有統計學意義(P<0.05)。研究結果與Drozdov等[12]的結果符合,通過觀察5例MCA梗死后出現致死性腦水腫的患者中有4例出現TS橫竇變異,與出現同側顱內靜脈引流異常的結果符合。可能原因是TS變異引起腦靜脈血液回流障礙,導致顱內靜脈的引流異常,在靜脈系統和毛細血管內淤積的血液,引起局部的腦組織腫脹,進而導致顱內壓增高[13]。顱內壓增高損害腦血管自主調節功能,延長腦循環時間,影響動脈血液回流,加速動脈粥樣硬化的進程[14],從而易形成同側動脈血栓且導致臨床癥狀加重。雖然本實驗中發現橫竇變異與同側前循環梗死的發生率相關,但樣本量較小,仍需大樣本實驗證實。
3.1.3 前循環梗死TS變異與頸內靜脈管徑? 因本研究行頸內靜脈彩超時受技術所限未獲得患者血流量相關數值,故只評估了管徑,通過評估頸內靜脈管徑后發現,管徑不對稱比例約48%,且與橫竇變異側做分析后,結果提示TS變異同側的頸內靜脈管徑顯著小,這也與先前研究一致[15-17]。從血流動力學的角度來看,毛細血管和靜脈是腦血管阻力的重要貢獻者,但在生理條件下,它們在血流調節中的作用微乎其微,當出現缺血時,阻力小動脈和動脈最大限度地擴張并變得反應遲鈍[18]。那么,橫竇變異與頸內靜脈管徑不對稱導致血流動力學異常也可以解釋。但由于本研究中受限彩超技術,導致未獲得頸內靜脈血流量相關數值。
3.2 TS變異與前循環梗死患者梗死體積的關系
本研究中,梗死體積在TS無變異與TS變異組間比較,差異均無統計學意義(P>0.05),與Tumanova等[19]研究的梗死體積的增大在靜脈竇變異后導致缺血性卒中水腫加重有關的結果不一致。可能與入組患者人數較少、臨床嚴重程度中等程度偏上有關。靜脈系統形態的異常是否類似于不完整的Willis環的后果仍需要縱向研究。
3.3 前循環梗死合并橫竇變異的臨床轉歸影響分析
王本孝等[20]發現OCSP的這四種臨床類型中,TACI患者入院時病情、神經功能缺損重,梗死面積大,預后差,致殘率高。NIHSS、90 d mRS是評價患者神經功能缺損嚴重程度、恢復情況的評估指標,評分越低意味著癱瘓程度越輕、預后越好。本研究中,完全/部分前循環梗死橫竇不同變異類型之間,TACI橫竇變異與PACI橫竇變異組比較,TACI橫竇變異組的NIHSS及90 dmRS評分更高,提示與嚴重的臨床癥狀、預后差有關。TACI橫竇變異與無變異組比較,TACI變異組的90 d mRS評分更高,提示預后差。本研究結果與早前的研究結果具有較好的一致性,如Kaartinen[21]等研究表明,在9例MCA梗死患者中有3例出現致死性水腫,腦血管造影顯示同側TS閉鎖和頸內靜脈發育不良,發現除梗死體積外,同側顱內引流靜脈發育不良或閉塞與MCA梗死早期致死性水腫有關,導致更嚴重的臨床表現。另外,Munuera等[22]研究發現梗死同側橫竇閉塞或發育不良的患者預后差,同側頸內靜脈閉塞或發育不良的發生率與預后良好的患者相當。對側橫竇閉塞、發育不良或對側頸內靜脈閉塞、發育不良在預后較差的患者與功能良好的患者中比例相似。隨著人們對腦靜脈循環的興趣的發展,應該更好地了解靜脈及靜脈竇及其在動脈缺血性腦水腫中的作用。本研究入組患者多數為中等程度的梗死,完全前循環梗死的患者數量相對較少,可能影響一些統計結果。
綜上所述,TS變異更容易發生同側前循環腦梗死,且TS變異同側的頸內靜脈管徑顯著小。合并TS的TACI組與PACI組比較,臨床癥狀重、預后差。與TACI無變異組比較,合并TS變異組的預后更差。
[參考文獻]
[1]? ?Zhang K,Li T,Tian J,et al. Subtypes of anterior circulation large artery occlusions with acute brain ischemic stroke[J]. Sci Rep,2020,10(1): 3442.
[2]? ?Flint AC,Bhandari SG,Cullen SP,et al. Detection of anter- ior circulation large artery occlusion in ischemic stroke using noninvasive cerebral oximetry[J].Stroke,2018,49(2):458-460.
