慢性阻塞性肺疾病患者急性加重頻率與高分辨率CT參數的相關性研究
2015-02-18 09:09:59王述紅黃小波何正光
中華肺部疾病雜志(電子版) 2015年3期
王述紅 黃小波 劉 翱 何正光
慢性阻塞性肺疾病患者急性加重頻率與高分辨率CT參數的相關性研究
王述紅1黃小波2劉翱3何正光1
慢性阻塞性肺疾病(chronic obstructive pulmonary disease, COPD)具有異質性的特點,在臨床工作中不難發現有部分患者,其肺功能測定氣流受限嚴重程度相似,然而對治療的反應、預后、急性加重頻率等相差甚遠[1-10]。COPD的急性加重,需要改變基礎的治療方案甚至需要住院治療,嚴重者需入住ICU搶救,反復發生急性加重是COPD患者死亡的主要原因。利用高分辨率CT(HRCT)重建圖像對COPD患者肺氣腫及支氣管管壁增厚程度進行評估,并將其分型,研究不同表型的特點,有助于指導臨床醫師進對患者行個體化治療[11-19]。本研究主要探討不同HRCT表型的COPD患者上一年急性加重次數的特點,及其與HRCT肺氣腫及支氣管管壁厚度參數的相關性,旨在為COPD患者的治療提供幫助。
資料與方法
一、一般資料
本研究納入2012年8月至2014年3月成都軍區昆明總醫院收治的臨床及肺功能檢查確診為COPD男性穩定期患者共159例,最終滿足要求的COPD患者共72例。年齡43~86歲,平均(68.11±8.52)歲。吸煙者65例(90.28%),吸煙量(52.85±30.29)包/年。其中肺功能1級者2例,2級者29例,3級者24例,4級者17例。病例入選標準:符合2011年COPD全球倡議(GLOD)診斷標準[20]。嚴格排除明確有肺部疾病、胸腔疾病及心功能不全者,全身各系統急性疾病狀態者,不能配合吸氣末屏氣下進行胸部HRCT掃描者。
二、方法
1. HRCT檢查及圖像分析: 采用GE公司Light Speed掃描儀。指導患者最大吸氣末屏氣,從肺尖到肺底行快速螺旋CT掃描。設置掃描電流220 mA,電壓120kV。肺窗采用Lung重建,縱膈窗采用Soft重建,重建圖像層距及層厚為0.625 mm。
在軸位圖像中,合格圖像的標準即無呼吸運動偽影。利用GE公司AW4.5工作站自帶軟件對Soft重建圖像進行圖像數據分析,通過軟件處理及人工校正,得到全肺的三維立體圖像,然后顯示CT值-面積曲線圖。將CT值設定低于-950HU的區域為肺氣腫區。方法為將平行于縱軸的直線移動至CT值為-950HU處,通過縱軸直接計算出圖像中CT值低于-950HU的區域所占整個肺體積的百分比,即為像素指數-950(PI-950),見圖1。
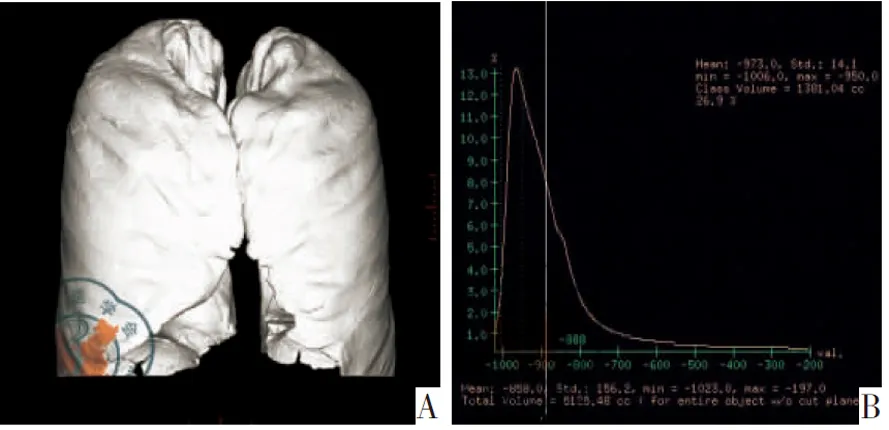
注:A:全肺三維立體圖;B:CT值-面積曲線圖
2.肺氣腫評估:選取3個解剖層面進行觀察,即靠近主動脈弓上緣1 cm、隆突水平下1 cm、右側橫膈上3 cm。三個解剖層面6個肺野中的密度減低區域面積(low attenuation areas, LAA)通過計算機自帶軟件,計算各層面LAA在該肺野中所占面積的比率。根據各層面LAA在該肺野中所占面積的比率進行LAA評分: 0分:LAA<5%,1分:5%≤LAA<25%,2分:25%≤LAA<50%,3分:50%≤LAA<75%,4分:LAA≥75%[21]。根據6個視野的評分總和對肺氣腫程度進行分級:0:總和為0分,1級:總和為1~6分,2級:總和為7~12分,3級:總和為13~18分,4級:總和為19~24分。將≥2級者定為肺氣腫型,見圖2。
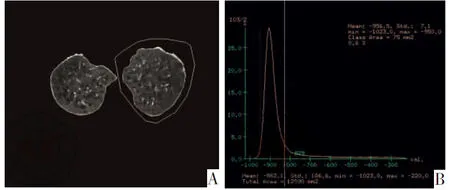
注:A:主動脈弓1 cm層面圈出右肺野;B:CT值-面積曲線圖
3.采用Roberts等[22]評估方法對支氣管管壁增厚程度進行評估。支氣管管壁厚度/相鄰肺動脈直徑<30%定為0級,30%≤支氣管管壁厚度/相鄰肺動脈直徑<50%定為1級,支氣管管壁厚度/相鄰肺動脈直徑≥50%定為2級。將≥1級者定為支氣管管壁增厚型。
4.HRCT分型:結合兩者綜合分型將患者分為A型、E型、M型三型,A型:LAA≤1級,支氣管管壁厚度評估<1級;E型:LAA≥2級,支氣管管壁厚度評估<1級;M型:LAA≥2級,支氣管管壁增厚≥1級。
三、統計學方法

結果
