轉移性前列腺癌伴惡性腹水一例報道
2023-06-20 05:52:09任尚青歐勇李安呂倩鐘山周放范世達陳正軍馮華林王強羅鋮聶鈺何軍嫻王東
機器人外科學 2023年2期
關鍵詞:前列腺癌
任尚青 歐勇 李安 呂倩 鐘山 周放 范世達 陳正軍 馮華林 王強 羅鋮 聶鈺 何軍嫻 王東
摘 要 目前,臨床上伴有胃轉移、腹膜轉移和惡性腹水的晚期前列腺癌很少見,且最佳治療方案尚不清楚。本研究報道了一例伴有膀胱頸受累、盆腔淋巴結浸潤的晚期前列腺癌患者,且腫瘤轉移到骨、胃及腹膜等部位并伴有惡性腹水。前列腺癌腹膜轉移和惡性腹水的預后極差,其主要的治療方法為癥狀支持、腹膜穿刺引流、內分泌治療和化療。本研究通過報道一例伴有腹膜轉移的晚期前列腺癌病例及回顧相關文獻,為伴有惡性腹水的轉移性前列腺癌臨床研究提供參考借鑒。
關鍵詞 前列腺癌;腫瘤轉移;胃;腹膜;腹水
中圖分類號 R697 文獻標識碼 A 文章編號 2096-7721(2022)02-0132-08
Abstract At present, clinically advanced prostate cancer with gastric metastasis, peritoneal metastasis and malignant ascites is rare, and the optimal treatment is unclear. This study reported a case of advanced prostate cancer with bladder neck involvement, pelvic lymph node invasion, and metastasis to bone, stomach, peritoneum with malignant ascites. The prognosis of prostate cancer with peritoneal metastasis and malignant ascites is extremely poor, and the main treatment methods are symptomatic support, peritoneal puncture and drainage, endocrine therapy and chemotherapy. Herein, through a case report of advanced prostate cancer with peritoneal metastasis and the review of relevant literatures, a case of advanced prostate cancer with peritoneal metastasis was reported and relevant literature was reviewed to provide reference for clinical research of metastatic prostate cancer with malignant ascites.
Key words Prostate cancer; Tumor metastasis; Gastric; Peritoneal; Ascites
Prostate cancer is among the most common malignancies in men[1], which poses a significant threat to public health. Worldwide, the incidence of prostate cancer ranks second among all male malignant tumors[2]. With a well-arranged surveillance schedule and local treatment-based management, early-stage prostate cancer usually has a good prognosis, with the 5-year survival rate closing to 90%[3]. At present, most newly diagnosed prostate cancer is locally advanced or extensively metastatic, and the patients cannot receive local radical treatment in China[4]. The most common metastatic sites of metastatic prostate cancer are pelvic lymph nodes and bone, whereas tumor metastasis is uncommon to the stomach, peritoneum, and is not frequently accompanied by malignant ascites. The patients family gave consent to these studies and publication, and this report was approved by the Ethics committee of Sichuan Academy of Medical Sciences & Sichuan Provincial Peoples Hospital.
1 Case presentation
A 57-year-old male presented to the Department of Robotic Minimally Invasive Surgery Center complaining of frequent urination, urgency and dysuria, and the patient underwent transurethral resection of the prostate in July 2014. The postoperative pathological diagnosis revealed prostate adenocarcinoma (Gleason score 5+3=8). The patient underwent laparoscopic radical prostatectomy after one years combined androgen blockade (Bicalutamide+Goserelin), the definitive pathology report revealed prostate adenocarcinoma with a Gleason score of 5+4=9, and postoperative endocrine therapy was continued.
