Heel pain caused by os subcalcis: A case report
2022-06-28 04:16:48SaijlafuSuoYuanLiXiaoYuZhiQiangLiGuangYangJingHuanLvGuangXiangChenRenJieXu
World Journal of Clinical Cases 2022年16期
INTRODUCTION
The accessory bones usually originate from nonunion of the secondary ossification center adjacent to the main bone mass[1,2]. They are common bone variations around the feet and ankles and remain mostly asymptomatic[3]. Os subcalcis is an accessory bone at the plantar aspect of the calcaneus, which is located just posterior to the insertion of the plantar fascia[4]. Focal bone formation at the calcaneal plantar pole has rarely been reported. We here report a case of bone formation of the plantar calcaneus in a man.
CASE PRESENTATION
Chief complaints
A 55-year-old man presented to our clinic with left plantar heel pain and a progressive swelling for 8 years.
History of present illness
Eight years previously, he felt pain in his left heel, especially when standing and walking, and a progressive swelling of the heel. Three years ago, he received a local blockage in the left heel, which temporarily relieved his pain. In recent two months, the pain was aggravated and affected his walking. He denied any previous trauma to the left heel.
劉雁衡與他對(duì)視一番,冷笑了一下,才說:“你用心再多,辦事再仔細(xì),怕只怕你這番苦心,最終要?dú)г谀切┎粻帤獾牟肯率掷铩!?/p>
History of past illness
After the patient was hospitalized, the preoperative examination identified diabetes which the patient was unaware of. Following drug treatment, the patient’s blood sugar has been well controlled.
Personal and family history
The authors declare noting to disclose.
Physical examination
Physical examination showed that the callosity was approximately 3 cm in diameter, and could be seen at the bottom of the left heel (Figure 1).
Laboratory examinations
2.3.1 暴露術(shù)野 常規(guī)整理好器械臺(tái),清點(diǎn)器械、紗布、縫針,消毒鋪單。固定好電刀、吸引器將其放置在醫(yī)師方便取用的位置,防止滑落。正確連接自體血回輸裝置。暴露后部脊柱結(jié)構(gòu)后,根據(jù)術(shù)前制訂的手術(shù)策略,沿棘突連線切開皮膚,剝離椎旁肌,充分顯露兩側(cè)關(guān)節(jié)突關(guān)節(jié)。
Imaging examinations
X-ray, computer tomography and magnetic resonance imaging (MRI) showed a large os subcalcison the plantar side of the calcaneus, located at the insertion of the plantar fascia (Figure 2). The accessory bone was in the shape of an inverted pyramid, about 35 mm × 35 mm × 25 mm in size.
FINAL DIAGNOSIS
The final diagnosis was large os subcalcis on the plantar side of left calcaneus.


TREATMENT
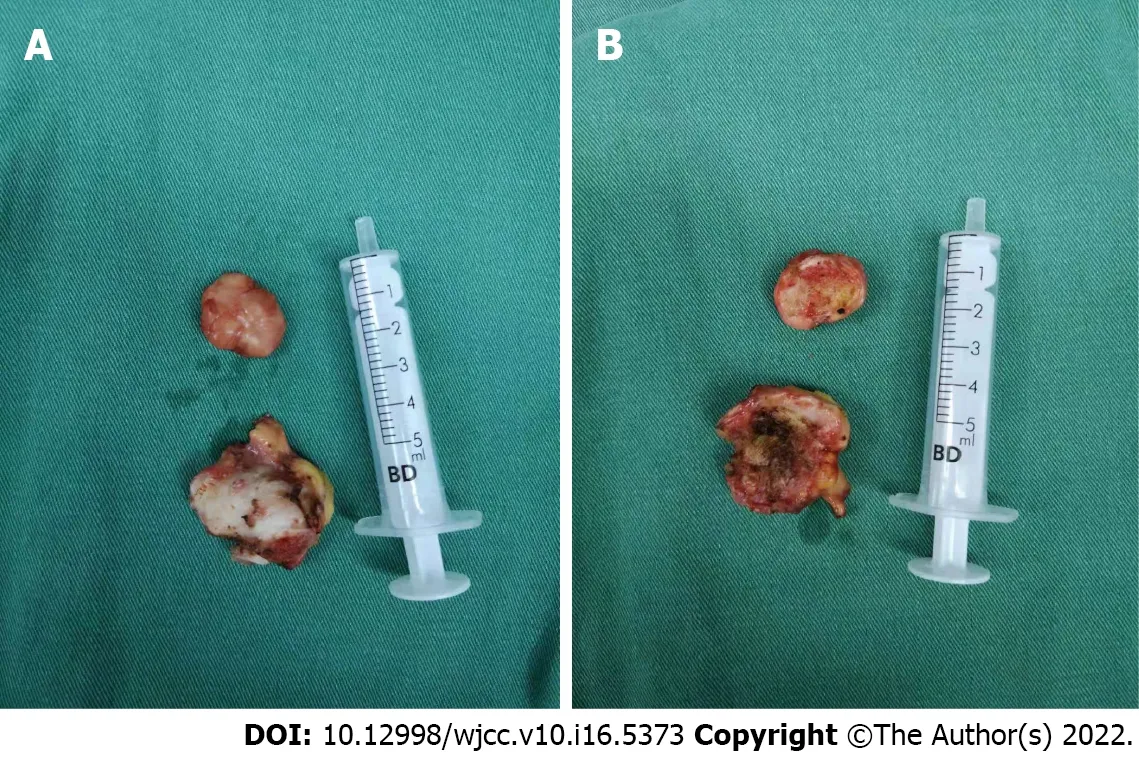
The large os subcalcis was excised under spinal anesthesia in the prone position. The left leg and foot were prepared using Anerdian. The skin and subcutaneous tissue were cut layer by layer through a longitudinal spindle incision on the heel bone surface. At the plantar surface of the os subcalcis, a bursa was present. The surrounding fibrous soft tissue was released and the os subcalcis was exposed. Along the surfaces of the neo-arthrosis between the oscalcis and os subcalcis, fibrous tissue and cartilage-like tissues were observed. The os subcalcis and the bursa were completely resected (Figure 3). Following hemostasis, the skin incision was sutured intermittently. The resected os subcalcis was sent for histological examination. Macroscopically, the resected bone was pyramid shaped and measured 35 mm × 35 mm × 25 mm. Microscopically, the bony trabeculae were intermingled with fat and covered with cartilage (Figure 4). Celecoxib was orally administered at 200 mg twice daily after surgery for analgesia.

