臨床局限性前列腺癌根治性切除與觀察等待預后比較的Meta分析
2014-04-24 09:25:31付生軍王志平
中國男科學雜志 2014年12期
羅 游 付生軍 王志平 楊 立
蘭州大學第二醫院泌尿外科,蘭州大學第二醫院泌尿外科研究所,
甘肅省泌尿系疾病臨床醫學中心,甘肅省泌尿系疾病重點實驗室(蘭州 730000)
臨床局限性前列腺癌根治性切除與觀察等待預后比較的Meta分析
羅 游 付生軍 王志平 楊 立*
蘭州大學第二醫院泌尿外科,蘭州大學第二醫院泌尿外科研究所,
甘肅省泌尿系疾病臨床醫學中心,甘肅省泌尿系疾病重點實驗室(蘭州 730000)
目的比較臨床局限性前列腺癌行根治性切除(radical prostatectomy, RP)和觀察等待(watchful waiting, WW)對患者生存的影響。方法通過計算機檢索Medline、Cochrane Library、ISI web of knowledge、SinoMed文獻檢索平臺,搜集國內外2014年7月前發表的關于早期前列腺癌根治性切除與主動監測的預后的隨機、半隨機對照試驗或觀察性研究,預后評價指標包括總體死亡、前列腺癌特異死亡;由2位研究者根據納入與排除標準獨立進行文獻篩選、資料提取和質量評價后,采用RevMan5.2進行統計分析。結果納入3個隨機對照試驗和10個臨床隊列研究,其中RCT共1 537例、隊列研究共186 590例患者;Meta分析結果顯示兩種治療方法(RP/WW)的總體死亡(ACM)風險為HR=0.59 [95%CI(0.51,0.69),P<0.00001],前列腺癌特異死亡(CSM)風險HR=0.43 [95%CI(0.32,0.58),P<0.00001],且不論RCT組還是隊列研究組,結果均一致傾向RP。結論 早期前列腺癌根治性切除可減少總體死亡及前列腺癌特異死亡風險,對于早期局限性前列腺癌選擇觀察等待應當十分慎重。
前列腺腫瘤/外科學; 存活率分析; 綜述; Meta分析
前列腺癌是男性泌尿系統常見的惡性腫瘤,其發病率逐年上升,2013年美國統計新發病例238 590例,位居男性腫瘤第一位,也是第二大腫瘤死亡原因[1]。隨著前列腺特異性抗原(PSA)檢測的普及,前列腺癌的發病率呈顯著增加趨勢,同時,也帶來了前列腺癌根治手術的增加,對于是否因此而造成早期前列腺癌的過度診斷與治療,以及PSA篩查的必要性均存在著爭議[2,3]。前列腺癌的治療手段主要以治愈性目的為主,包括根治性前列腺切除(radical prostatectomy, RP)、放療,伴或不伴雄激素去勢治療,治愈性治療方案常伴隨著發生率較高的陽痿、尿路功能障礙、生活質量的顯著降低以及高昂的治療費用等[4-9]。