CT肺動脈造影與MR診斷肺動脈栓塞臨床價值的 Meta分析
2014-08-10 12:28:29周璐范占明張兆琪徐磊于薇晏子旭姜紅
疑難病雜志 2014年4期
周璐,范占明,張兆琪,徐磊,于薇,晏子旭,姜紅
薈萃分析
CT肺動脈造影與MR診斷肺動脈栓塞臨床價值的 Meta分析
周璐,范占明,張兆琪,徐磊,于薇,晏子旭,姜紅
目的對CT肺動脈造影與MR評估肺動脈栓塞(PE)的臨床應用價值進行Meta分析。方法網絡檢索中英文數據庫MEDLINE、EMBASE、Cochrane圖書館、CBM、CNKI和萬方數據等,搜集公開發表的關于CT肺動脈造影與肺動脈MR評估PE的文獻,應用STATA12.0統計軟件進行數據合并,計算診斷試驗的敏感性、特異性和ROC曲線下面積(AUC)。結果共16項研究1 497例受試對象納入Meta分析,其中應用CT肺動脈造影評價PE 11項研究,MR檢查5項研究。Meta分析結果顯示CT肺動脈造影和MR評價PE的敏感性分別為0.79(95%CI 0.75~0.83)和0.54(95%CI 0.48~0.60),特異性分別為0.90(95%CI 0.87~0.93)和0.98(95%CI 0.96~1.00);CT肺動脈造影和MR評價PE的AUC分別為0.94(95%CI 0.92~0.96)和0.99(95%CI 0.97~0.99)。結論CT肺動脈造影與MR評估PE的準確性較高,可作為臨床評估PE的有效方法。
肺動脈栓塞;CT;核磁共振成像;Meta分析
肺動脈栓塞(pulmonary embolism,PE)臨床上較為常見[1],為內源性或外源性栓子堵塞肺動脈或其分支引起肺循環障礙的臨床和病理生理綜合征。其中最主要、最常見的類型為肺動脈血栓栓塞(pulmonary thromboembolism,PTE),還包括其他以肺血栓性栓子栓塞為病因的類型,如脂肪栓塞、羊水栓塞、空氣栓塞、異物栓塞和腫瘤栓塞。肺動脈栓塞后發生肺出血或壞死者稱肺梗死(pulmonary infarction)。肺動脈栓塞主要表現為三聯征,包括胸痛、呼吸困難和咯血,但大多數情況下并非所有患者都表現出上述癥狀,通過臨床癥狀診斷PE往往敏感性和特異性較低,易造誤診或漏診。近年來隨著影像學技術的發展,CT動脈造影和MR被逐漸用于PE的診斷,影像學技術在PE診斷方面顯現出了巨大的優勢,但由于各研究樣本量較小,統計效能較低,其對PE的診斷價值一直存在爭議。因此,本研究采用循證醫學的方法,對既往關于CT和MR作為檢測手段評估PE的臨床診斷試驗進行匯總并對相關數據進行Meta分析,探討CT肺動脈造影與MR用于評價PE的臨床價值。
1 資料與方法
1.1 文獻入選與排除 文獻發表語言:英語和漢語;研究類型:前瞻性對照研究;研究對象:臨床上可疑PE患者;診斷金標準:肺動脈造影。
1.2 文獻檢索 采用關鍵詞與自由詞結合的方式進行檢索相關數據庫,EDLINE、EMBASE、Cochrane等英文數據庫檢索詞為 “pulmonary embolism/PE”“Computer tomography” “Magnetic resonance image” 。CBM、CNKI和萬方數據等中文數據庫檢索詞為以“肺動脈栓塞” “計算機輔助成像”“磁共振成像”。同時為避免文獻丟失,我們還對納入文獻的參考文獻進行了手工檢索,以發現可能合格的相關研究報道。