一、 COPD患者HRCT參數及表型
所有受檢者在整個檢查過程中配合較好,順利完成HRCT掃描,均獲得了分析圖像。最終入組72例COPD患者,入組患者過去一年中急性加重次數0~3次,平均為(1.50±0.95)次;像素指數PI-950的數據范圍為(0.4~43.10)%,中位數為18.75%;支氣管管壁厚度/相鄰肺動脈的數據范圍為(17.48~41.53)%,中位數為28.35%。按HRCT參數分型,無肺氣腫型32例,肺氣腫型40例;無支氣管管壁增厚型40例,支氣管管壁增厚型32例;A型32例,E型19例,M型21例
二、 COPD患者HRCT參數與急性加重次數的相關性分析
相關性分析顯示,HRCT參數PI-950和支氣管管壁厚度/相鄰肺動脈直徑比值與上一年急性加重頻率均呈正相關(r=0.28,P=0.017;r=0.416,P=0.000)。
三、不同HRCT表型患者的急性加重次數的比較
肺氣腫型患者平均上一年急性加重次數為(1.83±0.81)次,顯著高于無肺氣腫型(1.09±0.96)次(t=3.494,P=0.001);支氣管管壁增厚型患者急性加重次數為(1.81±0.86)次,顯著高于無支氣管管壁增厚型(1.25±0.95)次(t=2.597,P=0.011);A型患者急性加重次數為(1.09±0.96)次,顯著低于E型(1.63±0.761)次及M型(2.00±0.84)次(q=3.006,P<0.05;q=5.225,P<0.001),E型與M型之間比較差異無統計學意義(q=1.884,P>0.05)。
討論
在20世紀60年代已有學者提出對COPD進行分型[23],西塞爾內科學也曾對A型(肺氣腫型)和B型(紫腫型)提出過鑒別。近年來,隨著Han等[24]對COPD表型概念的提出,表型已成為目前COPD研究的熱詞。通過肺結構的改變(如肺氣腫、氣道壁厚度和支氣管擴張程度等)可預測患者對治療的反應及預后。由于胸部HRCT可評估肺氣腫及氣道病變,目前HRCT已被應用于COPD表型的研究[25]。采用密度減低區域面積對肺氣腫程度進行評估,通過測量患者支氣管管壁厚度/相鄰肺動脈直徑,可判別支氣管管壁增厚程度。考慮LAA評分只針對3個解剖層面6肺野進行評估,存在一定誤差,因此本研究選擇PI-950作為代表肺氣腫量化的指標,進行相關性分析。入選的72例患者,按肺氣腫程度分為無肺氣腫型32例,肺氣腫型40例;按支氣管管壁增厚程度分為無支氣管管壁增厚型40例,支氣管管壁增厚型32例;結合兩者分為A型32例,E型19例,M型21例。
本研究中肺氣腫型及支氣管管壁增厚型的患者COPD急性加重頻繁,A型的患者急性加重頻率低。E型與M型兩者間進行比較,其過去一年中急性加重次數無統計學意義。有研究發現COPD急性發作頻率及急性加重次數分別與肺氣腫占雙肺的百分比、段支氣管管壁厚度呈正相關[26]。本研究中PI-950、支氣管管壁厚度/相鄰肺動脈直徑比值上一年度越明顯,其急性加重越頻繁,患者肺功能下降速度越快,生活質量越差。有實驗數據顯示以肺氣腫和氣道壁增厚為主的表現型存在家庭聚集現象,同時發現兩者之間呈負相關[27]。因此,E、M型兩型急性加重頻率未發現統計學差異,需要進一步加大樣本進行研究。同時提示對其機制行深入分析,尋找其主要影響因素,阻斷主要影響因素可能會減少患者急性加重頻率。
總之,COPD患者PI-950及支氣管管壁厚度/相鄰肺動脈直徑比值與上一年急性加重次數呈正相關。HRCT表型為肺氣腫型及支氣管管壁增厚型的患者COPD急性加重頻繁,A型的患者急性加重頻率較低。因此,對于肺實質破壞和/或支氣管管壁增厚明顯的患者,應積極采用多種措施,對肺氣腫為主的患者可采用多種支氣管擴張劑聯合治療。小劑量阿奇霉素長期口服治療支氣管管壁增厚型COPD患者,可以減輕氣道炎癥,減緩肺功能下降速率,并減少急性加重頻率,提高生活質量[28]。本研究采用手動測量支氣管管壁增厚程度,選擇測量支氣管也不盡相同,測量中存在個人差異,因此,需進一步探索更客觀統一的測量方法。
參考文獻
1任成山. 慢性阻塞性肺疾病發病機制研究現狀與展望[J/CD]. 中華肺部疾病雜志:電子版, 2009, 2(2): 104-115