觀察等待(watchful waiting, WW)的定義是指在病程監測過程中,當患者癥狀或PSA水平出現進展時予以姑息性治療[10],其內容與觀察性治療基本一致或可認為是其另一種表達方式,觀察等待是保守治療策略的一種。前列腺癌“緩慢、惰性”的自然史表現可能并未使治愈性手段獲得更顯著療效優勢,也使得觀察等待成為可能[11,12]。雖然觀察等待在歐洲泌尿科學會(EAU)及美國國立綜合癌癥網絡(NCCN)均已被寫進前列腺癌診療指南[10,13],但對于根治性切除與觀察等待兩者的預后效果在不同文獻報道存在差異[14,15]。本文擬對早期局限性前列腺癌的不同干預效果進行系統評價及分析,為臨床早期前列腺癌的治療決策提供參考。
資料與方法
一、文獻納入與排除標準
(一)納入標準
(1)研究類型為隨機或非隨機對照研究;(2)經病理或細胞學確診為早期或局限性的前列腺癌患者(T1~2Nx~0Mx~0),不限年齡、種族;(3)文章內容包含有RP和WW兩者統計數據的臨床研究;(4)結局內容包括總體和(或)疾病特異死亡預后指標;(5)語種限定為中文及英文。
(二)排除標準
(1)標題摘要雖描述為臨床局限性前列腺癌但實際包含了大量T3及以上分期的高風險前列腺癌的研究;(2)最長隨訪時間低于5年的研究;(3)重復發表的文獻。
二、評價指標
評價兩種不同干預措施效果的結局指標有:總體死亡風險和前列腺癌特異死亡風險。
三、檢索策略
計算機檢索Medline、Cochrane Library、ISI we of knowledge、SinoMed平臺2014年7月前發表的關于早期RP與WW對比預后的相關文獻,同時查詢納入文獻的參考文獻。英文檢索式:radical prostatectom AND(observational therapy OR watchful waiting O expectant management OR deferred treatment OR delaye therapy OR conservative management)AND(earl prostate cancer OR localized prostate cancer OR low ris prostate cancer)AND(mortality OR survival),限定語種為英語。 中文檢索式:(早期前列腺癌 OR 局限性前列腺癌 OR 低危前列腺癌 OR 低風險前列腺癌)AND(根治 OR 手術)AND (觀察等待 OR 觀察等待 OR 延緩治療 OR 保守治療 OR 監測)。