[3]? ?Tinker RJ,Smith CJ,Heal C,et al. Predictors of mortality and disability in stroke-associated pneumonia[J].Acta Neurol Belg,2021,121(2):379-385.
[4]? ?Yang Y,Torbey MT. Angiogenesis and blood-brain barrier permeability in vascular remodeling after stroke[J].Curr Neuropharmacol,2020,18(12):1250-1265.
[5]? ?Hua J,Liu P,Kim T,et al. MRI techniques to measure arterial and venous cerebral blood volume[J].Neuroimage,2019,187:17-31.
[6]? ?Saposnik G,Barinagarrementeria F, Brown RD Jr, et al. Diagnosis and management of cerebral venous throm-bosis:A statement for healthcare professionals from the American Heart Association/American Stroke Association[J].Stroke,2011, 42(4):1158-1192.
[7]? ?Quan T,Ren Y,Lin Y,et al. Role of contrast-enhanced magnetic resonance high-resolution variable flip angle turbo-spin-echo(T1 SPACE) technique in diagnosis of tra-nsverse sinus stenosis[J].Eur J Radiol,2019,120: 108 644.
[8]? ?Gul B,Samanci C,Uluduz DU,et al. Does measurement of the jugular foramen diameter on MRI help to differentiate transverse sinus thrombosis from unilateral transverse sinus hypoplasia[J].Radiol Med,2021,126(3):430-436.
[9]? ?Fofi L,Giugni E,Vadalà R,et al. Cerebral transverse sinus morphology as detected by MR venography in patients with chronic migraine[J]. Headache,2012,52(8):1254-1261.
[10]? Arauz A,Chavarria-Medina M,Pati?觡o-Rodriguez HM,et al. Association between transverse sinus hypoplasia and cerebral venous thrombosis:A case-control study[J].J Stroke Cerebrovasc Dis,2018,27(2):432-437.
[11]? Massrey C,Altafulla JJ,Iwanaga J,et al.Variations of the transverse sinus: Review with an unusual case report[J].Cureus,2018,10(9):e3248.
[12]? Drozdov AA,Javan R,Leon Guerrero CR,et al. Asymmetry of medullary veins on multiphase CT-angiography in patients with acute ischemic stroke[J].J Stroke Cerebrovasc Dis,2020,29(10):105 064.
[13]? Tong LS,Guo ZN,Ou YB,et al. Cerebral venous collaterals: A new fort for fighting ischemic stroke[J].Prog Neurobiol,2018,(163-164): 172-193.
[14]? Liu M,Xu H,Wang Y,et al. Patterns of chronic venous insufficiency in the dural sinuses and extracranial draining veins and their relationship with white matter hyperintensities for patients with Parkinson's disease[J]. J Vasc Surg,2015,61(6):1511-1520.
[15]? Vink A,Schoneveld AH,Richard W,et al. Plaque burden, arterial remodeling and plaque vulnerability:Determined by systemic factors[J].J Am Coll Cardiol,2001,38(3):718-723.
[16]? Saiki K,Tsurumoto T,Okamoto K,et al. Relation between bilateral differences in internal jugular vein caliber and flow patterns of dural venous sinuses[J].Anat Sci Int,2013, 88(3):141-150.
[17]? Matsuda W,Sonomura T,Honma S,et al. Anatomical varia- tions of the torcular Herophili: Macroscopic study and clinical aspects[J]. Anat Sci Int,2018,93(4):464-468.
[18]? Connor-Schuler R,Daniels L,Coleman C,et al. Presence of spontaneous echo contrast on point-of-care vascular ultrasound and the development of major clotting events in coronavirus disease 2019 patients[J].Crit Care Explor,2021,3(1):e0320.
[19]? Tumanova UN,Lyapin VM,Burov AA,et al. The possibility of postmortem magnetic resonance imaging for the diagno- stics of lung hypoplasia[J].Bull Exp Biol Med,2018,165(2):288-291.
[20]? 王本孝,許平.急性腦梗死OCSP分型與頸動脈粥樣硬化的相關性[J].中國動脈硬化雜志,2010,18(11):885-888.
[21]? Kaartinen M,van der Wal AC,van der Loos CM,et al. Mast cell infiltration in acute coronary syndromes:Implications for plaque rupture[J].J Am Coll Cardiol,1998, 32(3):606-612.
[22]? Munuera J,Blasco G,Hernández-Pérez M,et al. Venous imaging-based biomarkers in acute ischaemic stroke[J]. J Neurol Neurosurg Psychiatry,2017,88(1): 62-69.
(收稿日期:2021-05-12)
