造影劑優維顯對早期急性胰腺炎病情的影響
2012-11-06 06:54:01張敏劉思純馬博廖獻花李初俊
中華胰腺病雜志 2012年1期
張敏 劉思純 馬博 廖獻花 李初俊
·短篇論著·
造影劑優維顯對早期急性胰腺炎病情的影響
張敏 劉思純 馬博 廖獻花 李初俊
增強CT是目前判斷急性胰腺炎(AP)嚴重度最可靠的方法。但是,起病96 h內進行增強CT是否會加重AP病情仍有爭議。針對此問題,本研究對我院AP患者的臨床資料進行了回顧性分析,現報告如下。
一、資料與方法
1.研究對象及分組:收集2005年1月至2008年6月發病96 h內入院的AP患者。診斷符合中華醫學會消化病學分會胰腺病學組制定的指南標準[1]。按發病96 h內是否進行增強CT將病例分為增強CT組和對照組。增強CT造影劑為優維顯-300,CT檢查后沒有使用抗氧化劑預防造影劑不良反應。排除標準:(1)CT檢查前靜脈使用造影劑者;(2)發病96 h后入院者;(3)觀察期內出院或資料欠完善者;(4)合并妊娠者;(5)發病96 h內出現并發癥者。
2.觀察指標:記錄入院時患者性別,年齡,病因,首次APACHEⅡ評分,主要癥狀持續時間,住院時間,有無消化道出血、全身性炎癥反應綜合征(SIRS)、休克、急性腎損傷等癥狀發生,是否中轉ICU和病死。消化道出血定義為胃腸引流液隱血陽性或連續兩次大便隱血陽性;SIRS和休克診斷參考外科學標準[2];急性腎損傷標準參考ADQI工作組的標準[3]。

二、 結果
1.臨床資料:共有85例患者入選。兩組患者基線值比較除APACHEⅡ評分外均無顯著性差異(表1)。

表1 增強CT組和對照組基線值比較
2.觀察指標:85例病例主要癥狀平均持續4 d,平均住院10 d。兩組間觀察指標的比較見表2。
3.Logisstic回歸分析:根據中位數,按主要癥狀持續時間≤4 d或>4 d,住院時間≤10 d或>10 d,將這兩個指標轉換為二分類變量。經單變量logistic回歸分析,增強CT檢查和住院時間與SIRS發生相關,與住院癥狀持續時間、消化道出血、休克、急性腎損傷、中轉ICU和病死無關。在多變量模型中,經病因和APACHEⅡ評分校正后,增強CT檢查和各種觀察指標均無相關性(表3)。
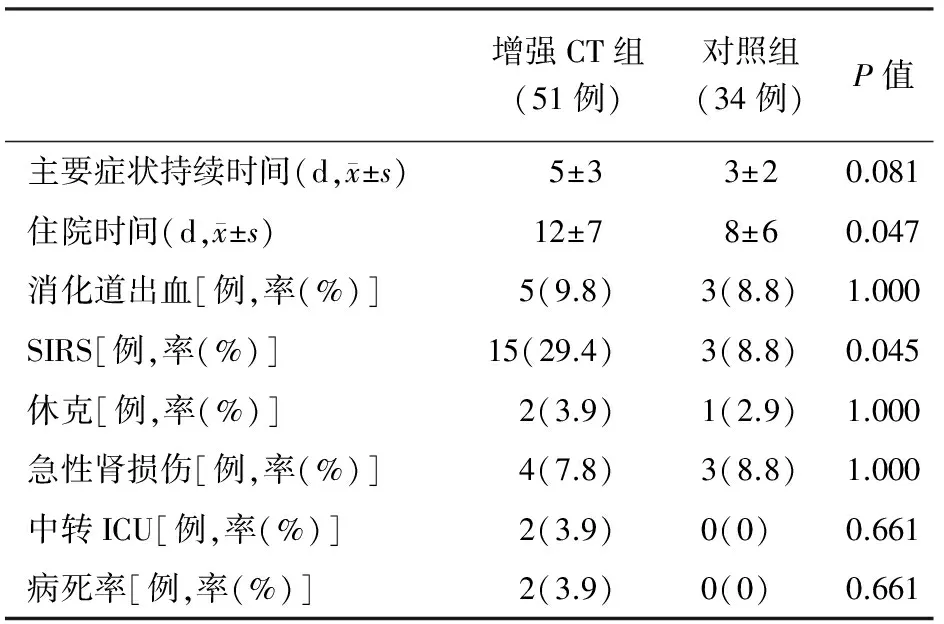
表2 增強CT組和對照組觀察指標比較
注:aP<0.05
討論增強CT,尤其是增強薄層多排CT,是判斷AP嚴重程度的最佳影像學檢查。增強CT使用的造影劑存在一定的毒副作用,滲透壓越高,毒性越大。造影劑包括離子型和非離子型。離子型為高滲性造影劑,如最早應用的泛影酸,現已較少使用。非離子型造影劑分為低滲和等滲造影劑。前者的滲透壓仍較血漿高2~4倍,包括目前常用的碘海醇(歐乃派克)、碘普胺(優維顯)和碘帕醇(典比樂);后者則幾乎與血漿相當,代表藥物是碘克沙醇(威視派克)。造影劑是否加重AP病情,目前還有爭議。
支持造影劑加重AP的證據主要來源于動物研究。給大鼠靜脈注射低滲造影劑會明顯減少微循環血流,對胰腺血流已經減少的區域影響更為明顯,從而進一步降低組織氧合,增加腺泡壞死及胰蛋白酶原激活肽生成[4]。給雨蛙素和甘氨脫氧膽酸誘導的AP大鼠注射離子型或非離子型造影劑,可增加大鼠死亡率[5-6]。由于胰腺為單支動脈供血,AP早期(通常為96 h)胰腺對缺血高度敏感。造影劑可能通過加重胰腺微循環障礙等途徑損傷胰腺,增加血液黏滯度,激活補體系統及對胰腺腺泡細胞的直接毒性作用;此外,造影劑的胰外損傷會加重內環境紊亂,潛在的造影劑腎病會增加病情嚴重程度。然而,在膽源性胰腺炎動物模型中,注射離子型造影劑并不加重病情[7]。在胰管內注射牛磺膽酸鈉制備急性壞死性胰腺炎模型中,離子型或非離子型造影劑并不降低胰腺局部血流量,也沒有加重胰腺組織的病理損害[8]。
有關增強CT是否加重AP患者病情的臨床資料目前十分有限。回顧性分析資料顯示[9-10],早期增強CT檢查可能延長AP病程,增加AP并發癥,延長患者住院時間。但較大規模的一項前瞻性、隨機對照研究入選了302例病例,其中264例在發病96 h內行增強CT,結果發現造影劑不會加重AP病情,反而可能降低早期病死率[11]。也有小樣本的前瞻性隨機對照研究得到了陰性結果[12]
本研究結果顯示,在單變量分析中除了住院時間和SIRS發生的比例較高外,增強CT組的各種觀察指標和對照組沒有顯著差別。進一步的多變量分析顯示,增強CT檢查不是AP各種觀察指標發生的獨立危險因素,提示增強CT不會影響AP病情。
[1] 王興鵬. 中國急性胰腺炎診治指南(草案). 中華內科雜志, 2004,43: 236-238.
[2] 吳在德, 吳肇漢. 外科學. 6版. 北京:人民衛生出版社, 2005,44-53.