1.3 數據提取 根據文獻納入與排除標準進行相關數據庫文獻檢索和文獻篩查,納入符合要求的文獻并剔除不符合要求的文獻,對于符合要求的文獻進行相關數據提取。提取的內容有:作者姓名、文章發表時間、研究實施所在地區、待評價診斷試驗、入組患者人數及待評價試驗的敏感性、特異性、真陽性、假陽性、假陰性、真陰性。文獻納入采用雙人平行評價的方法,對于存在爭議的數據則請教相關專家或與第三人討論,最終決定是否納入。
1.4 統計學方法 采用STATA12.0軟件進行統計分析,將提取的數據輸入數據庫(EXCEL),統計學異質性采用Q統計量的I2檢驗,I2<50%認為各研究間不存在異質性,采用固定效應模式(fixed effect model)進行合并;如果I2>50%則認為各研究間存在異質,采用隨機效應模型(randomized effect model)進行合并。分別合并診斷實驗的敏感性、特異性、陽性似然比、陰性似然比,STATA 11.0統計軟件繪制合并后的受試者工作特征(ROC)曲線,計算曲線下面積(AUC)。P<0.05為差異有統計學意義。
2 結 果
2.1 文獻檢索 依據納入與排除標準,檢索相關數據庫,初檢索到關于CT肺動脈造影與MR評估PE的臨床研究文獻共521篇。進一步通過瀏覽文獻的題目和摘要,排除明顯不符合要求的研究505項,結果納入文獻16篇,納入分析的文獻具體特征見表1。
2.2 異質性檢驗 提取16篇原始文獻中的診斷真陽性、假陽性、真陰性和假陰性,并根據其具體數值計算診斷試驗敏感性和特異性的統計學異質性。異質性檢驗結果顯示,診斷的敏感性和特異性均存在統計學異質性,故采用隨機效應模型進行數據合并。
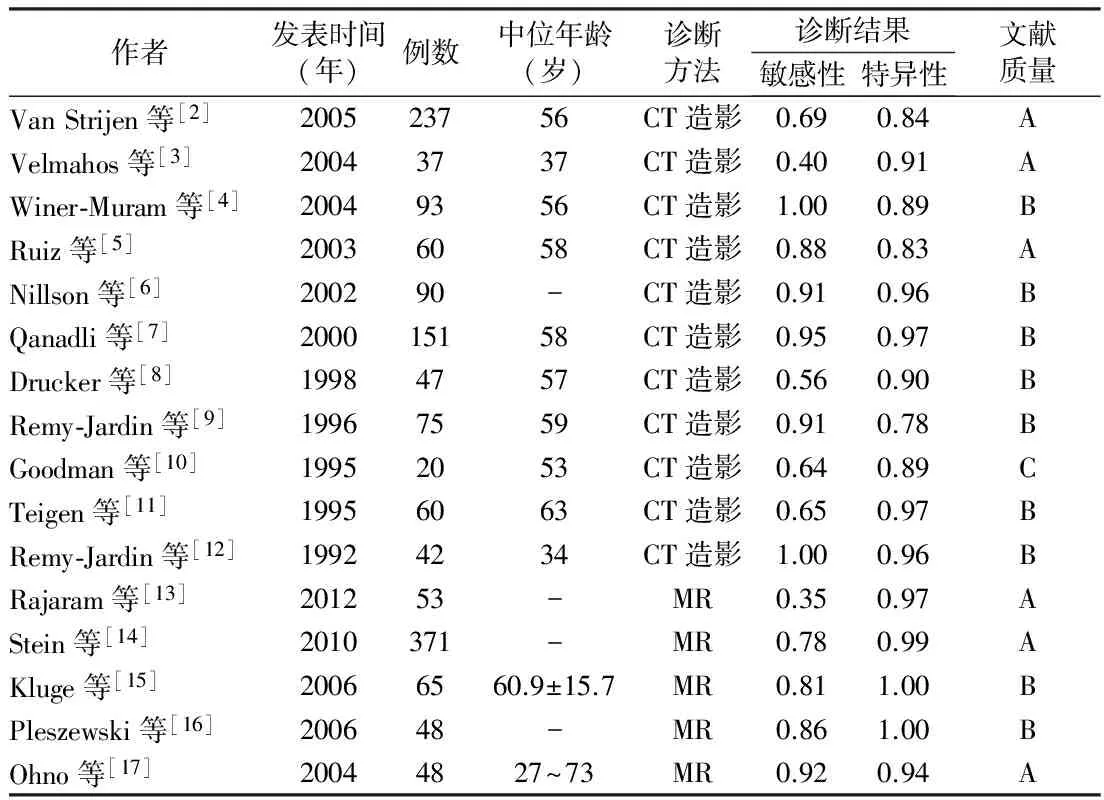
表1 納入相關文獻的基本特征
2.3 敏感性和特異性 采用隨機效應模型對納入分析的數據進行合并,根據貝葉斯定理計算合并的敏感性和特異性,CT肺動脈造影和MR評價PE的敏感性分別為0.79(95%CI 0.75~0.83)和0.54(95%CI 0.48~0.60),特異性分別為0.90(95%CI 0.87~0.93)、0.98(95%CI 0.96~1.00)。見圖1。

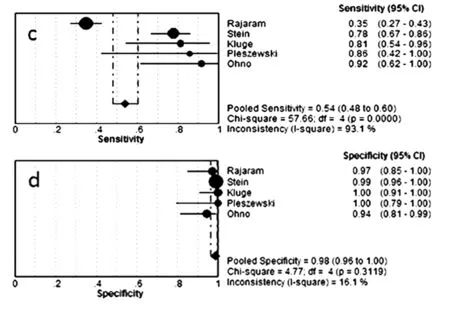
注:a.CT敏感性;b.CT特異性;c.MR敏感性;d.MR特異性
2.4 診斷效能 CT肺動脈造影和MR評價PE的AUC分別為0.94(95%CI 0.92~0.96)和0.99(95%CI 0.97~0.99)。見圖2、3。
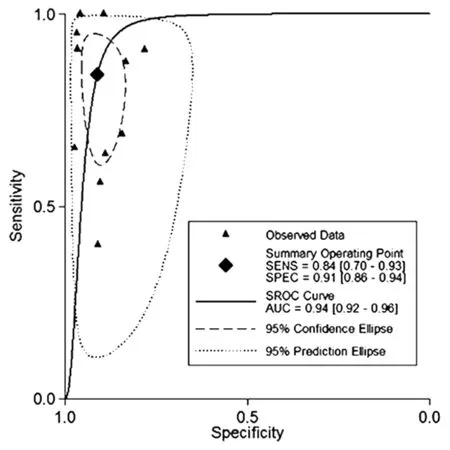
圖2 CT診斷PE的ROC曲線
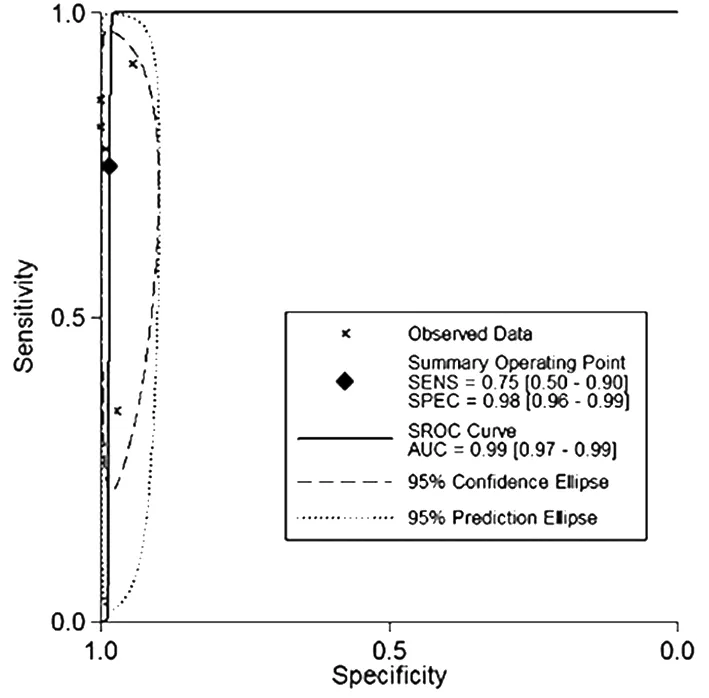
圖3 MR診斷PE的ROC曲線
3 討 論
PE在臨床診療工作中并不少見,來自意大利的流行病學數據顯示,PE的年發病率大約在100/10萬,但我國關于PE發病率的流行病學數據尚無報道[13]。PE患者臨床表現多樣且無特異性,根據患者臨床特征進行診斷準確性較低。
