腹腔鏡子宮肌瘤切除術的臨床價值分析
2015-12-08 02:46:32江向潔
中外醫療 2015年27期
關鍵詞:腹腔鏡
江向潔
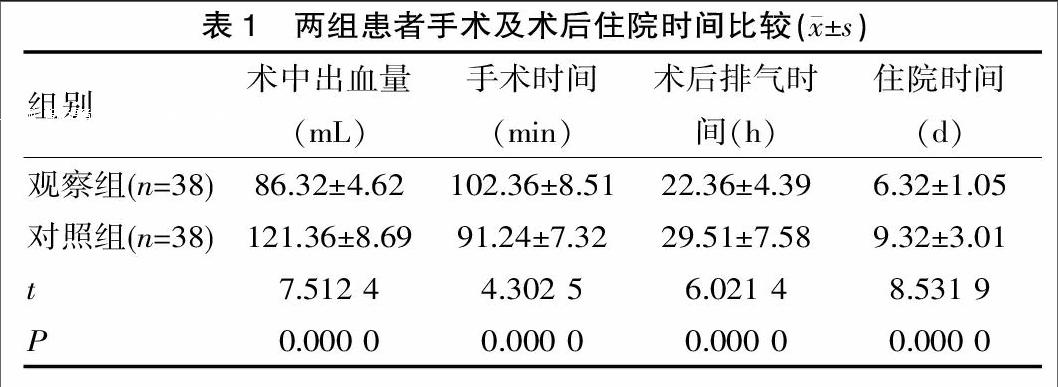
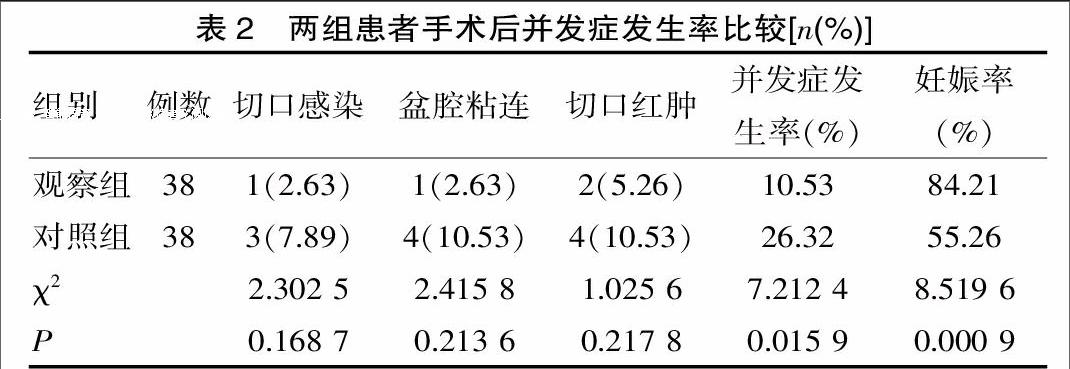
[摘要] 目的 探討腹腔鏡子宮肌瘤切除術的治療效果及臨床應用價值。 方法 整群選擇該院2013年2月—2014年2月間收治的76例子宮肌瘤患者為研究對象,隨機分為對照組38例,實施傳統開腹子宮肌瘤切除術治療,觀察組38例,實施腹腔鏡子宮肌瘤切除術治療,對兩組患者手術情況及術后恢復情況進行分析。 結果 觀察組術手術時間較對照組長,但是術中出血量較低,術后排氣時間及住院時間明顯較對照組短,差異有統計學意義(P<0.05);觀察組術后出現切口感染、盆腔粘連、切口紅腫等并發癥發生率為10.53%,較對照組26.32%低,差異有統計學意義(P<0.05),觀察組術后妊娠率為84.21%,明顯較對照組55.26%高(P<0.05)。 結論 子宮肌瘤采取腹腔鏡子宮肌瘤切除術的創傷較小,并發癥較少,可利于術后快速恢復,減少患者痛苦,提高術后妊娠率,值得推廣。
[關鍵詞] 子宮肌瘤;腹腔鏡;開腹手術
[中圖分類號] R5 [文獻標識碼] A [文章編號] 1674-0742(2015)09(c)-0059-03
[Abstract] Objective To study the therapeutic effect and clinical value of laparoscopic myomectomy. Methods 76 patients with uterine fibroids admitted to this hospital between February 2013 and February 2014 were randomized to undergo traditional open surgery (the control group, n=38) and laparoscopic myomectomy (the observation group,n=38). We analyzed the operation and postoperative recovery of the two groups. Results The operation duration was longer, but the intraoperative blood loss and postoperative exhaust time and hospital stay were shorter in the observation group than in the control group, and the differences were statistically significant, P<0.05; the rate of complications including incision infection, pelvic adhesion, incision inflammation(10.53% vs 26.32%) was lower in the observation group than in