四、文獻的篩選、數據提取和質量評價
由兩位研究者根據納入與排除標準獨立進行文獻篩選、資料提取與質量評價,并進行交叉核對,如遇分歧則通過討論或征求第三方的意見解決。數據的提取盡量以文獻原始數據為準,當資料不全或未詳細描述時采用以下兩種方法獲取數據:(1)郵件聯系作者獲得原始數據;(2)對于文獻未明確給出相關數據的可采用Tierney等[16]提出的數據提取方法和EXCEL表格計算HR和95%CI值;并參考AHR的一篇循證綜述提供的結果[17]。質量評價RCT采用Cochrane 系統評價員手冊5.1.0[18]中隨機試驗的偏倚風險評估工具,觀察性研究采用NOS(Newcastle Ottawa Scale)量表對納入研究的質量進行評價,5星以上考慮有較高質量。
五、統計分析
采用RevMan 5.2軟件進行meta分析。本文研究預后問題均使用計數資料,采用風險比(HR)作為效應量。以各效應量及其95% CI表示結果。首先采用x檢驗對納入研究結果進行異質性檢驗。若P≥0.1且I≤50%,提示各研究結果間無統計學異質性,采用固定效應模型進行Meta分析;若P<0.1但I2≤50%,提示各研究結果間存在異質性,但在可接受范圍內,采用隨機效應模型行Meta分析;若P<0.1或P≥0.1且I2>50%,認為各研究結果間異質性較大,對其異質性來源進行分析,并對可能導致異質性的因素進行亞組分析,若無明顯臨床異質性,采用隨機效應模型進行Meta分析。Meta分析的檢驗水準設為α=0.05,Meta分析結果采用森林圖呈現。
結 果
一、文獻檢索結果
通過相關檢索式初檢出715篇相關文獻,逐層篩選后最終納入3個隨機對照試驗(RCT)和10個隊列研究涉及共18篇文獻[14,15,19-34],包括188 127例患者,根治性前列腺切除105 213例,觀察等待82 914例。18篇均為英文文獻,無中文文獻。篩選流程及結果如圖1,納入文獻基本特征如表1。
二、納入研究的質量評價
如表1顯示RCT中美國退伍軍人管理局泌尿外科研究合作組(VACURG)[23,24]試驗偏倚風險較高,而前列腺癌干預與對比研究(PIVOT)[14]和斯堪地那維亞前列腺癌研究4組(SPCG-4)[15,19-22]的偏倚風險分別為中度、低度;隊列研究質量評價均在可接受范圍。

表1 納入研究的基本特征
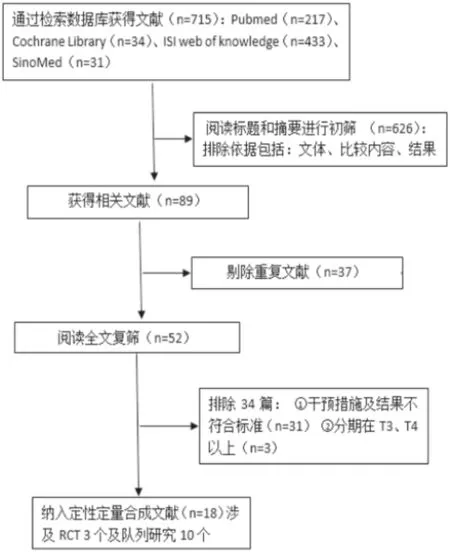
圖1 文獻篩選流程及結果
三、Meta分析結果