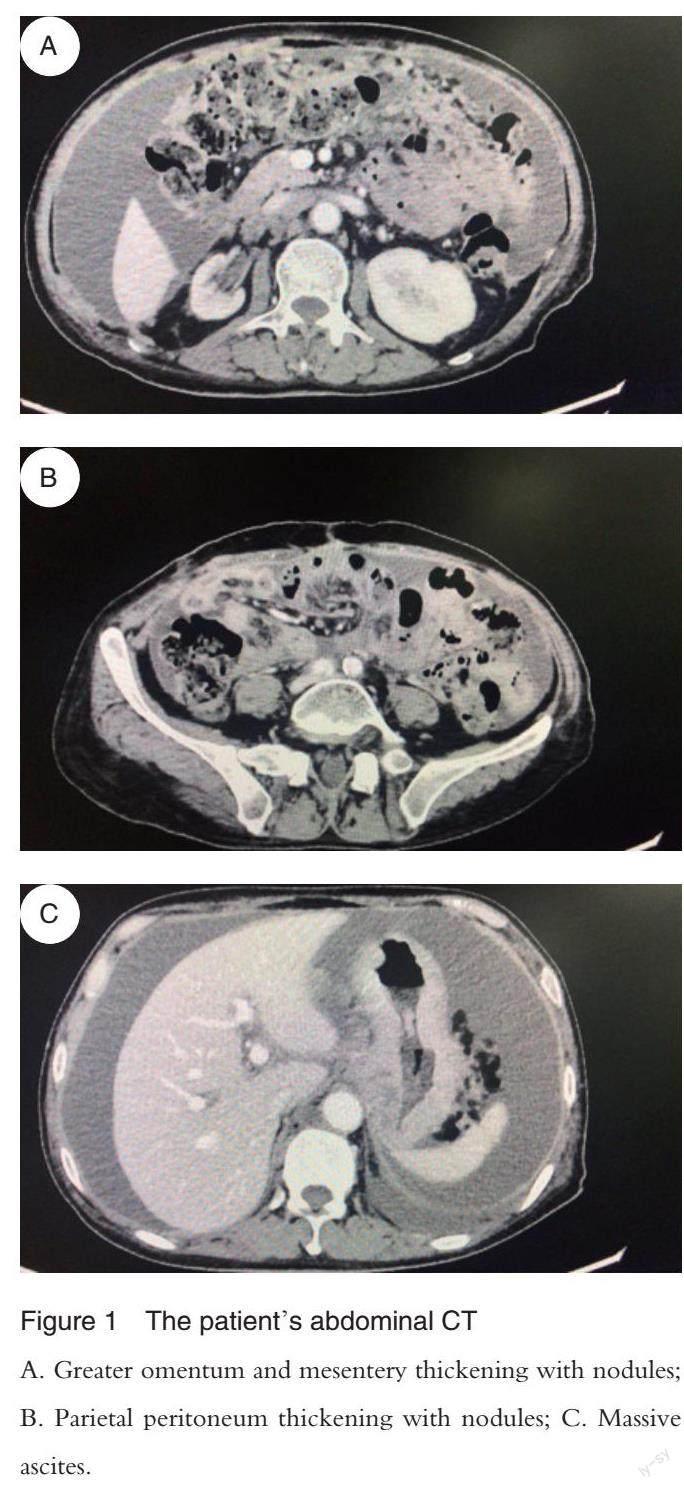
During the follow-up visit in February 2016, the patient underwent ultrasound examination and a mass was found in the bladder. The initial biopsy findings of the urinary bladder mass indicated poor differentiated carcinoma, and the transurethral resection of bladder tumor was performed. The postoperative pathological diagnosis revealed prostate adenocarcinoma metastasis. Subsequently, pelvic radiotherapy stereotactic body radiation therapy (SBRT) was performed for 36 times from May 2016 to June 2016, and regular follow-up was made. In June 2017, the patient was admitted to the hospital again due to abdominal distention. The CT examination showed a large amount of fluid in the abdominal cavity; The gastric wall of the cardia and the lesser curvature of the stomach was thickened and heterogeneous; The enlarged lymph node was identified in the abdominal cavity and retroperitoneum; Metastatic lesions were also found in multiple thoracic, lumbar, and sacral
vertebrae (Figure 1). The operator repeated peritoneal drainage to collect pale yellow ascites, which were identified as abnormal cells that tended to be poorly differentiated cancer cells. The operator used docetaxel+prednisone chemotherapy and zoledronic acid for the prevention of bone related adverse events in the first phase of treatment, and the symptoms of abdominal distension were relieved and the patients condition improved after one stage of treatment. In addition, chemotherapy (docetaxel+prednisone+cisplatin) from the second phase to the fourth phase was completed from July 2017 to November 2017, with the addition of bevacizumab in the fourth phase. A gastroscopy was performed in December 2017, and multiple grayish neoplasms were observed in the bottom of the stomach and duodenal bulb. Immunohistochemistry of the biopsy showed pan-cytokeratin (PCK)(+), the epithelial membrane antigen(EMA) (+) and
creatine kinase 7(CK7) (individual+), prostate specific antigen (PSA) (focal+), prosaposin (PSAP) (individual+), androgen receptor (AR) (+) and CK20 (+), cluster of differentiation 56 (CD56)(+), caudal-relatedhome-odomain transcription 2 (CDX-2) (-), paired box gene 8 (PAX-8) (-), which were considered as poorly differentiated prostate adenocarcinoma. Since then, the patient experienced multiple episodes of abdominal bloating exacerbation, accompanied by chest tightness and dyspnea. The patient eventually died of acute pulmonary edema in January 2018.