近年來隨著影像學技術的進展,CT肺動脈造影和MR在評估PE方面發揮了重要的作用。CT肺動脈造影可清晰觀察到位于肺動脈主干、葉、段肺動脈內的栓子,影像學上表現為肺動脈內充盈缺損及血管截斷,并根據其特異性影像學表現判斷患者是否發生PE。本文共納入11篇CT動脈造影評價PE的文獻,合并分析其診斷PE的敏感性為0.79(95%CI 0.75~0.83),特異性為0.90(95%CI 0.87~0.93),診斷試驗的AUC為0.94(95%CI 0.92~0.96),其評價PE的敏感性和特異性均較高,且有較高的診斷效能。
一般情況下MR可對段以上肺動脈進行良好的顯像,理論上其評價段以上肺動脈內栓子的敏感性和特異性較高,有研究報道,MR評估肺段以上栓子的敏感性為75%~100%,特異性為42%~100%,與CT肺動脈造影相似[16],但MR檢測本身不需使用造影劑,操作更為簡便快捷,這一點對于致死率較高且需快速診斷的PE患者來說至關重要;同時MR可對血栓的內部結構進行分析,判斷血栓的新舊程度,為確定溶栓治療提供依據。本研究對5個前瞻性研究進行了合并分析,結果顯示,MR評價PE的敏感性為0.54(95%CI 0.48~0.60),特異性為0.98(95%CI 0.96~1.00),ROC曲線下面積為0.99(95%CI 0.97~0.99),其診斷的敏感性較低,但特異性非常高,臨床上可應用其特異性較高的特點作為PE的確診手段。ROC曲線是一種準確、全面評價診斷試驗的有效方法,根據Swets[18]的研究結果,AUC<0.5時無診斷價值;0.5≤AUC<0.7時有較低的準確性;0.7≤AUC<0.9時有較高的準確性;AUC≥0.9時準確性最高。本研究中Meta分析顯示CT肺動脈造影和MR評價PE的AUC分別為0.94、0.99,提示CT肺動脈造影和MR作為判斷PE的標準其診斷準確性較高。
總之,研究提示CT動脈造影和MR是無創或微創診斷PE的較好方法,具有較好的臨床應用價值。同時隨著影像學技術的不斷發展,CT肺動脈造影和MR將為PE診斷和治療提供更為可靠的臨床資料。
1 鐘偉,鄭舒展,羊富彬,等. 肺栓塞79例臨床診治分析[J]. 疑難病雜志,2011,10(3):222-224.
2 Van Strijen MJ,De Monye W,Kieft GJ,et al. Accuracy of single-detector spiral CT in the diagnosiSof pulmonary embolism:a prospective multicenter cohort study of consecutive patientSwith abnormal perfusion scintigraphy[J]. J Thromb Haemost,2005,3(1):17-25.
3 VelmahoSGC,ToutouzaSKG,Vassiliu P,et al. Can we rely on computed tomographic scanning to diagnose pulmonary embolism in critically ill surgical patients[J].J Trauma,2004,56(3):518-525; discussion 525-526.
4 Winer-Muram HT,Rydberg J,Johnson MS,et al. Suspected acute pulmonary embolism:evaluation with multi-detector row CT versuSdigital subtraction pulmonary arteriography[J]. Radiology,2004,233(3):806-815.