OUTCOME AND FOLLOW-UP
Plantar heel pain is the most common foot problem, which can be caused by bone, soft tissue, nerve or systemic diseases. Although accurate diagnosis and proper management are important, it is difficult to distinguish the various causes of highly similar symptoms. The bone disorders include calcaneal stress fracture, calcaneal apophysitis, osteomyelitis and inflammatory arthritis. Soft tissue pathology includes fat pad atrophy or contusion, plantar fascia rupture and plantar fasciitis. Neurological factors include the first branch of the lateral plantar nerve, the medial calcaneal branch of the posterior tibial nerve, and S1 radiculopathy, tarsal tunnel syndrome and peripheral neuropathy[5]. There are few reports on plantar heel pain caused by os subcalcis in the literature.
DISCUSSION
The radiography at the first postoperative day demonstrated that the os subcalcis was completely resected (Figure 5). No weight-bearing on the heel was allowed until the incision healed. At 3 wk after surgery, the heel pain was relieved, and the patient was able to walk freely.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).

Kruse
[6] investigated more than 1200 foot X-ray films from the DuPont Institute in Wilmington, DE, United States, in order to estimate the incidence of accessory bones around the foot and ankle. Cilli
[7] performed anteroposterior and lateral plantar X-rays on 464 male patients in Kayseri, Turkey, to analyze the presence, incidence and distribution of accessory bones. Coskun
[8] investigated 984 foot X-rays from the medical schools of Akdeniz University and Hacettepe University in Turkey to estimate the incidence of accessory bones around the ankle. Longo
[9] investigated the prevalence of accessory ossicles and sesamoid bones in a population of Italian women with hallux valgus. A total of 505 women aged 26 to 80 years at the time of hallux valgus correction were examined. Udoaka
[10] conducted a study of 520 radiographs in Nigeria to ascertain the prevalence of sesamoidbones. Koo
[11]retrospectively reviewed foot images of 213 patients taken at a tertiary hospital in Seoul, Korea. Neither these investigations nor some reviews mentioned os subcalcis[3,12-14].
We found a very few case reports of os subcalcis in the literature. Milliken[4] was the first to describe os subcalcis in the literature. In 1937, a 65-year-old farmer with a small bony structure on the plantar side of the calcaneus was described. The ossicle was removed, and the histological examination demonstrated a spongy bone covered with cartilage, with well-oriented trabecula. Varounis
[15] reported an 11-year-old female who presented with a bony mass separate from the posterior portion of the calcaneus. Clinically, the os subcalcaneum displayed a syndesmotic attachment to the calcaneus. Husebye
[16] presented the case of a 72-year-old female with a volume-expanding os subcalcis. Histological examination demonstrated that cartilage covered the surface of os subcalcis with endochondral ossification between the cancellous bone and the cartilage. Combined with the above reports[4,15,16], we believe that the surgical indications of os subcalcis are: (1) progressive enlargement of the heel mass; (2) significant heel pain or walking instability caused by the heel mass; and (3) broken heel skin caused by the heel mass.