2 Discussion
The clinical manifestations of prostate cancer are various because it can metastasize to nearly every organ. In 1948, Arnheim first described the catalog of metastatic sites in patients with prostate cancer in a study of the autopsy results of 176 cases. The study founded the most common sites of metastasis of prostate cancer were bone, lymph nodes and lung. Rare metastases include adrenal glands, kidneys, brain, pancreas, genitals and breasts, malignant ascites or pleural effusion is extremely rare[5].
In 2000, Bubendorf L et al. had reported 1 589 cases of prostate cancer suggested that 35% of the patients had blood-derived metastases, with the most common metastases in the bone (90%) and the less common metastases in the lungs (46%), liver (25%), pleura (21%) and adrenal gland (13%)[6]. Skin, optic nerve, mandible, testicle, penis, pituitary gland, thyroid gland and salivary gland are some rare sites reported in the literature.
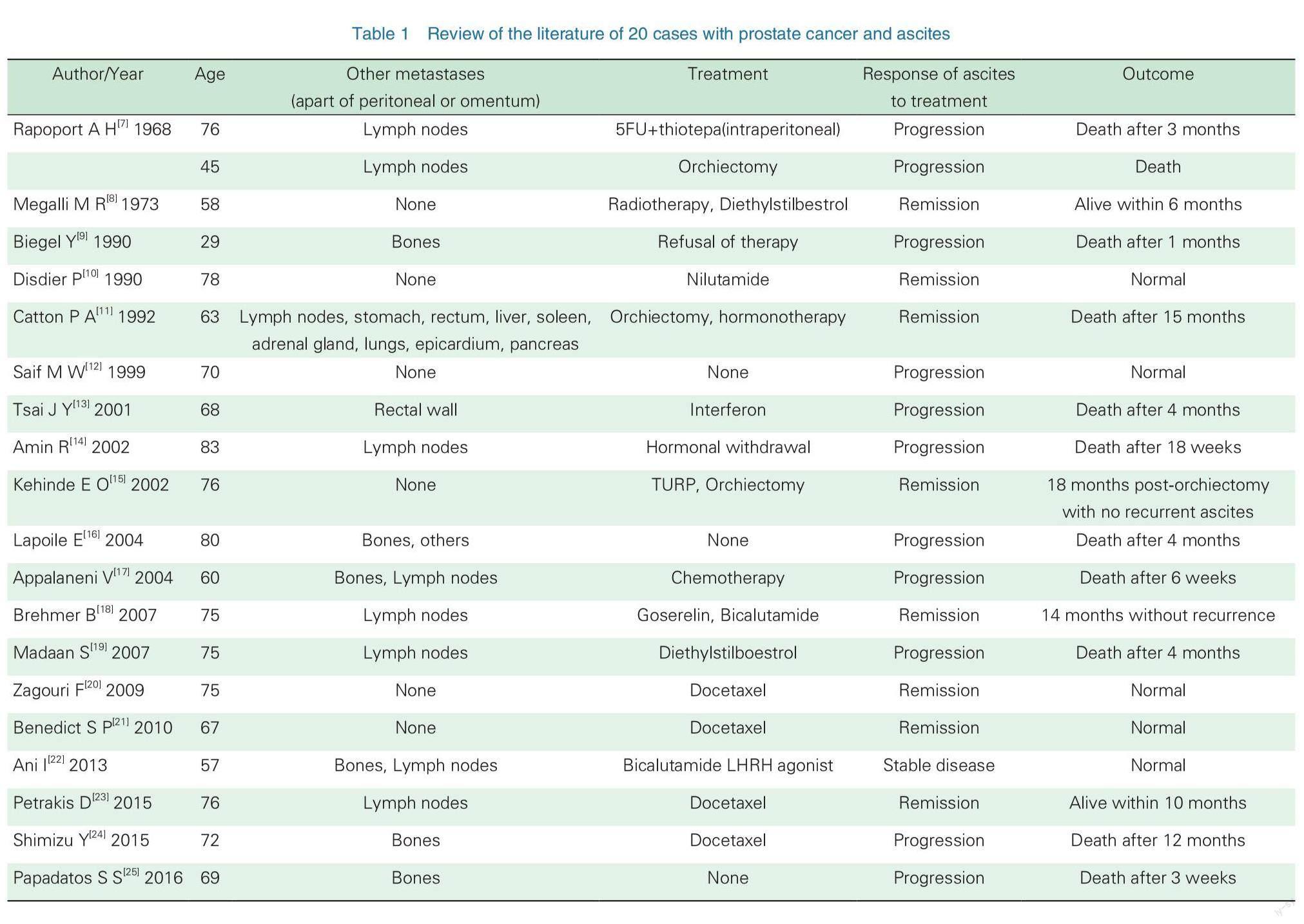
Peritoneal metastasis of prostate cancer with malignant ascites is rare, and only 20 cases have been reported in literatures[7-25] (Table 1). The age of the patients ranged from 29 to 83 years, and most of them had high-risk prostate cancer, with 6 cases of bone metastasis, 6 cases of lymph node metastasis, 1 case of rectal wall metastasis, 1 case of multiple visceral metastasis and 6 cases without other metastases (apart of peritoneal or omentum). Ascites was the first symptom in some patients, while the rest of the patients with ascites 1 to 16 years after the initial diagnosis. Among them, 3 cases presented with chylous ascites[9,14,24], 1 case presented hemorrhagic ascites[13], and the rest presented exudative ascites. 14 out of 20 cases received endocrine therapy or chemotherapy, and a total of 8 cases had responses, 5 cases responded to endocrine therapy, and 3 cases responded to chemotherapy. Responders lived for up to 18 months, while non-responders died within 1-4 months.
Gastric metastasis of prostate cancer is less common, and only a few reports suggest that metastatic prostate cancer affects the stomach[26-34]. Most patients have varying degrees of upper gastrointestinal tract symptoms, such as nausea, vomiting, hematemesis and so on. On some occasions, the symptoms relieved in response to endocrine therapy or chemotherapy, but most patients had poor prognosis.
The pathogenesis of prostate cancer with ascites is still unclear, and the invasion of tumor cells into mesothelium is considered to be the main cause of peritoneal effusion. Rapoport A H et al.[7] found that 13 of 523 cases of prostate cancer had peritoneal metastasis with peritoneal effusion, but no other metastases. However, studies of