(一)總體死亡
3個RCT和8個隊列研究的合并效應及11個研究的總體效應均顯示RP對比WW顯著減少總體死亡(ACM)風險HR=0.59 [95%CI(0.51,0.69),<0.00001],見圖2。
(二)腫瘤特異死亡
2個RCT和7個隊列研究的合成效應以及9個研究的總體效應均顯示RP組前列腺癌特異死亡(CSM)要顯著低于WW組 HR=0.43 [95%C(0.32,0.58),P<0.00001],見圖3。
(三)敏感性分析
在Meta分析時發現,Iversen 1995[24]因年代太久、隨訪質量低而被敏感性剔除后,所有結果仍然顯示不論RCT組還是非隨機對照試驗(NRCT)組、ACM還是CSM均顯著支持RP(結果未展示)。
(四)發表偏倚
圖4和圖5顯示合并效應中線兩側研究數量接近,無明顯發表偏倚見。;在敏感性分析時的同樣未見顯著發表偏倚(漏斗圖未給出)。
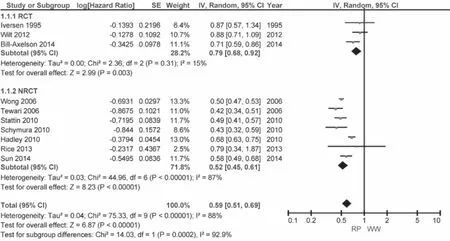
圖2 總體死亡--研究類型分組
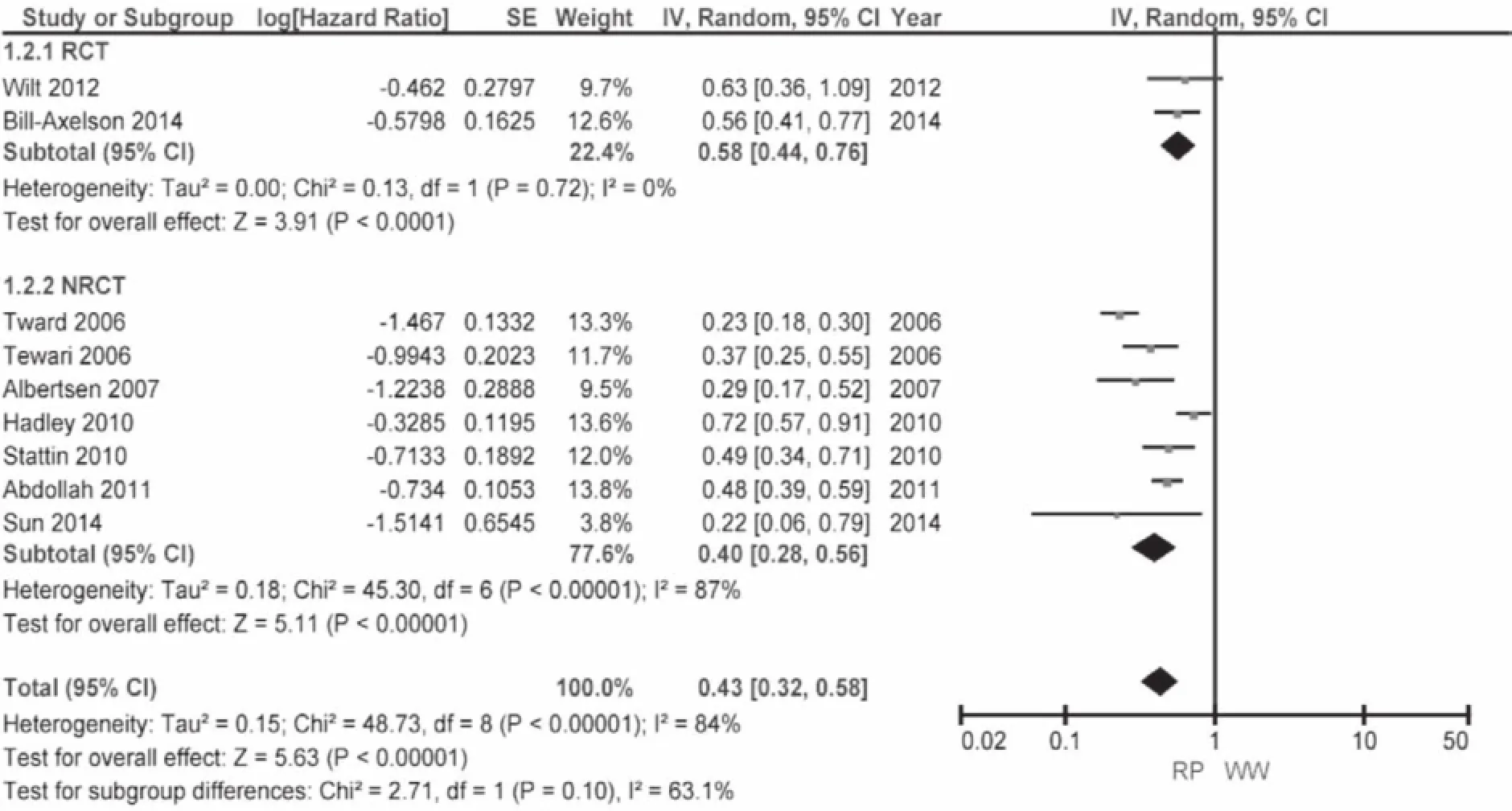
圖3 前列腺癌特異死亡--研究類型分組
討 論
對于早期局限性前列腺癌的保守治療策略分為兩類即“觀察等待”和“主動監測”,兩者的最大區別在于對疾病進展的處理策略,主動監測傾向于治愈性治療方案如根治、放療,而觀察等待在疾病進展時往往予以姑息性處理如TURP、姑息性去勢治療;其次在隨訪中主動監測可能更多涉及穿刺活檢。NCCN指南2014最新版指出主動監測(AS)適用于極低、低風險并且生存期望≥10年的早期前列腺癌患者,推薦監測頻率PSA不低于6個月,直腸指檢及穿刺活檢不低于12個月,除非在有臨床提示的情況下;而觀察等待無特定的適應指證,一般在T1-2期且壽命期望<10年的可以考慮,也適用于各種治療反應不佳的患者[10]。
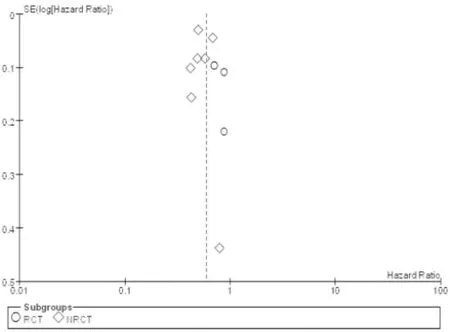
圖4 總體死亡漏斗圖
勃起功能障礙(ED)和尿路功能障礙是根治性手術的兩大并發癥,對于相對年輕人群及性生活需求顯著的患者尤為重要。Bill-Axelson等[19]的研究報道手術后1年ED率58.1%,尿瘺率32.2%;對于ED目前提倡神經保留手術,保留神經有利于術后性功能的恢復[35],但保留神經手術帶了來手術切緣腫瘤陽性率增加的風險[36],術后應用磷酸二酯酶-5型抑制劑有助于改善勃起功能及其恢復[37-39]。生活質量也是治療方案選擇的重要影響因素,研究表明手術后的生活質量RP對比WW明顯變差[5,40,41],表現在性行為的不滿意帶來的心理障礙、社交活動的心理負擔、焦慮、抑郁等方面。醫療費用也是值得考慮的另一個決定因素,保守治療對比根治手術能夠相對減少治療費用[8]。