Imaging plays a crucial role in the diagnosis of plantar subcalcis. Among imaging tests, MRI can clearly reveal the cartilage covered surface of os subcalcis, trabecular bone structure and the well demarcated and formed cortical findings[17]. MRI helps us in differential diagnosis with heterotopic ossification, ectopic calcification, osteochondroma[18], periosteal osteosarcoma[19]. In addition, ultrasonography performed with high-resolution broadband linear-array probes due to low cost, fast, readily available, and free of ionizing radiation. It is becoming increasingly important in the evaluation of the ligaments around the ankle joint. Ultrasound has an additional role in the first level differential diagnosis of ankle and heel pain as well as in detection of accessory bones[20,21]. The use of a gel standoff pad can detect otherwise-missed peri- or intra-lesional flow signals on Doppler imaging, increasing the diagnostic role of this technique in differential diagnosis of heel pain[22].
CONCLUSION
We report a rare case of a patient with accessory os subcalcis leading to heel pain. The accessory os subcalcis was completely excised, and the heel pain disappeared after surgery. This case report may improve the orthopedic awareness of os subcalcis and help avoid future misdiagnosis of heel pain.
FOOTNOTES
Saijilafu and Li SY contributed equally to this work. Saijilafu and Li SY conducted all integrated data, edited the figures and wrote the manuscript; Yu X and Li ZQ critically reviewed the manuscript; Yang G and Lv JH performed the pathological examination; Chen GX and Xu RJ supervised the study and provided advice; Chen GX and Xu RJ contributed equally to this work; All authors read and approved the final manuscript.
The Gusu Talents Project, No. GSWS2020069.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
普通高等院校開設(shè)的健美操普修課程是以健身鍛煉為目的、體現(xiàn)健與美的課程。健美操對(duì)培養(yǎng)學(xué)生良好身體姿態(tài),身體協(xié)調(diào)能力、審美能力以及增強(qiáng)體質(zhì)都起到很好的促進(jìn)作用。于上世紀(jì)80年代中期引入體育課堂的健美操,雖發(fā)展歷程較短,但它以自身的獨(dú)特性迅速受到廣大學(xué)生的喜愛和歡迎。現(xiàn)今,河南省雖有不少高校開設(shè)了健美操普修課程,但也存在諸多問題,教學(xué)質(zhì)量并不如預(yù)期規(guī)劃的好,基于此種現(xiàn)象,提出具有針對(duì)性的對(duì)策,為優(yōu)化河南省高校健美操普修課程提供有力依據(jù)。
2.1 兩組AECOPD患者血?dú)鈾z查結(jié)果 兩組AECOPD 患者血?dú)庵当容^,Pa02、PaCO2、pH 均有統(tǒng)計(jì)學(xué)差異,且患者病情與Pa02呈負(fù)相關(guān),與PaCO2、PH 呈正相關(guān),見表 1。
The patient had unremarkable personal and familial medical history, including psycho-social history.
The accessory bones usually originate from nonunion of the secondary ossification center adjacent to the main bone mass. They are common bone variations around the feet and ankles. The percentage of adult feet with accessory bones ranges from 18% to 30%.
All study participants provided informed written consent prior to study enrollment.
His red blood cell count, hemoglobin, white blood cell, white blood cell differential count, platelet, Creactive protein, erythrocyte sedimentation rate, rheumatoid factor and uric acid test results were within normal limits.
有醫(yī)生坦言,自己在診療過程中,針對(duì)熟人介紹的病人,可能礙于情面放棄疾病所需的常規(guī)檢查,而主要憑借自己經(jīng)驗(yàn)做判斷,比如本來該拍X光片的,熟人帶著透視一下就行了,錢省了,重要的診斷證據(jù)卻沒留下;在用藥方面,也會(huì)想辦法找便宜但質(zhì)量相對(duì)欠缺的藥品替代;至于看病不寫病歷的情況就更普遍了。這就是導(dǎo)致不少正常的就醫(yī)程序被簡化,不規(guī)范醫(yī)療情況出現(xiàn),一旦出現(xiàn)醫(yī)療糾紛,患者往往會(huì)礙于情面吃啞巴虧或難以舉證,給維護(hù)自己的合法權(quán)益帶來了困難,最終受害的還是患者。
China
Saijilafu 0000-0003-2290-9808; Suo-Yuan Li 0000-0003-1414-6847; Xiao Yu 0000-0003-2522-2251; Zhi-Qiang Li 0000-0003-4229-2171; Guang Yang 0000-0001-7379-6810; Jing-Huan Lv 0000-0003-1746-420X; Guang-Xiang Chen 0000-0001-7174-9519; Ren-Jie Xu 0000-0002-6147-2453.