Broghamer W L Jr et al.[35]? suggest that prostate cancer with ascites may be caused by metastasis or reactive diseases, such as pancreatic cancer, lung cancer and gastric cancer. Megalli M R et al.[36] pointed out that ascites of prostate cancer can also be caused by second primary malignant tumors, of which gastrointestinal malignant tumors are the most common. Three cases of chylous ascites with diffuse lymph node metastasis had also been reported, which may be due to lymphatic hyperemia caused by a large number of cancer cells, resulting in chylous thorax and chylous ascites[9, 14, 24].
It is crucial to judge the nature and etiology of ascites in these patients. Ascites may have multiple causes, it is necessary to distinguish metastatic ascites from ascites caused by other benign or malignant diseases, especially ascites caused by gastrointestinal tumors. Ascites exfoliated cells immunohistochemical staining, prostatic acid phosphatase, and prostate-specific antigen as specific markers can be used as an essential tool to identify malignant effusion[12]. Peroxidase-antiperoxidase (PAP)
immunohistochemical staining has specificity and sensitivity. PAP is positive in more than 95% of prostatic tissues and weak positive in about 3% of non-prostatic tissues, and PSA may also exist in anaplastic tumor cells with low PAP activity[28]. The combination of PSA and PAP improves the sensitivity of diagnosis of prostate metastases. Therefore, the detection of ascites specific markers and the application of exfoliated cell immunohistochemical staining are helpful to differentiate ascites.
Abdominal distension, abdominal pain, and respiratory distress can be alleviated through ascites management, diet, diuresis, puncture, and drainage. Some patients may be relieved by endocrine therapy or chemotherapy. These therapies may prolong life expectancy and improve the quality of life. However, the prognosis is poor, and most patients die within weeks to months.
In this study, the patient presented similar clinical manifestations. Ascites occurred three years after the diagnosis of prostate cancer. During this period, the patient received endocrine therapy. The presence of peritoneal metastasis, multiple lymph node metastasis, bone metastasis and gastric metastasis in the patient was confirmed by CT, ascites exfoliative cytology and gastroscopic biopsy. After the diagnosis of ascites, the patient underwent abdominal puncture and drainage, and was treated with docetaxel, cisplatin, and bevacizumab. However, the patient died of acute pulmonary edema in January 2018.