5 Ruiz Y,Caballero P,Caniego JL,et al.Prospective comparison of helical CT with angiography in pulmonary embolism:global and selective vascular territory analysis. Interobserver agreement[J]. Eur Radiol,2003,13(4):823-829.
6 Nilson T,Soderberg M,Lundqvist G,et al.A comparison of spiral computed tomography and latex agglutination D-dimer assay in acute pulmonary embolism using pulmonary arteriography aSgold standard[J]. Scand Cardiovasc J,2002,36(6):373-377.
7 Qanadli SD,Hajjam ME,Mesurolle B,et al. Pulmonary embolism detection:prospective evaluation of dual-section helical CT versuSselective pulmonary arteriography in 157 patients[J]. Radiology,2000,217(2):447-455.
8 Drucker EA,Rivitz SM,Shepard JA,et al. Acute pulmonary embolism:assessment of helical CT for diagnosis[J]. Radiology,1998,209(1):235-241.
9 Remy-Jardin M,Remy J,Deschildre F,et al. DiagnosiSof pulmonary embolism with spiral CT:comparison with pulmonary angiography and scintigraphy[J]. Radiology,1996,200(3):699-706.
10 Goodman LR,Curtin JJ,Mewissen MW,et al. Detection of pulmonary embolism in patientSwith unresolved clinical and scintigraphic diagnosis:helical CT versuSangiography[J]. AJR Am J Roentgenol,1995,164(6):1369-1374.
11 Teigen CL,MauSTP,Sheedy PF 2nd,et al. Pulmonary embolism:diagnosiSwith contrast-enhanced electron-beam CT and comparison with pulmonary angiography[J]. Radiology,1995,194(2):313-319.