從本研究結果看來無論是總體死亡還是前列腺癌特異死亡,根治手術均優于觀察等待。但其中兩個十分重要的RCT結果卻不盡相同,PIVOT實驗結果顯示不論ACM還是CSM,RP與WW的預后無顯著差異,而SPCG-4在ACM和CSM上均顯著支持RP。對于這兩個研究結果的差異,有學者認為該差異是因為PIVOT是PSA時代的產物而SPCG-4研究在前PSA時代,從而PIVOT研究包含了更多的經PSA篩選的T1c期患者。另一方面,PSA帶來的另一個影響是作為前列腺癌進展的監測指標,或許能有益于患者的管理而提高生存,但這兩個研究的跟蹤隨訪中均有PSA監測指標。Vuong等[42]對這兩個研究比較分析后認為期望壽命以及隨訪時間的不同是PIVOT難以證實RP受益的重要原因。而Xia等[43]的假設分析認為PSA篩選時代的前置期和過度診斷是PIVOT顯示很低絕對受益的原因,因而不能作為RP無效的有力證據。作者對這兩個研究的隨機化服從情況比較分析可以看出PIVOT研究中不服從隨機到WW組(75/367)遠高于SPCG-中的不服從率(30/348),P<0.0001;同樣不服從隨機到RP組比例PIVOT(83/364)比SPCG-4(54/347)卻無顯著差異,P=0.098。這可能是PIVOT無法顯示出RP受益的重要原因。
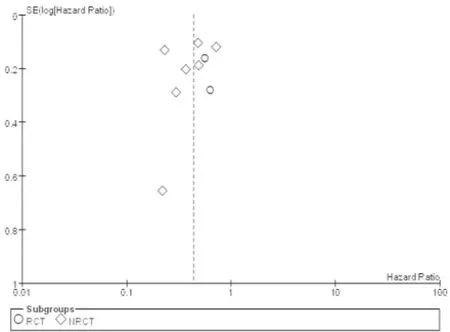
圖5 前列腺癌特異死亡漏斗圖
本研究的局限性表現在納入研究中僅3個RCT,且質量參差不齊,其余均為回顧性隊列研究,同時納入的隊列研究中部分存在觀察地區的交叉,這些可能造成不同程度的風險偏倚;另一方面,研究結果僅限于總體人群,因不同研究以不同分層方式報道亞組結果而無法進行亞組合成分析(比如不同腫瘤風險、Gleason評分、PSA水平等),亞組分析可能能夠更加細致的探討觀察等待的適應人群。
本Meta分析結果提示:RP對總體和前列腺癌特異死亡均有顯著優勢,早期前列腺癌根治性切除可減少總體死亡及前列腺癌特異死亡風險,對于早期局限性前列腺癌選擇觀察等待應當十分慎重,治療方案的選擇需要結合患者其他因素綜合考慮。
1 Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA:A Cancer Journal for Clinicians2013; 63(1): 11-30.