Pei,W.(2000:29-31,87,179-181)also suggests six functions of context,that is,demonstrative function;extensive function;acceptive and rejective function;restrictive function;absolute function;interpretive function.
Chang KL
A
其中,上海 ·中駿世界城項(xiàng)目總用地面積100512.8 0m2,擬建總建筑面積458988.89m2,地上主要設(shè)置高層辦公、多層辦公及商業(yè)街,地下包含停車庫下沉廣場及地下商業(yè)步行街等功能。項(xiàng)目擬采用透水地面、雨水回收、活動(dòng)外遮陽、蓄熱蓄冷技術(shù)等多種綠色技術(shù),并于方案階段采用綠色建筑系列軟件進(jìn)行項(xiàng)目室內(nèi)外風(fēng)、光、熱環(huán)境的模擬計(jì)算,通過主被動(dòng)結(jié)合方式達(dá)到高星級(jí)綠色建筑認(rèn)證要求。
Chang KL
1 O'Rourke J, Stone P, Stern M, McGarry J. Accessory bone or unusual congenital anomaly. J Am Podiatr Med Assoc 1997 ;87 : 407 -413 [PMID: 9308307 DOI: 10 .7547 /87507315 -87 -9 -407 ]
2 Vaz A, Trippia CR. Small but troublesome: accessory ossicles with clinical significance. Radiol Bras 2018 ; 51 : 248 -256[PMID: 30202129 DOI: 10 .1590 /0100 -3984 .2017 .0147 ]
3 Mellado JM, Ramos A, Salvadó E, Camins A, Danús M, Saurí A. Accessory ossicles and sesamoid bones of the ankle and foot: imaging findings, clinical significance and differential diagnosis.
2003 ; L164 [DOI:10 .1007 /s00330 -003 -2011 -8 ]
4 Milliken RA. Os subcalcis. Am J Surg 1937 ; 116 [DOI: 10 .1016 /s0002 -9610 (37 )90875 -4 ]
5 Yi TI, Lee GE, Seo IS, Huh WS, Yoon TH, Kim BR. Clinical characteristics of the causes of plantar heel pain.
2011 ; 35 : 507 -513 [PMID: 22506166 DOI: 10 .5535 /arm.2011 .35 .4 .507 ]
6 Kruse RW, Chen J. Accessory bones of the foot: clinical significance. Mil Med 1995 ; 160 : 464 -467 [PMID: 7478033 DOI:10 .1093 /milmed/160 .9 .464 ]
7 Beytemür O, ?ncü M. The age dependent change in the incidence of calcaneal spur. Acta Orthop Traumatol Turc 2018 ;52 : 367 -371 [PMID: 30170885 DOI: 10 .1016 /j.aott.2018 .06 .013 ]
8 Coskun N, Yuksel M, Cevener M, Arican RY, Ozdemir H, Bircan O, Sindel T, Ilgi S, Sindel M. Incidence of accessory ossicles and sesamoid bones in the feet: a radiographic study of the Turkish subjects.
2009 ; 31 : 19 -24[PMID: 18633564 DOI: 10 .1007 /s00276 -008 -0383 -9 ]
9 Longo UG, Marinozzi A, Petrillo S, Spiezia F, Maffulli N, Denaro V. Prevalence of accessory ossicles and sesamoid bones in hallux valgus.
2013 ; 103 : 208 -212 [PMID: 23697726 DOI: 10 .7547 /1030208 ]
10 Udoaka AI, Didia BC. Prevalence and types of accessory ossicles and sesamoid bones of the feet of adult Southern Nigerians.
2013 ; 25 [DOI: 10 .3923 /rjmsci.2013 .25 .27 ]
11 Koo BS, Song Y, Lee S, Sung YK, Sung IH, Jun JB. Prevalence and distribution of sesamoid bones and accessory ossicles of the foot as determined by digital tomosynthesis.
2017 ; 30 : 1072 -1076 [PMID: 28714106 DOI:10 .1002 /ca.22952 ]
12 Keles-Celik N, Kose O, Sekerci R, Aytac G, Turan A, Güler F. Accessory Ossicles of the Foot and Ankle: Disorders and a Review of the Literature.