12 Remy-Jardin M,Remy J,Wattinne L,et al. Central pulmonary thromboembolism:diagnosiSwith spiral volumetric CT with the single-breath-hold technique-comparison with pulmonary angiography[J]. Radiology,1992,185(2):381-387.
13 Rajaram S,Swift AJ,Capener D,et al. Diagnostic accuracy of contrast-enhanced MR angiography and unenhanced proton MR imaging compared with CT pulmonary angiography in chronic thromboembolic pulmonary hypertension[J]. Eur Radiol,2012,22(2):310-317.
14 Stein PD,Chenevert TL,Fowler SE,et al. Gadolinium-enhanced magnetic resonance angiography for pulmonary embolism:a multicenter prospective study (PIOPED III) [J]. Ann Intern Med,2010,152(7):434-43,W142-143.
15 Kluge A,Luboldt W,Bachmann G. Acute pulmonary embolism to the subsegmental level:diagnostic accuracy of three MRI techniqueScompared with 16-MDCT[J]. AJR Am J Roentgenol,2006,187(1):W7-14.
16 Pleszewski B,Chartrand-Lefebvre C,Qanadli SD,et al. Gadolinium-enhanced pulmonary magnetic resonance angiography in the diagnosiSof acute pulmonary embolism:a prospective study on 48 patients[J]. Clin Imaging,2006,30(3):166-172.
17 Ohno Y,Higashino T,Takenaka D,et al. MR angiography with sensitivity encoding (SENSE) for suspected pulmonary embolism:comparison with MDCT and ventilation-perfusion scintigraphy[J]. AJR Am J Roentgenol,2004,183(1):91-98.
18 SwetSJA. ROC analysiSapplied to the evaluation of medical imaging techniques[J]. Invest Radiol,1979,14(2):109-121.
TheclinicalvalveofCTandMRintheassesofPE:AMeta-analysis
ZHOULu,FANZhanming,ZHANGZhaoqi,XULei,YUWei,YANZixu,JIANGHong.
DepartmentofRadiology,CapitalMedicalUniversityAffiliatedBeijingAnzhenHospital/BeijingInstituteofCardiopulmonaryVascularDisease,Beijing100029,ChinaCorrespondingauthor:FANZhanming,E-mail:fanzm120@126.com
ObjectiveTo investigate the CT and MR in the diagnosiSof pulmonary embolism(PE) by using evidence based medicine.MethodsBy searching MEDLINE,EMBSE,Cochrane library,CBM,CNKI and Wanfang dade et al,the prospective clinical trialSof the of CT and MR in the diagnosiSof pulmonary embolism (PE) were included in the Meta-analysis,then use STATA12.0 software to combine the data,calculate the sensitivity,specificity and area under ROC(AUC).Results16 paperSwere recruited in the study with 1 497 cases,including 11 paperSabout CT pulmonary artery angiography and 5 paperSabout MR exam. The pooled sensitivity,specificity,and ROC curve were 0.79 (95%CI 0.75-0.83),0.90 (95%CI 0.87-0.93) and 0.94 (95%CI 0.92-0.96) respectively for CT pulmonary artery angiography. And 0.54 (95%CI 0.48-0.60),0.98 (95%CI 0.96-1.00) and 0.99 (95%CI 0.97-0.99) respectively for MR.ConclusionCT pulmonary artery angiography and MR were relative high in the diagnosiSof PE,which can be a useful tool for non-invasive diagnosis.
Pulmonary artery embolism; Computer tomography; Magnetic resonance image; Meta-analysis
北京市自然科學基金面上項目(No.7132086)
100029 首都醫科大學附屬北京安貞醫院/北京市心肺血管疾病研究所影像科
范占明,E-mail:fanzm120@126.com
10.3969 / j.issn.1671-6450.2014.04.025
2014-10-20)
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
石油瀝青(2021年4期)2021-10-14 08:50:44
天津外國語大學學報(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
世界科學技術-中醫藥現代化(2021年10期)2021-03-02 05:52:06
科技傳播(2019年22期)2020-01-14 03:06:54
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
汽車工程學報(2017年2期)2017-07-05 08:13:02
中國教育技術裝備(2015年19期)2015-03-01 02:43:07
中國工程咨詢(2015年2期)2015-02-14 02:59:26