2 Xia J, Gulati R, Au M,et al. Effects of Screening on Radical Prostatectomy Eff cacy: The Prostate Cancer Intervention Versus Observation Trial.J Natl Cancer Inst2013; 105(8): 546-550
3 Loeb S, Bjurlin MA, Nicholson J,et al.Overdiagnosis and Overtreatment of Prostate Cancer.Eur Urol2014 65(6): 1046-1055
4 Bill-Axelson A, Garmo H, Holmberg L,et al. Long-termDistress After Radical Prostatectomy Versus Watchful Waiting in Prostate Cancer: A Longitudinal Study from the Scandinavian Prostate Cancer Group-4 Randomized Clinical Trial.Eur Urol2013; 64(6): 920-928
5 Johansson E, Steineck G, Holmberg L, et al. Long-term quality-of-life outcomes after radical prostatectomy or watchful waiting: the Scandinavian Prostate Cancer Group-4 randomised trial.Lancet Oncol2011; 12(9): 891-899
6 Steineck G, Helgesen F, Adolfsson J,et al. Quality of life after radical prostatectomy or watchful waiting.N Engl J Med2002; 347(11): 790-796
7 Perlroth DJ, Bhattacharya J, Goldman DP,et al. An Economic Analysis of Conservative Management Versus Active Treatment for Men with Localized Prostate Cancer.J Natl Cancer Inst Monogr2012; 2012(45): 250-257
8 Corcoran AT, Peele PB, Benoit RM. Cost Comparison Between Watchful Waiting With Active Surveillance and Active Treatment of Clinically Localized Prostate Cancer.Urology2010; 76(3): 703-707
9 Konety BR, Cowan JE, Carroll PR. Patterns of primary and secondary therapy for prostate cancer in elderly men: analysis of data from CaPSURE.J Urol2008; 179(5): 1797-1803
10 NCCN. NCCN Clinical Practice Guidelines in Oncology (Version I.2014): Prostate Cancer[EB/OL]. [2014-06-28]. http://www.nccn.org/professionals/physician_gls/pdf/ prostate.pdf.
11 Popiolek M, Rider JR, Andren O,et al. Natural History of Early, Localized Prostate Cancer: A Final Report from Three Decades of Follow-up.Eur Urol2013; 63(3): 428-435
12 Elliott SP, Meng MV, Elkin EP,et al. Incidence of urethral stricture after primary treatment for prostate cancer: data From CaPSURE.J Urol2007; 178(2): 529-534
13 Mottet N, Bastian PJ, Bellmunt J,et al. Guidelines on Prostate Cancer [EAU 2014][EB/OL]. [2014-06-28]. http://www.uroweb.org/guidelines/online-guidelines/ ?no_cache=1.
14 Wilt TJ, Brawer MK, Jones KM,et al.Radical Prostatectomy versus Observation for Localized Prostate Cancer.N Engl J Med2012; 367(3): 203-213
15 Bill-Axelson A, Holmberg L, Garmo H,et al. Radical prostatectomy or watchful waiting in early prostate cancer.N Engl J Med2014; 370(10): 932-942
16 Tierney JF, Stewart LA, Ghersi D,et al.Practical method for incorporating summary time-to-event data into metaanalysis.Trials2007; 8(1): 16
17 Ip S, Dahabreh IJ, Chung M,et al.An evidence review o active surveillance in men with localized prostate cancer.Evid Rep Technol Assess (Full Rep)2011; (204): 1-341
18 Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011][EB/OL]. http://www.handbook.cochrane.org/.