2017 ; 9 : e1881 [PMID: 29387510 DOI: 10 .7759 /cureus.1881 ]
13 Nwawka OK, Hayashi D, Diaz LE, Goud AR, Arndt WF, 3 rd, Roemer FW, Malguria N, Guermazi A. Sesamoids and accessory ossicles of the foot: anatomical variability and related pathology.
2013 ; 581 [DOI:10 .1007 /s13244 -013 -0277 -1 ]
14 Vora BMK, Wong BSS. Common accessory ossicles of the foot: imaging features, pitfalls and associated pathology.
2018 ; 59 : 183 -189 [PMID: 29749423 DOI: 10 .11622 /smedj.2018046 ]
15 Varounis G, Pasternack WA. Os subcalcaneum. J Am Podiatr Med Assoc 1989 ; 79 : 517 -518 [PMID: 2585284 DOI:10 .7547 /87507315 -79 -10 -517 ]
16 Husebye EE, St?dle A, Lund-Iversen M, Hvaal K. Unilateral, Volume-expanding Os Subcalcis: Patient History and Treatment: A Case Report.
2021 ; 60 : 209 -212 [PMID: 33168442 DOI: 10 .1053 /j.jfas.2020 .09 .006 ]
17 Lucas P, Kaplan P, Dussault R, Hurwitz S. MRI of the foot and ankle. Curr Probl Diagn Rad 1997 ; 209 [DOI:10 .1016 /s0363 -0188 (97 )90015 -3 ]
18 Jung HG, Carag JA, Park JY, Bae EJ, Lim SD, Kim HS. Osteochondroma of the calcaneus presenting as Haglund's deformity.
2011 ; 17 : e20 -e22 [PMID: 21549965 DOI: 10 .1016 /j.fas.2010 .08 .007 ]
19 Singh D, Sen R, Chaudhary S, Tripathy SK. Periosteal osteosarcoma of the calcaneum: a case report.
2012 ; 5 : 121 -123 [PMID: 22343818 DOI: 10 .1177 /1938640011434510 ]
20 Fessell DP, Vanderschueren GM, Jacobson JA, Ceulemans RY, Prasad A, Craig JG, Bouffard JA, Shirazi KK, van Holsbeeck MT. US of the ankle: technique, anatomy, and diagnosis of pathologic conditions.
1998 ; 18 : 325 -340 [PMID: 9536481 DOI: 10 .1148 /radiographics.18 .2 .9536481 ]
21 Sconfienza LM, Orlandi D, Lacelli F, Serafini G, Silvestri E. Dynamic high-resolution US of ankle and midfoot ligaments:normal anatomic structure and imaging technique.
2015 ; 35 : 164 -178 [PMID: 25590396 DOI:10 .1148 /rg.351130139 ]
22 Corvino A, Sandomenico F, Corvino F, Campanino MR, Verde F, Giurazza F, Tafuri D, Catalano O. Utility of a gel standoff pad in the detection of Doppler signal on focal nodular lesions of the skin.
2020 ; 23 : 45 -53 [PMID:30927249 DOI: 10 .1007 /s40477 -019 -00376 -3 ]
猜你喜歡
品牌研究(2022年29期)2022-10-15 08:01:00
品牌研究(2022年26期)2022-09-19 05:54:46
品牌研究(2021年35期)2022-01-18 08:45:18
云南化工(2021年6期)2021-12-21 07:31:42
內(nèi)蒙古教育(2021年20期)2021-03-08 01:09:14
計(jì)算機(jī)教育(2020年5期)2020-07-24 08:53:38
家庭影院技術(shù)(2019年11期)2019-12-09 09:14:30
海峽姐妹(2019年3期)2019-06-18 10:37:10
教育與職業(yè)(2014年1期)2014-04-17 14:28:07
百科知識(shí)(2008年8期)2008-05-15 09:53:30
 World Journal of Clinical Cases2022年16期
World Journal of Clinical Cases2022年16期
- World Journal of Clinical Cases的其它文章
- Practical points that gastrointestinal fellows should know in management of COVID-19
- Electroconvulsive therapy plays an irreplaceable role in treatment of major depressive disorder
- Pleural involvement in cryptococcal infection
- Advances in the clinical application of oxycodone in the perioperative period
- Endoscopic surgery for intraventricular hemorrhage: A comparative study and single center surgical experience
- Pediatric acute myeloid leukemia patients with i(17)(q10) mimicking acute promyelocytic leukemia: Two case reports