2Young RP, Hopkins RJ, Christmas T, et al. COPD prevalence is increased in lung cancer, independent of age, sex and smoking history[J]. Eur Respiratory J, 2009, 34(2): 380-386.
3Kiri VA, Soriano J, Visick G, et al. Recent trends in lung cancer and its association with COPD: an analysis usig the UK GP Research Database[J]. Prim Care Respir J, 2010, 19(1):57-61.
4Yamada Y, Sekine Y, Suzuki H, et al. Trends of bacterial colonisation and the risk of postoperative pneumonia in lug cancer patients with chronic obstrucive pulmonary disease[J]. Eur J Cardiothorac Surg, 2010, 37: 752-757.
5Raviv S, Hawkins KA, DeCamp MM Jr, et al. Lung cancer in chronic obstructive pulmonary disease:enhancing surgical options and outcomes[J]. Am J Respir Crit Care Med, 2011, 183(9): 1138-1146.
6Sundar IK, Mullapudi N, Yao H, et al. Lung cancer and its association with chronic obstructive pulmonary disease: update on nexus of epigenetics[J]. Cur Opin Pulm Med, 2011, 17(4): 279-285.
7Caremori G, Casolari P, Casolari P, et al. Mecha-nisms involved in lung cancer development in COPD[J] . The International Journal of Bichemistry &cell Biology, 2011, 43(7): 1030-1044.
8Rooney C, Sethi T. The epithelial cell and lung cancer: the link between chronic obstructive pulmonary diseases and lung cancer[J]. Respiration, 2011, 81(2): 89-104.
9Young RP, Hopkins RJ. How the genetics of lung cancer may overlap with CIPD[J]. Respirology, 2011, 16(7): 1047-1055.
10Zuiueta JJ, Wisnivesky JP, Henschke CI, et al. Emphysema scores predict death from COPD and lung cancer[J]. Chest, 2012, 141(5), 1216-1223.
11Matsumoto H, Niimi A, Tabuena RP,etal. Airway wall thickening in patients with cough variant asthma and nonasthmatic chronic cough[J]. Chest,2007, 131(4): 1042-1049.
12Niimi A, Matsumoto H, Amitani R,etal. Effect of short-term treatment with inhaled corticosteroid on airway wall thickening in asthma[J]. Am Med,2004, 116(11): 725-731.