19 Bill-Axelson A, Holmberg L, Ruutu M,et al. Radical prostatectomy versus watchful waiting in early prostat cancer.N Engl J Med2011; 364(18): 1708-1717
20 Bill-Axelson A, Holmberg L, Ruutu M,et al. Radical prostatectomy versus watchful waiting in early prostate cancer.N Engl J Med2005; 352(19): 1977-1984
21 Holmberg L, Bill-Axelson A, Helgesen F,et al. A randomized trial comparing radical prostatectomy with watchfu waiting in early prostate cancer.N Engl J Med2002 347(11): 781-789
22 Bill-Axelson A, Holmberg L, Filen F,et al. Radical Prostatectomy Versus Watchful Waiting in Localized Prostate Cancer: the Scandinavian Prostate Cancer Group-4 Randomized Trial.J Natl Cancer Inst2008; 100(16): 1144-1154
23 Graversen PH, Nielsen KT, Gasser TC,et al. Radical prostatectomy versus expectant primary treatment in stages I and II prostatic cancer. A f fteen-year followup.Urology1990; 36(6): 493-498
24 Iversen P, Madsen PO, Corle DK. Radical prostatectomy versus expectant treatment for early carcinoma of the prostate. Twenty-three year follow-up of a prospectiv randomized study.Scand J Urol Nephrol Suppl1995; 172: 65-72
25 Stattin P, Holmberg E, Johansson J E,et al. Outcomes in Localized Prostate Cancer: National Prostate Cancer Register of Sweden Follow-up Study.J Natl Cancer Inst2010; 102(13): 950-958
26 Abdollah F, Sun M, Schmitges J,et al. Cancer-Specif c and Other-Cause Mortality After Radical Prostatectomy Versus Observation in Patients with Prostate Cancer: Competing-Risks Analysis of a Large North American Population-Based Cohort.Eur Urol2011; 60(5): 920-930
27 Hadley J, Yabroff KR, Barrett MJ,et al. ComparativeEffectiveness of Prostate Cancer Treatments: Evaluating Statistical Adjustments for Confounding in Observational Data.J Natl Cancer Inst2010; 102(23): 1780-1793
28 Tewari A, Raman JD, Chang P,et al. Long-term survival probability in men with clinically localized prostate cancer treated either conservatively or with definitive treatment (radiotherapy or radical prostatectomy).Urology2006; 68(6): 1268-1274
29 Sun M, Sammon JD, Becker A,et al.Radical prostatectomy vs radiotherapy vs observation among older patients with clinically localized prostate cancer: a comparative effectiveness evaluation.BJU Int2014; 113(2): 200-208
30 Schymura MJ, Kahn AR, German RR,et al. Factors associated with initial treatment and survival for clinically localized prostate cancer: results from the CDC-NPCR Patterns of Care Study (PoC1).BMC Cancer2010; 10: 152
31 Rice KR, Colombo ML, Wingate J,et al. Low risk prostate cancer in men >/= 70 years old: to treat or not to treat.Urol Oncol2013; 31(6): 755-760
32 Wong Y, Mitra N, Hudes G,et al.Survival Associated With Treatment vs Observation of Localized Prostate Cancer in Elderly Men.JAMA2006; 296(22): 2683-2693
33 Albertsen PC, Hanley JA, Penson DF,et al. 13-Year Outcomes Following Treatment for Clinically Localized Prostate Cancer in a Population Based Cohort.J Urol2007; 177(3): 932-936
34 Tward JD, Lee CM, Pappas LM,et al. Survival of men with clinically localized prostate cancer treated with prostatectomy, brachytherapy, or no definitive treatment-Impact of age at diagnosis.CANCER2006; 107(10): 2392-2400
35 Suardi N, Moschini M, Gallina A,et al.Nerve-sparing approach during radical prostatectomy is strongly associated with the rate of postoperative urinary continence recovery.BJU Int2013; 111(5): 717-722
36 Roder MA, Thomsen FB, Christensen IJ,et al. Risk factors associated with positive surgical margins following radical prostatectomy for clinically localized prostate cancer: can nerve-sparing surgery increase the risk?.Scand J Urol2014; 48(1): 15-20
37 Gandaglia G, Gallina A, Suardi N,et al. Preoperative erectile function is the only predictor of the use of a high number of phosphodiesterase type-5 inhibitors afte bilateral nerve-sparing radical prostatectomy.Int J Impot Res2014; 26(6): 201-204
