共管模式治療老年股骨粗隆間骨折的效果
2022-05-03 00:39:12張波張成林
中國醫藥科學 2022年6期
張波 張成林

[摘要] 目的探討應用老年科- 骨科共管模式對治療老年股骨粗隆間骨折療效的影響。方法選取129例南京醫科大學附屬宿遷第一人民醫院2019年 4月至2020年 12月收治的65歲及以上股骨粗隆間骨折患者。將共管模式治療的55例患者作為共管組,將骨科治療的74例患者作為對照組。比較兩組患者 mFI-5得分情況、48 h 內手術率、術后并發癥發生率和術后半年內病死率。結果共管組患者 mFI-5得分明顯高于對照組;48 h 內手術率(52.73%,29/55)明顯高于對照組(17.57%,13/74);術后并發癥發生率(21.82%,12/55)明顯低于對照組(40.54%,30/74);術后半年內病死率(7.27%,4/55)明顯低于對照組(20.27%,15/74),差異有統計學意義( P <0.05)。結論老年科- 骨科共管模式可提高患者早期手術率、減少術后并發癥及術后半年內死亡的發生,提高手術治療效果。
[關鍵詞] 共管模式;老年人;股骨粗隆間骨折;并發癥;病死率
[中圖分類號] R683.42??? [文獻標識碼] A??? [文章編號] 2095-0616(2022)06-0154-04
Efficacy of the co-management mode in the treatment of femoral intertrochanteric fractures in the elderly
ZHANG? Bo ????ZHANG? Chenglin2
1.Department of Rehabilitation Medicine, the Affiliated Suqian First People’s Hospital of Nanjing Medical University, Jiangsu, Suqian 223800, China;2. Department of Geriatric Medicine, the Affiliated Suqian First People’s Hospital of Nanjing Medical University, Jiangsu, Suqian 223800, China
[Abstract] Objective To explore the effect of the geriatric-orthopedic co-management mode on the efficacy in the treatment of femoral intertrochanteric fractures in the elderly. Methods A total of 129 patients aged 65 years and above with femoral intertrochanteric fractures admitted to the Affiliated Suqian First People’s Hospital of Nanjing Medical University from April 2019 to December 2020 were selected as study subjects.55 patients treated with the co-management mode were included in the co-management group, while 74 patients treated in the orthopedic department were included in the control group. The mFI-5 scores, surgery rate within 48 h, the incidence of postoperative complications and mortality rate within six months after surgery were compared between the two groups. Results The mFI-5 scores of patients in the co-management group were significantly higher than those in the control group, the surgery rate within 48 h in the co-management group (52.73%, 29/55) was significantly higher than