13Nakano Y, Muro S, Sakai H,etal. Computed tomographic measurements of airway dimensions and emphysema in smokers. Correlation with lung function[J]. Am J Respir Crit Care Med,2000, 162(3 Pt 1): 1102-1108.
14Hoshino M, Matsuoka S, Handa H,etal. Correlation between airflow limitation and airway dimensions assessed by multidetector CT in asthma[J]. Respir Med,2010, 104(6): 794-800.
15Harmanci E, Kebapci M, Metintas M,etal. High-resolution computed tomography findings are correlated with disease severity in asthma[J]. Respiration,2000, 69(5): 420-426.
16Shaw RJ, Djukanovic R, Tashkin DP,etal. The role of small airways in lung disease[J]. Respir Med,2002, 96(2): 67-80.
17Yamashiro T, Matsuoka S, Bartholmai BJ,etal. Collapsibility of lung volume by paired inspiratory and expiratory CT scans: correlations with lung function and mean lung density[J]. Acad Radiol,2010, 17(4): 489-495.
18Mesia-Vela S, Yeh CC, Austin JH,etal. Plasma carbonyls do not correlate with lung function or computed tomography measures of lung density in older smokers[J]. Biomarkers,2008, 13(4): 422-434.
19Guerra S. Asthma and chronic obstructive pulmonary disease[J]. Curr Opin Allergy Clinical,2009, 9(5): 409-416.
20GOLD Executive Committee. Global strategy for the diagnosis, management,and prevention of chronic obstructive pulmonary disease(Revised 2011 ). http://www.goldcopd.com.
21Kitaguchi Y, Fujimoto K, Kubo K, et al. Characteristics of COPD phenotypes classified according to the findings of HRCT[J]. Respir Med, 2006, 100(10): 1742-1752.
22Roberts HR, Wells AU, Milne DG, et al. Airflow obstruction in bronchiectasis correlation between computed tomography features and pulmonary function tests[J]. Thorax, 2000, 55(3): 198-204.
23Burrows BE, Fletcher CM, Heard BE, et al. The emphysematous and bronchial type of chronic airways obstruction.A clincopathological study of patients in London and Chicago[J]. Lancet, 1966, 1(7442): 830-835.
24Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pulmonary disease phenotypes: the future of COPD[J]. Am J Respir Crit Care Med, 2010, 182(5): 598-604.
25黃宇婷, 劉翱. HRCT定量測量與慢性阻塞性肺疾病表型的關系[J/CD]. 中華肺部疾病雜志: 電子版, 2015, 8(2): 251-253.
26Kim V, Han MK, Vance GB, et al. The chronic bronchitic phenotype of COPD: an analysis of the COPD Gene Study[J].Chest, 2011, 140(3): 626-633.
27Patel BD, Coxson HO, Pillai SG, et al. Airway wall thickening and emphysema show independent familial aggregation in chronic obstructive pulmonary disease[J]. Am J Respir Crit Care Med, 2008, 178(5): 500-505.
28Albert RK, Connett J, Bailey WC, et al. Azithromycin for prevention of exacerbations of COPD[J]. N Engl J Med, 2011, 365(8): 689-698.
(本文編輯:王亞南)
王述紅,黃小波,劉翱,等. 慢性阻塞性肺疾病患者急性加重頻率與高分辨率CT參數的相關性研究[J/CD]. 中華肺部疾病雜志: 電子版, 2015, 8(3): 308-312.