3 Conclusion
The prognosis of prostate cancer with peritoneal metastasis and malignant ascites is extremely poor. The main treatment modalities of this patient were symptomatic and supportive care, peritoneal puncture and drainage, endocrine therapy, radiotherapy and chemotherapy, etc. Patient distress could be relieved and patients life be prolonged by these therapies. However, gastric and peritoneal metastatic prostate cancer is uncommon in clinical practice, and its treatment needs to be further optimized and explored.
Declaration
Availability of data and materials
All the data and material are from the patients assay and examination of Sichuan Academy of Medical Sciences & Sichuan Provincial Peoples Hospital, which are real, credible and for availability.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or
publication of this article.
Authors contributions
REN Shangqing and OU Yong was responsible for writing and editing the article; LI An, ZHONG Shan, ZHOU Fang were responsible for reviewing the literature; LYU Qian, FAN Shida, CHEN Zhengjun, FENG Hualin, WANG Qiang, LUO Cheng, NIE Yu, HE Junxian were responsible for collecting the information of the current case. WANG Dong were responsible for the revision of the manuscript for important intellectual content. All authors have read and approved the manuscript.
Acknowledgements
I would like to show my gratitude to Dr. WANG Dong who has provided me with valuable guidance to this article.
References
[1] Salim E I, Magid A D, Farara K M, et al. Antitumoral and antioxidant potential of egyptian propolis against the pc3 prostate cancer cell line [J]. Asian PacJ Cancer Prey, 2015, 16(17):7641-7651.
[2] Center M M, Jemal A, Lortet-Tieulent J, et al. International variation in prostate cancer incidence and mortality rates [J]. Eur Urol, 2012, 61(6):1079-1092.
[3] Brawley O W, Gansler T. Introducing the 2010 american cancer society prostate cancer screening guideline [J]. CA Cancer J Clin, 2010, 60(2):68-69.
[4] Chen W, Zheng R, Baade P D, et al. Cancer Statistics in China, 2015 [J]. CA Cancer J Clin, 2016, 66(2):
115-132.
[5] Arnheim F K. Carcinoma of the prostate: a study of the post-mortem findings in one hundred and seventy-six cases [J]. J Urol, 1948, 60(4):599-603.
[6] Bubendorf L, Sch?pfer A, Wagner U, et al. Metastatic patterns of prostate cancer: an autopsy study of 1589 patients [J]. Hum Pathol, 2000, 31(5):578-583.
[7] Rapoport A H, Omenn G S. Dermatomyositis and malignant effusions: rare manifestation of cancer [J]. J Urol, 1968, 100(2): 183-187.
[8] Megalli M R, Gursel E O, Veenema R J. Ascites as an unusual presentation of carcinoma of the prostate [J]. J Urol, 1973, 110(2):232-234.
[9] Beigel Y, Zelikovski A, Shimoni S, et al. Chylous ascites as a presenting sign of prostate adenocarcinoma [J]. Lymphology, 1990, 23(4):183-186.
[10] Disdier P, Harle J R, Swiader L,et al. Ascites with cachexia revealing prostatic carcinoma[J]. Presse Med, 1990, 19(5):220.
[11] Catton P A, Hartwick R W, Srigley J R. Prostate cancer presenting with malignant ascites: signet-ring cell variant of prostate adenocarcinoma [J]. Urology, 1992, 39(5):495-497.
[12] Saif M W, Figg W D, Hewitt S, et al. Malignant ascites as only manifestation of metastatic prostate cancer [J]. Prostate Cancer Prostatic Dis, 1999, 2(5/6):290-293.
[13] Tsai J Y, Ling M, Chang V T, et al. Hemorrhagic ascites: an unusual manifestation of prostate carcinoma [J]. Am J Med, 2001, 111(3):245-246.
[14] Amin R. Chylous ascites from prostatic adenocarcinoma [J].?Urology, 2002, 59(5):773.
[15] Kehinde E O, Abdeen S M, Al-Hunayan A, et al. Prostate cancer metastatic to the omentum [J]. Scand J Urol Nephrol, 2002, 36(3):225-227.
[16] Lapoile E, Bella?che G, Choudat L, et al. Ascites associated with prostate cancer metastases:an unusual localization [J]. Gastroenterol Clin Biol, 2004, 28(1):92-94.
[17] Appalaneni V, Yellinedi S, Baumann M A. Diagnosis of malignant ascites in prostate cancer by measurem Jakse Gent of prostate specific antigen [J]. Am J Med Sci, 2004, 327(5):262-263.
