小腦型多系統萎縮患者的血尿酸水平
2014-06-01 09:09:35董靖德張麗靳凌
實用老年醫學 2014年7期
董靖德 張麗 靳凌
小腦型多系統萎縮患者的血尿酸水平
董靖德 張麗 靳凌
目的通過觀察小腦型多系統萎縮患者(MSA?C)的血尿酸水平,探討MSA?C患者血尿酸水平與病程的關系。方法2011年6月至2013年4月間在我院神經科病房收治的MSA?C患者21例作為觀察組,選取相同時期健康體檢的人群22例作為對照組,早晨空腹抽取肘正中靜脈血4 ml,測定血尿酸水平,分析血尿酸水平與其病程的相關性。結果MSA?C患者血尿酸水平[(279.19±71.48)mmol/L]明顯低于正常人群的血尿酸水平[(340.96±58.02)mmol/L](P<0.05);MSA?C患者的血尿酸水平與病程無明顯相關性(r=0.041,P=0.859)。結論MSA?C患者可能受氧化應激反應的影響,血尿酸水平明顯下降,但血尿酸水平高低與病程無關。
小腦型多系統萎縮;尿酸;病程
尿酸是嘌呤代謝的終產物,具有抗氧化應激的作用。近年來尿酸對神經變性疾病的保護作用越來越受到人們的關注。在神經變性疾病帕金森病(Parkinson's disease,PD)動物模型中發現尿酸可抑制氧化應激,阻止多巴胺神經元的死亡[1]。而尿酸在多系統萎縮患者中的作用報道不多,本研究通過觀察小腦型多系統萎縮(MSA?C)患者的血尿酸水平,探討MSA?C患者血尿酸水平與病程的關系。
1 對象與方法
1.1 研究對象 收集2011年6月至2013年4月間在我院神經科門診和病房收治的MSA?C患者共21例,為MSA?C組,男12例,女9例,年齡50~70歲,平均(58.1±7.9)歲。均為散發病例。另外選取23例相同時期健康體檢的人群作為對照組,男12例,女11例,年齡50~70歲,平均(59.8±6.3)歲。2組性別、年齡差異無統計學意義(P>0.05)。MSA?C患者經詳細的病史詢問和神經系統查體,排除酒精中毒、服苯妥英鈉及高血壓病史。根據1999年美國密歇根大學Gilman等[2]提出的MSA的4組臨床特征和診斷標準。臨床特征:(1)自主神經功能衰竭和(或)排尿功能障礙;(2)PD綜合征;(3)小腦性共濟失調;(4)皮質脊髓功能障礙。診斷標準:(1)可能MSA:第1個臨床特征加上2個其他特征;(2)很可能MSA:第1個臨床特征加一個對多巴胺反應不佳的帕金森綜合征或小腦性共濟失調;(3)確定診斷MSA:神經病理檢查證實。本研究對象MSA?C患者均有小腦性共濟失調癥狀。所有研究對象均為本地區居民,飲食結構及生活習慣相似。
1.2 血液標本收集及測定 所有受試對象均采用早晨空腹抽取肘正中靜脈血4 ml,應用美國DADE?Behring公司全自動生化分析儀測定血尿酸、肝腎功能及血脂水平。
1.3 統計學處理 采用SPSS 17.0統計學軟件,對2組一般資料分別進行正態性檢驗,方差齊性檢驗,然后進行t檢驗比較2組均數。相關關系應用Spearman等級相關分析尿酸與病程的相關性。P<0.05為有統計學意義。
2 結果
2.1 一般資料的比較 MSA?C患者的肝功能(丙氨酸氨基轉移酶)、腎功能(肌酐)以及血脂(三酰甘油、總膽固醇)水平與正常人群比較差異無統計學意義(P>0.05)。見表1。