[3] Bellomo R, Ronco C, Kellum JA, et al. Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care,2004,8:R204-R212.
[4] Schmidt J, Hotz HG, Foitzik T, et al. Intravenous contrast medium aggravates the impairment of pancreatic microcirculation in necrotizing pancreatitis in the rat.Ann Surg,1995,221:257-264.
[5] Foitzik T, Bassi DG, Schmidt J, et al. Intravenous contrast medium accentuates the severity of acute necrotizing pancreatitis in the rat. Gastroenterology,1994,106:207-214.
[6] Foitzik T, Bassi DG, Fernández-del Castillo C, et al. Intravenous contrast medium impairs oxygenation of the pancreas in acute necrotizing pancreatitis in the rat. Arch Surg, 1994,129:706-711.
[7] Kaiser AM, Grady T, Gerdes D, et al. Intravenous contrast medium does not increase the severity of acute necrotizing pancreatitis in the opossum.Dig Dis Sci,1995,40:1547-1553.
[8] Apodaca-Torrez FR, Goldenberg A, Lobo EJ, et al. Evaluation of the effects of noniodinized and iodinized ionic contrast media and gadoteric acid in acute necrotizing pancreatitis: experimental study in rabbits. Pancreas, 2007,35:e41-e44.
[9] McMenamin DA, Gates LK Jr. A retrospective analysis of the effect of contrast-enhanced CT on the outcome of acute pancreatitis. Am J Gastroenterol, 1996,91:1384-1387.
[10] Carmona-Sánchez R, Uscanga L, Bezaury-Rivas P, et al. Potential harmful effect of iodinated intravenous contrast medium on the clinical course of mild acute pancreatitis. Arch Surg, 2000,135:1280-1284.
[11] Uhl W, Roggo A, Kirschstein T, et al. Influence of contrast-enhanced computed tomography on course and outcome in patients with acute pancreatitis. Pancreas, 2002,24:191-197.
[12] Hwang TL, Chang KY,Ho YP. Contrast-enhanced dynamic computed tomography does not aggravate the clinical severity of patients with severe acute pancreatitis: reevaluation of the effect of intravenous contrast medium on the severity of acute pancreatitis. Arch Surg, 2000,135:287-290.
10.3760/cma.j.issn.1674-1935.2011.06.018
150655 廣州,中山大學附屬第六醫院消化內科(張敏、李初俊);中山大學附屬第一醫院消化內科(劉思純);中山大學附屬第一醫院黃埔院區消化內科(馬博、廖獻花)
劉思純,Email:liusichun66@sina.com
2011-02-23)
(本文編輯:呂芳萍)