that in the control group (17.57%, 13/74), and the incidence of postoperative complications in the co-management group (21.82%, 12/55) was significantly lower than that in the control group (40.54%, 30/74). Besides, the mortality rate within six months after surgery in the co-management group (7.27%, 4/55) was significantly lower than that in the control group (20.27%, 15/74). All differences were statistically significant between the two groups (P <0.05). Conclusion The geriatric- orthopedic co-management mode can improve the early surgery rate, reduce the occurrence of postoperative complications and death within six months after surgery, and improve the efficacy of surgical treatment.
[Key words] Co-management mode; Elderly; Femoral intertrochanteric fractures; Complications; Mortalit
隨著社會老齡化程度的加深,老年人髖部骨折的發病率不斷增加,而作為其中最常見的類型,股骨粗隆間骨折的發生率也在不斷增加。鑒于高致殘率和高致死率是該病的兩大重要特點,因此如何提高老年股骨粗隆間骨折患者的手術療效、生存質量及存活率是目前亟待研究的問題。研究表明,衰弱可提高包括髖部骨折在內的多種疾病病死率及術后并發癥發生率[1-5]。5項 -改良衰弱指數(5-factor modified frailty index, mFI-5)是評估衰弱的工具之一,得分越高,衰弱程度越重,其在預測多種手術的預后中起到重要作用[6-10]。有研究認為老年科-骨科共管模式可提高老年髖部骨折患者的治療效果、減少術后并發癥的發生、降低病死率[11-14],但也有研究認為共管模式并不能使患者從中獲益[15]。2019年 4月,南京醫科大學附屬宿遷第一人民醫院成立了老年股骨粗隆間骨折多學科診療團隊,采用老年科- 骨科共管模式對部分老年股骨粗隆間骨折患者進行救治。本研究觀察共管模式對治療老年股骨粗隆間骨折效果的影響。
1 資料與方法
1.1? 一般資料
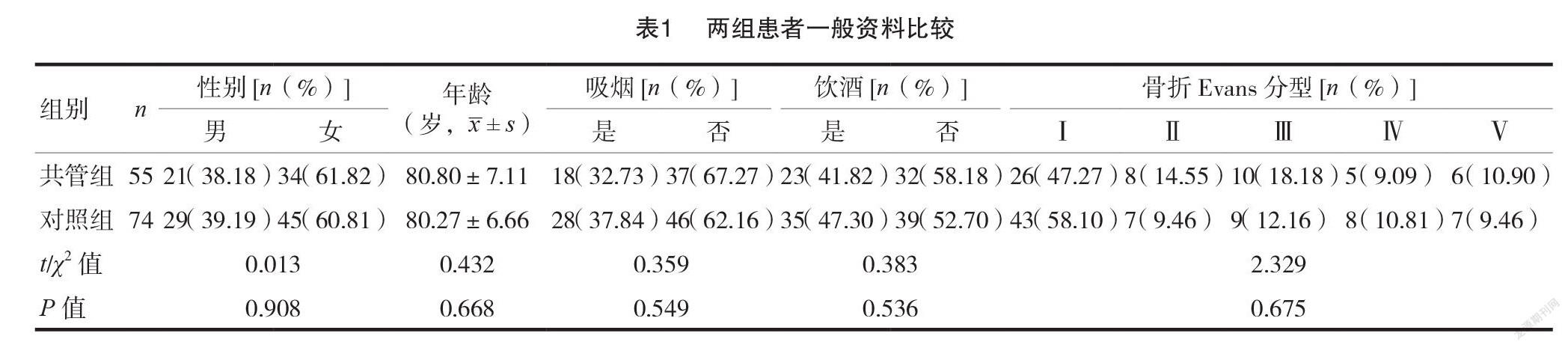
本研究選取南京醫科大學附屬宿遷第一人民醫院2019年 4月至2020年 12月收治129例 65歲及以上股骨粗隆間骨折患者。將老年科- 骨科共管模式治療的55例患者作為共管組,男21例,女34例,年齡65~ 93歲,吸煙18例,飲酒23例,骨折 Evans 分型:Ⅰ 型26例、Ⅱ型 8例、Ⅲ型 10例、Ⅳ型5 例、Ⅴ型6 例;骨科治療的74例患者作為對照組,男29例,女45例,年齡66~ 96歲,吸煙28例,飲酒35例,骨折 Evans 分型:Ⅰ型43例、Ⅱ型7 例、Ⅲ型9 例、Ⅳ型8 例、Ⅴ型7 例。本研究經醫院醫學倫理委員會批準(2020-SL-0091)。見表1。
1.2? 納入與排除標準
納入標準:① 65歲及以上老年人;②僅單側股骨粗隆間骨折患者,且在院期間行股骨近端閉合復位髓內釘固定術;③低能量損傷者;④就診距受傷時間≤24 h。排除標準:①合并其他類型骨折;
②假體周圍骨折和腫瘤等原因所致的病理性骨折;
③在院時行其他手術治療;④失訪或有數據缺失。
1.3? 診治流程
自2019年 4月老年股骨粗隆間骨折多學科診療團隊成立以來,患者的診治流程如下:①急診完善相關檢查;②按內科疾病病情輕重分別收住骨科(輕度)和共管病房(中重度);③收住共管病房的患者,老年科負責綜合管理,老年科、骨科、麻醉科共同負責手術時機和麻醉方案的確定,骨科負責準備和實施手術,康復科負責術后康復的指導。
1.4? 觀察指標