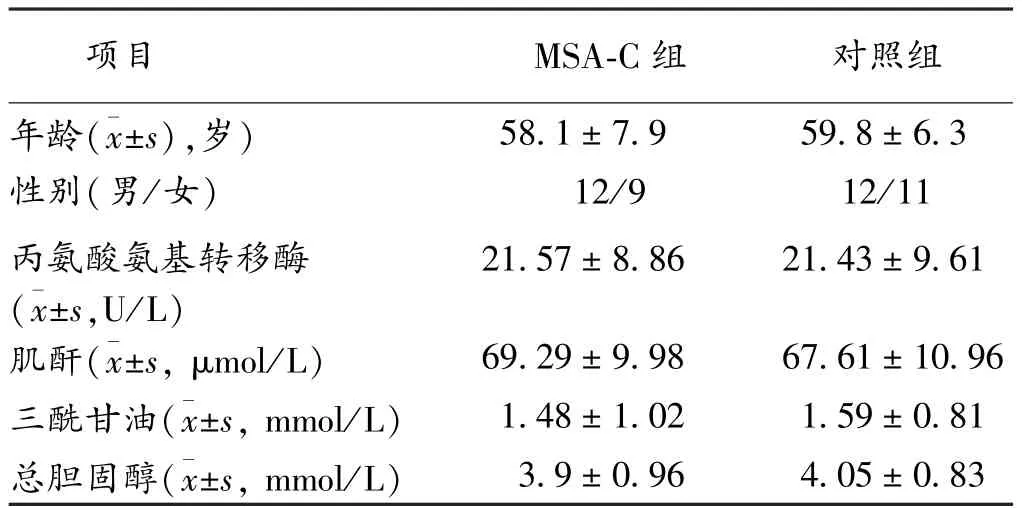
表1 MSA?C患者與正常人群一般資料比較
2.2 MSA組與正常人群的血尿酸水平比較 MSA?C患者平均血尿酸為(279.19±71.48)mmol/L,明顯低于對照組的血尿酸水平[(340.96±58.02)mmol/L],P<0.05。
2.3 MSA患者血尿酸水平與其病程的相關性分析MSA患者平均病程為(2.76±2.69)年,MSA?C患者的血尿酸水平與病程無明顯相關性(P>0.05)。
3 討論
MSA是一組原因不明、散發、進行性進展的神經系統變性疾病,可累及錐體外系、自主神經和小腦3大系統。MSA多發生在>50歲的中老年人[3],主要臨床表現是緩慢進展的多組神經系統癥狀,如步態蹣跚、吟詩樣語言等小腦功能障礙,肌張力增高、強直、運動遲緩等帕金森樣癥狀以及體位性低血壓、暈厥、陽痿等自主神經癥狀。
目前MSA的發病機制不明,氧化應激反應可能為MSA潛在的發病原因。氧化應激反應是指體內生成的氧自由基等超過體內內源性抗氧化應激能力的代償,引起生物膜上的不飽和脂肪酸形成過氧化脂質,對蛋白質、DNA、RNA及多糖高分子物質等產生氧化、交聯、變性和降解,導致膜流動性降低、通透性增高、線粒體腫脹、溶酶體釋放生物酶、細胞器及酶的結構和功能破壞,從而引起的組織氧化損傷過程。過量自由基導致的氧化應激反應在神經變性疾病的發生和發展過程中起著重要的作用。Ying等[4]發現在MSA患者中由于氧化應激反應導致內環境Ca2+紊亂,最終可引起膠質細胞的死亡。Riedel等[5]發現給予氧化應激刺激后,共核蛋白(α?Syn)疾病(MSA、PD等)的膜脂質修飾發生改變,從而導致α?Syn疾病包涵體形成。
尿酸是體內腺苷、鳥苷和飲食中細胞內核糖核酸嘌呤代謝的終末產物[6],是人體內特有的天然水溶性抗氧化劑,具有清除氧自由基和其他活性自由基的作用,比抗壞血酸有更顯著的增強紅細胞膜脂質抗氧化、防止細胞溶解凋亡的作用。尿酸可增強超氧化物歧化酶(SOD)活性,延長其生存,防止細胞過氧化。在尿酸與神經變性疾病關系的研究中,Shen等[7]對PD的發病危險因素與尿酸關系的Meta分析表明:尿酸與PD的危險因素之間有密切的相關性,特別是在男性患者中。并且發現PD患者維持高尿酸水平有助于延緩病情的發展。Sun等[8]對中國PD患者與尿酸關系的研究表明低尿酸血癥是PD發病的獨立危險因素。Auinger等[9]對亨廷頓病患者的血清尿酸水平的研究中發現,隨著亨廷頓病病情加重,尿酸水平也逐漸下降,且高尿酸水平在亨廷頓病中發揮的作用與在PD中一樣,可延緩疾病的發展。目前國內尿酸與MSA之間關系的研究少見,而我們的研究結果表明MSA?C患者的血尿酸明顯低于正常人群,說明MSA?C患者清除氧自由基能力明顯低于正常人群,而體內的自由基增多可能導致MSA病情的加重。但本研究對尿酸與MSA?C病程的分析顯示二者無相關性,可能與本次入組的樣本量過小有關。因此研究具有一定的局限性,而今后的研究需要我們進一步觀察尿酸水平與MSA發生發展、病情嚴重程度的關系。
[1] Perry G,Moreira PI,Siedlak SL,etal.Natural oxidantbal?ance in Parkinson disease[J].Arch Neurol,2009,66(12):1445.