38 Montorsi F, Brock G, Stolzenburg JU,et al.Effects of Tadalafil Treatment on Erectile Function Recovery Following Bilateral Nerve-sparing Radical Prostatectomy: A Randomised Placebo-controlled Study (REACTT).Eur Urol2014; 65(3): 587-596
39 Wang X, Wang X, Liu T,et al.Systematic review and meta-analysis of the use of phosphodiesterase type 5 inhibitors for treatment of erectile dysfunction following bilateral nerve-sparing radical prostatectomy.PLoS One2014; 9(3): e91327
40 Couper J W, Love A W, Dunai J V,et al. The psychologica aftermath of prostate cancer treatment choices: a comparison of depression, anxiety and quality of life outcomes over the 12 months following diagnosis.Med J Aust2009; 190(7 Suppl): S86-S89
41 Litwin MS, Lubeck DP, Spitalny GM,et al. Mental health in men treated for early stage prostate carcinoma.Cancer2002; 95(1): 54-60
42 Vuong W, Sartor O, Pal S. Management of localized prostate cancer: the pendulum swings (back to the middle).Asian J Androl2014; 16(4): 570-571
43 Xia J, Gulati R, Au M,et al.Effects of Screening on Radica Prostatectomy Eff cacy: The Prostate Cancer Intervention Versus Observation Trial.J Natl Cancer Inst2013; 105(8): 546-550
(2014-08-30收稿)
Radical prostatectomy versus watchful waiting for clinically localized prostate cancer: A Meta-Analysis
Luo You, Fu Shengjun, Wang Zhiping, Yang Li*Department of Urology, Lanzhou University Second Hospital; Institute of Urology, Lanzhou University Second Hospital; Institute of Gansu Nephro-Urological Clinical Center; Key laboratory of urological disease of Gansu province, Lanzhou
730000, China
Yang Li, E-mail: yuze250@163.com
ObjectiveTo compare the survival effect of clinically localized prostate cancer treated by radical prostatectomy (RP) and watchful waiting (WW) .MethodsRandomized controlled trials or observational studies were searched from database of Medline, Cochrane Library, ISI web of knowledge and SinoMed for the evaluation of prognosis of clinically localized prostate cancer treated by RP versus WW. Prognosis evaluation parameter included all-cause mortality and prostate cancer specif c mortality. The latest retrieval date was July 2014. The data extraction and the quality assessment of included studies were independently conducted by 2 reviewers. RevMan5.2 software was used to perform data synthesis.Results3 RCTs involving 1 537 patients (772 RP versus 765 WW) and 10 retrospective cohort studies involving 186 590 patients (104441 RP versus 82149 WW) were enrolled f nally. The results of meta-analysis showed that both the hazard of allcause mortality and prostate cancer specif c mortality in RP group were signif cantly lower than that of WW group, all-cause mortality risk was HR=0.59 [95%CI (0.51, 0.69),P<0.00001], and prostate cancer specif c mortality risk was HR=0.43 [95%CI (0.32, 0.58),P<0.00001]. All outcomes favored radical prostatectomy regardless of study type stratification.ConclusionRadical prostatectomy reduces the hazard of all-cause mortality and cancer specif c mortality of clinically localized prostate cancer, which may push more deliberations when physicians take watchful waiting in consideration.
prostatic neoplasms/surgery; survival analysis; review, systematic; Meta-analysis
10.3969/j.issn.1008-0848.2014.12.005
R 737.25
*通訊作者, E-mail: yuze250@163.com
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
民用飛機設計與研究(2020年4期)2021-01-21 09:15:02
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:02
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
家庭醫學(下半月)(2020年3期)2020-05-30 12:42:00
科技傳播(2019年22期)2020-01-14 03:06:54
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
中國生殖健康(2019年7期)2019-01-06 09:27:34
電子制作(2018年18期)2018-11-14 01:48:24