mFI-5由是否有糖尿病史、治療中的高血壓病、充血性心力衰竭史、慢性阻塞性肺疾病病史或肺部感染以及機體功能狀態(完全或部分依賴)5項得分之和計算而來[16]。每項陽性計1 分,陰性計0 分。本研究收集患者的一般資料、mFI-5 得分、術前等待時間、術后發生并發癥例數、術后半年內死亡例數。比較兩組患者 mFI-5得分情況、48 h 內手術率、術后并發癥發生率、術后半年內病死率。
1.5? 統計學方法
采用 IBM SPSS 19.0進行數據分析,計量資料首先采用 Shapiro-Wilk 檢驗判斷是否符合正態分布,對符合正態分布及方差齊的計量資料,以均數± 標準差(x ±s)表示,兩組間比較采用獨立樣本 t 檢驗;對不符合正態分布的計量資料采用 Mann-Whitney U? 秩和檢驗分析;計數資料用[n(%)]表示采用χ2?? 檢驗。 P <0.05為差異有統計學意義。
2 結果
2.1? 患者mFI-5得分比較
共管組患者 mFI-5得分明顯高于對照組,差異有統計學意義( P <0.05)。見表2。
2.2? 患者相關指標比較
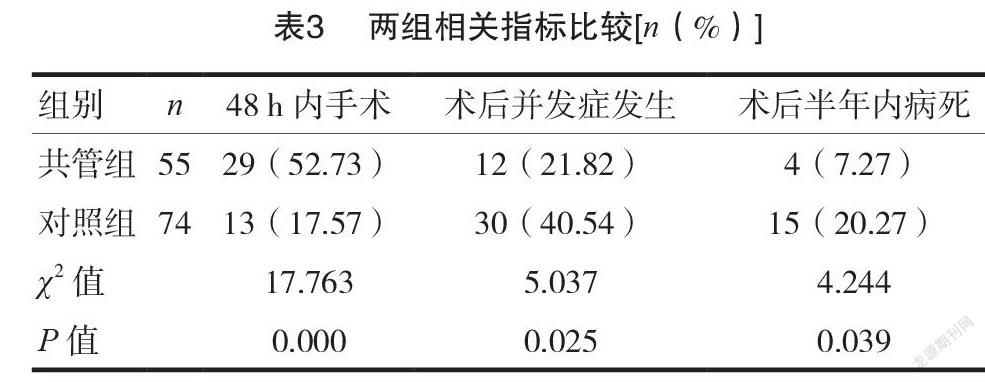
共管組患者48 h 內手術率高于對照組、術后并發癥發生率及術后半年內病死率低于對照組,差異有統計學意義( P <0.05)。見表3。
3 討論
股骨粗隆間骨折是一種脆性骨折,多見于低能量損傷的老人,首選治療方法為手術,跌倒是其最常見病因。多項研究和指南推薦,48 h 內完成手術可減少患者術后并發癥和死亡的發生[17-19]。但因老年人內科并發癥較多,外科醫生管理內科疾病的臨床能力有所欠缺,常需內科等多科室會診協同治療,可能貽誤手術時機、延長住院時間、降低治療效果等。
本研究結果顯示共管組患者48 h 內手術率是對照組的3 倍,差異有統計學意義( P <0.05)。說明共管模式可更快穩定老年股骨粗隆間骨折患者的病情、使更多患者及早獲得手術治療。這可能與共管模式減少了因等待會診造成的術前等待時間延長、并可及時處理患者的病情變化等原因相關。Traven SA 等研究發現隨著 mFI-5得分升高,老年髖部骨折術后并發癥發生率及死亡率提高 [20]。本文共管組患者 mFI-5得分明顯高于對照組,但術后并發癥發生率(21.82%)明顯低于對照組(40.54%),術后半年內死亡率(7.27%)明顯低于對照組(20.27%)。說明共管模式可顯著減少老年股骨粗隆間骨折患者術后并發癥、術后半年內死亡等不良事件的發生。這可能與共管模式下對患者進行綜合診治,尤其是與老年科醫生在治療內科疾病方面的優勢、對患者及家屬進行全面的健康教育、定期進行隨訪并指導治療等相關。
近年來關于老年科- 骨科共管模式對老年髖部骨折的影響的研究較多,但很少有單獨針對老年股骨粗隆間骨折的研究。Moyet 等[11-12]發現成立老年科- 骨科共管病房可降低老年髖部骨折患者病死率、提高手術治療效果,姜駱永等[13-14]研究發現老年科- 骨科共管模式可縮短患者術前等待時間、降低術后并發癥發生率和30 d 內死亡率。本研究結果與上述結果一致,且研究對象為老年股骨粗隆間骨折患者,針對性更強、觀察時間更長。
本研究存在以下不足:首先這是一項回顧性研究,其次納入的病例數偏少,上述原因可能會使研究結果造成一定的偏倚。但本研究仍可說明老年科 -骨科共管模式可提高老年股骨粗隆間骨折患者48 h 內手術率,降低術后并發癥發生率和術后半年內病死率,提高手術治療效果。
[參考文獻]
[1] Turner G,Clegg A.Best Practice guidelines for themanagement of frailty: a British Geriatrics Society, Age UK and Royal College of General Practitioners report[J]. Age Ageing,2014,43(6):744-747.
[2] Choi JY,Cho KJ,Kim SW,et al.Prediction ofMortality and Postoperative Complications by Hip- Multidimensional Frailty Score in Hip Fracture Elderly Patients[J].Journal of the American Geriatrics Society,2016(64):S277-S278.
[3] Takauji S,Hifumi T,Saijo Y,et al.Associationbetween frailty and mortality among patients with accidental hypothermia: a nationwide observational study in Japan[J].BMC geriatrics,2021,21(1):507.