[2] Gilman S,Low PA,Quinn N,etal.Consensus statementon the diagnosis ofmultiple system atrophy[J].JNeurol Sci,1999,163(1):94?98.
[3] 王博,張朝東,李昭.多系統萎縮的臨床特征與疾病進展的特點[J].臨床神經病學雜志,2007,20(6):407?410.
[4] Ying Z,Lin F,Gu W,et al.α?synuclein increases U251 cells vulnerability to hydrogen peroxide by disrupting calcium homeostasis[J].J Neural Transm,2011,118(8):1165?1172.
[5] Riedel M,Goldbaum O,Wille M,et al.Membrane lipid modification by docosahexaenoic acid(DHA)promotes the formation ofα?synuclein inclusion bodies immunopositive for SUMO?1 in oligodendroglial cells after oxidative stress[J].J Mol Neurosci,2011,43(3):290?302.
[6] 劉昌慧,白玉鵬.老年人高尿酸血癥與冠心病的相關性研究[J].實用老年醫學,2006,20(2):95?97.
[7] Shen C,Guo Y,LuoW,et al.Serum urate and the risk of Parkinson's disease:results from ameta?analysis[J].Can J Neurol Sci,2013,40(1):73?79.
[8] Sun CC,Luo FF,Wei L,et al.Association of serum uric acid levels with the progression of Parkinson's disease in Chinese patients[J].Chin Med J(Engl),2012,125(4):583?587.
[9] Auinger P,Kieburtz K,McDermott MP.The relationship between uric acid levels and Huntington's disease progression[J].Mov Disord,2010,25(2):224?228.
Blood uric acid levels in the patients w ith m ultip le system atrophy?cerebellar type
DONG Jing?de,ZHANG Li,JIN Ling.Department ofGeriatric Neurology,the Brain Hospital Affiliated to Nanjing Medical University,Nanjing 210029,China
ObjectiveTo explore the blood uric acid level in the patientswithmultiple system atrophy?cerebellar type(MSA?C)and to discover the relationship between blood uric acid level and the course of MSA.MethodsTwenty?one pa?tientswith MSA?C in the neurologicalward of our hospital from June 2011 to April 2013 were enrolled as observation group. Twenty?two healthy people were enrolled as control group in the same period.The fasting bloodswere collected from the elbow venous in themorning and the blood uric acid levelwas detected.The relationship of blood uric acid level with the course of MSA?C was analyzed.ResultsThe blood uric acid level(279.19±71.48mmol/L)of the patientswith MSA?Cwas signifi?cantly lower than that of health people(340.96±58.02mmol/L)(P<0.05).The blood uric acid level was not significantly related with the course of MSA?C(r=0.041,P=0.859).ConclusionsMSA?Cmay be influenced by oxidative stress and induce the decrease of blood uric acid level,but the blood uric acid level has no relationswith the course of MSA?C.
multiple system atrophy?cerebellar type;uric acid;course of disease
R 446.1
A
10.3969/j.issn.1003?9198.2014.07.013
2013?10?31)
210029江蘇省南京市,南京醫科大學附屬腦科醫院老年神經科
靳凌,Email:jinling19750712@163.com
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
美與時代·美術學刊(2022年3期)2022-04-27 01:18:15
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
世界科學技術-中醫藥現代化(2020年2期)2020-07-25 02:05:56
科技傳播(2019年22期)2020-01-14 03:06:54
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
人大建設(2019年12期)2019-05-21 02:55:32
西南軍醫(2016年6期)2016-01-23 02:21:19
西南軍醫(2015年2期)2015-01-22 09:09:37
食品科學(2013年15期)2013-03-11 18:25:48