·論著·
【摘要】目的探討不同高分辨率CT(HRCT)表型慢性阻塞性肺疾病(COPD)患者上一年急性加重次數的特點,及與HRCT參數的相關性。 方法收集COPD穩定期患者159例,對最終滿足標準的72例COPD患者完成HRCT檢查,并記錄上一年急性加重次數。根據HRCT影像中肺氣腫程度或(和)支氣管管壁增厚情況進行分型,并測定PI-950和支氣管管壁厚度與相鄰肺動脈直徑的比值。結果COPD表型分別為:無肺氣腫型32例,肺氣腫型40例;無支氣管管壁增厚型40例,支氣管管壁增厚型32例;A型32例,E型19例,M型21例。COPD患者的HRCT參數EI和支氣管管壁厚度/相鄰肺動脈直徑比值與上一年急性加重頻率均呈正相關(r=0.28,P=0.017; r=0.416,P=0.000)。HRCT表型為肺氣腫型的患者平均上一年急性加重次數為(1.83±0.81)次,高于無肺氣腫型[(1.09±0.96)次,P=0.001];支氣管管壁增厚型患者急性加重次數為(1.81±0.86)次,高于無支氣管管壁增厚型[(1.25±0.95)次,P=0.011)];A型急性加重次數為(1.09±0.96)次,低于E型及M型[(1.63±0.761)次,(2.00±0.84)次,P=0.002],E型與M型之間比較差異無統計學意義。結論COPD患者PI-950及支氣管管壁厚度/相鄰肺動脈直徑比值與上一年急性加重次數呈正相關。HRCT表型多為肺氣腫型及支氣管管壁增厚型的患者,且COPD急性加重頻繁,而A型患者的急性加重頻率較低。
【關鍵詞】肺疾病,慢性阻塞性;CT,高分辨率;頻率,急性加重;表型
Correlation of high-resolution CT data with the number of exacerbation in patients with chronic obstructive pulmonary diseaseWangShuhong1,HuangXiaobo2,LiuAo3,HeZhengguang1.1DepartmentofRespiratoryMedicine,CentralHospitalofSuining,Suining629000,China;2DepartmentofRadiology,KunmingGeneralHospitalofChengduMilitaryCommandofChinesePLA,Kunming650032,China;3DepartmentofRespiratoryMedicine,KunmingGeneralHospitalofChengduMilitaryCommandofChinesePLA,Kunming650032,China)
Correspondingauthor:LiuAo,Email:ynkm43@126.com
【Abstract】ObjectiveTo classify the high resolution computed tomography (HRCT) phenotypes of chronic obstructive pulmonary disease (COPD) , and to investigate the acute exacerbation frequency characteristics of various phenotypes and the relationship with HRCT parameters. Methodsseventy-two consecutive COPD patients underwent HRCT and their the number of acute exacerbations last year were recorded. COPD subjects were classified into different phenotypes based on the visual HRCT findings (with or without emphysema and/or bronchial wall thickening).With the volumetric HRCT data, the total lung volume(TLV) was calculated automatically by Extended Brilliance WorkspaceTM, the total emphysema volume(TEV) was obtained by applying density thresholds of -950HU, and the TEV/TLV was calculated as an emphysema index(EI). Emphysema threshold was set to -950HU, then find out the corresponding percentage, it was the pixel index-950(PI-950). We measured the bronchial wall thickness and the adjacent pulmonary artery diameter and calculated their ratio. ResultsWe divided the cases into different phenotypes: emphysematous phenotype (40 cases), non-emphysematous phenotype (32 cases); bronchial wall thickening phenotype(32 cases) and non-bronchial wall thickening phenotype(40 cases); A phenotype(32 cases), E phenotype (19 cases), M phenotype (21 cases). The PI-950 and the ratio of bronchial wall thickening and adjacent pulmonary artery diameter were positively correlated with the number of acute exacerbation history in previous year(r=0.28,P=0.017; r=0.416,P=0.000). The number of acute exacerbation history in previous year of non-emphysematous phenotype and emphysematous phenotype is 1.09±0.96, 1.83±0.81 respectively, and has statistical difference (t=-3.494, P=0.001). Non-bronchial wall thickening phenotype and bronchial wall thickening phenotype is 1.25±0.95, 1.81±0.86 respectively, and has statistical difference (t=-2.597, P=0.011). A phenotype is 1.09±0.96, E phenotype is 1.63±0.76 and M phenotype is 2.00±0.84.There is significant difference among three phenotypes (F=7.051, P=0.002). Comparison between two groups, there are differences between A phenotype and two other groups, no differences between E phenotype and M phenotype. ConclusionThe PI-950 and the ratio of bronchial wall thickening and adjacent pulmonary artery diameter are positively correlated with the number of acute exacerbation history in previous year in COPD patients. The number of acute exacerbation of emphysematous phenotype and bronchial wall thickening phenotype compared with non-emphysematous phenotype and non-bronchial wall thickening phenotype have more frequently. HRCT phenotype A compared with phenotype B and C is associated with a lower the acute exacerbation frequency in COPD patients.
【Key words】Chronic obstructive pulmonary disease;High resolution computed tomography (HRCT);Acute exacerbation frequency;Phenotype
收稿日期:(2014-08-26)
文獻標識碼:中圖法分類號: R563 A
通訊作者:劉翱, Email: ynkm43@126.com
DOI:作者單位: 629000 四川,遂寧市中心醫院呼吸內科1;650032 昆明,成都軍區昆明總醫院影像科2、呼吸內科3