[4] Sia TY,Wen T,Cham S,et al.The effect of frailty onpostoperative readmissions, morbidity, and mortality in endometrial cancer surgery[J].Gynecol Oncol,2021,161(2):353-360.
[5] Jin X,Ren Y,Shao L,et al.Prevalence of frailty andprediction of mortality in Chinese cancer patients using a frailty index-based clinical algorithm-A multicentre study[J].Cancer Med,2021,10(18):6207-6217.
[6] Pierce KE,Naessig S,Kummer N,et al.The Five-item Modified Frailty Index is Predictive of 30-day Postoperative Complications in Patients Undergoing Spine Surgery[J].Spine,2021,46(14):939-943.
[7] Khalafallah AM,Shah PP,Huq S,et al.The 5-factormodified frailty index predicts health burden following surgery for pituitary adenomas[J].Pituitary,2020,23(6):630-640.
[8] Tracy BM, Wilson JM, Smith RN, et al.The 5-ItemModified Frailty Index Predicts Adverse Outcomes in Trauma[J].Journal of Surgical Research,2020(253):167-172.
[9] Luo J,Carter GC,Agarwal JP,et al.The 5-FactorModified Frailty Index as a Predictor of 30-day Complications in Pressure Ulcer Repair[J].J Surg Res,2021(265):21-26.
[10]? Lachance,Morin S,Vasilevsky N,et al.Validayion ofa 5-Item modified fratlty index for patients undergoing colorectal cancer surgery using the acs-nsqip database[J].Diseases of the Colon & Rectum,2018,61(5):E259-E260.
[11]? Moyet J,Deschasse G,Marquant B,et al.Which isthe optimal orthogeriatric care model to prevent mortality of elderly subjects post hip fractures? A systematic review and meta-analysis based on current clinical practice[J].International Orthopaedics,2018,43(6):1449-1454.
[12]? Prestmo? A,Hagen G,Sletvold O,et al.Comprehensive geriatric care for patients with hip fractures: a prospective, randomised, controlled trial[J]. Lancet,2015,385(9978):1623-1633.
[13]? 姜駱永,孫煒,黃曉陽,等. 多學科診療模式對老年髖部骨折患者術后30 d 死亡率和術后并發癥的影響 [J].中華創傷骨科雜志,2020,22(9):777-782.
[14]? 吳新寶,楊明輝,張萍,等 .老年病科和骨科共管模式縮短老年髖部骨折患者術前等待時間和住院時間 [J].骨科臨床與研究雜志,2017,2(2):96-100.
[15]? Joeris A,Hurtado-Chong A,Hess D,et al.Evaluationof the geriatric co-management for patients with fragility fractures of the proximal femur (Geriatric Fracture Centre (GFC) concept): protocol for a prospective multicentrecohort study[J].BMJ Open,2017,7(7):e014795.
[16]? Subramaniam S,Aalberg JJ,Soriano RP,et al.New5-Factor Modified Frailty Index Using American College of Surgeons NSQIP Data[J].Journal of the American College of Surgeons,2018,226(2):173-181.
[17]? Sasabuchi Y,Matsui H,Lefor AK,et al.Timing ofsurgery for hip fractures in the elderly: A retrospective cohort study[J].Injury,2018,49(10):1848-1854.
[18]? 中華醫學會骨科學分會骨質疏松學組. 骨質疏松性骨折診療指南[J].中華骨科雜志,2017,37(1):1-10.
[19]? Lems WF,Dreinh?fer KE,Bischoff-Ferrari H,et al.EULAR/EFORT recommendations for management of patients older than 50 years with a fragility fracture and prevention of subsequent fractures[J].British Medical Journal (Clinical research ed.),2017,76(5):802-810.
[20]? Traven SA, Reeves RA,Althoff AD,et al.NewFive-Factor Modified Frailty Index Predicts Morbidity and Mortality in Geriatric Hip Fractures[J].Journal of Orthopaedic Trauma,2019,33(7):319-323.
(收稿日期:2021-10-10)
猜你喜歡
保健醫苑(2022年1期)2022-08-30 08:40:44
保健醫苑(2022年6期)2022-07-08 01:25:16
保健醫苑(2022年4期)2022-05-05 06:11:20
海峽姐妹(2018年1期)2018-04-12 06:44:24
中外醫學研究(2016年26期)2016-11-30 03:19:32
中國現代醫生(2016年26期)2016-11-28 02:18:52
今日健康(2016年12期)2016-11-17 11:38:30
科技視界(2016年18期)2016-11-03 21:58:33
中國實用醫藥(2016年24期)2016-10-17 05:58:58
中國實用醫藥(2016年24期)2016-10-17 04:26:41