[18] Brehmer B, Makris A, Wellmann A. Solitary peritoneal carcinomatosis in prostate cancer [J]. Actuelle Urol, 2007, 38(5):408-409.
[19] Madaan S, Palit V, Gudgeon P, et al. Omental metastasis with malignant ascites: an unusual manifestation of prostatic adenocarcinoma [J]. Can Urol Assoc J, 2007, 1(3):288-290.
[20] Zagouri F, Papaefthimiou M, Chalazonitis A N, et al. Prostate cancer with metastasis to the omentum and massive ascites: a rare manifestation of a common disease [J]. Onkologie, 2009, 32(12):758-761.
[21] Benedict S P, Ahuja M, Mammen K J. Hormone refractory carcinoma of prostate with peritoneal metastases and malignant ascites without skeletal involvement: a case report and review of literature [J]. Indian J Urol, 2010, 26(2): 287-288.
[22] Ani I, Colstaldi M, Abouassaly R. Metastatic prostate cancer with malignant ascites: a case report and literature review [J]. Can Urol Assoc J, 2013, 7(3-4): E248-E250.
[23] Petrakis D, Pentheroudakis G, Kamina S, et al. An unusual presentation of a patient with advanced prostate cancer, massive ascites and peritoneal metastasis: case report and literature review [J]. J Adv Res, 2015, 6(3):517-521.
[24] Shimizu Y, Kanamaru S, Ito N, et al. Simultaneous chylothorax and chylous ascites in a patient with castration-resistant prostate cancer after docetaxel chemotherapy: an unusual manifestation [J]. Int J Urol, 2015, 22(6): 614.
[25] Papadatos S S, Bazoukis G, Deligiannis G, et al. Malignant ascites due to prostatic adenocarcinoma: an extremely rare manifestation of a common disease [J]. J Clin Diagn Res, 2016, 10(11): OL01.
[26] Christoph F, Grünbaum M, Wolkers F, et al. Prostate cancer metastatic to the stomach [J]. Urology, 2004, 63(4): 778-779.
[27] Ben-Izhak O, Lichtig C. Signet-ring cell carcinoma of the prostate mimicking primary gastric carcinoma [J]. J Clin Pathol, 1992, 45(5): 452-454.
[28] Holderman W H, Jacques J M, Blackstone M O, et al.
Prostate cancer metastatic to the stomach: clinical aspects and endoscopic diagnosis [J]. J Clin Gastroenterol, 1992, 14(3):251-254.
[29] Green L K. Hematogenous metastases to the stomach. A review of 67 cases [J]. Cancer, 1990, 65(7): 1596-1600.
[30] Oda I, Kondo H, Yamao T, et al. Metastatic tumors to the stomach: analysis of 54 patients diagnosed at endoscopy and 347 autopsy cases [J]. Endoscopy, 2001, 33(6): 507-510.
[31] Kato M, Hirakawa A, Kobayashi Y Ms, et al. The influence of the presence of intraductal carcinoma of the prostate on the grade group systems prognostic performance [J]. Prostate, 2019, 79(10):1065-1070.
[32] Kemp C. Metastatic spread and common symptoms. Part six: Advanced cancer of the pancreas, prostate, stomach, and uterus [J]. Am J Hosp Palliat Care, 1999, 16(5):673-681.
[33] Aoyama Y, Wato M, Colvin M, et al. A case of metastatic prostate cancer with gastric metastases and high serum CEA [J]. Nihon Shokakibyo Gakkai Zasshi, 2018, 115(9):804-810.
[34] Onitilo A A, Engel J M, Resnick J M. Prostate carcinoma metastatic to the stomach: report of two cases and review of the literature [J]. Clin Med Res, 2010,8(1):18-21.
[35] Broghamer W L Jr, Richardson M E, Faurest S, et al.?PAP immunoperoxidase staining of cytologically positive effusions associate with adenocarcinoma of the prostate and neoplasms of undetermined origin [J]. Acta Cytol, 1985, 29(3):272-278.
[36] Megalli M R, Gursel E O, Veenema R J. Ascites as an unusual presentation of carcinoma of the prostate [J]. J Urol, 1973, 110(2):232-234.
猜你喜歡
基礎醫學與臨床(2022年1期)2022-01-21 05:22:06
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:02
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:02
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:02
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
天津醫科大學學報(2019年3期)2019-08-13 06:53:10
中國生殖健康(2019年7期)2019-01-06 09:27:34