the control group, and the difference was statistically significant, P<0.05; the postoperative pregnancy rate (84.21% vs 55.26%) was significant higher in the observation group than in the control group with statistical difference, P<0.05. Conclusions With less trauma and complications, laparoscopic myomectomy in the treatment of uterine fibroids is conducive to rapid postoperative recovery and can reduce the patients' pain and improve pregnancy rate, therefore it is worthy of promotion.
[Key words] Uterine fibroids; Laparoscope; Open operation
子宮肌瘤是常見女性生殖器官良性腫瘤,患者主要表現為下腹墜脹、腹部包塊、壓迫及子宮出血。子宮肌瘤發病率極高,特別是中年女性,發病率達75%左右,嚴重影響女性的生活質量及生殖健康[1]。子宮肌瘤主要采取積極手術方案切除治療,以往主要實施開腹切除術,創傷大,術后并發癥較多,導致術后恢復較慢,不利于術后恢復。隨著外科微創技術的不斷發展,腹腔鏡手術開始逐漸應用于臨床,其創傷小,安全性高,作為首選子宮肌瘤手術方案[2]。該組研究對子宮肌瘤患者分別實施開腹手術及腹腔鏡手術治療,現報道如下。
1 資料與方法
1.1 一般資料
整群選擇該院2013年2月—2014年2月收治的76例子宮肌瘤患者為研究對象,所有患者均符合《實用婦科學》[3]中子宮肌瘤診斷標準。隨機分為對照組38例,觀察組38例,觀察組:年齡23~47歲,平均年齡(31.5±4.7)歲;孕次0~6次,平均孕次(2.3±0.5)次;單發肌瘤23例,多發肌瘤15例;對照組:年齡24~48歲,平均年齡(31.1±4.2)歲;孕次0~5次,平均孕次(2.6±0.7)次;單發肌瘤21例,多發肌瘤17例;納入標準:符合子宮肌瘤診斷標準;與該組研究配合;18~60歲;排除標準:嚴重免疫性疾病及血液疾病者;心、腎、肝功能不全者;妊娠期、哺乳期女性。兩組患者一般資料差異無統計學意義(P>0.05),存在可比性。
1.2 方法
兩組患者均實施氣管插管全麻,對照組:根據病灶位置選擇切口,分離肌瘤系膜,直接切除,隨后徹底止血、清洗腹腔,最后逐層縫合創口;觀察組:取膀胱截石位,臍窩部縱形切口,置入套管及腹腔鏡設備,分別取兩側操作孔,置入腹腔鏡設備,使用6U垂體后葉素注入肌瘤切口部位,經縱軸切開肌瘤表面基層,直至瘤體,肌瘤作完整剝離后,使用雙極電凝止血。瘤腔縫合時,使用可吸收線作切緣內翻卷折填充瘤窩縫合法,可起到壓迫止血作用,保持創面平滑。
猜你喜歡
腹腔鏡外科雜志(2022年7期)2022-08-16 04:31:06
臨床醫藥文獻雜志(電子版)(2017年11期)2017-05-17 04:48:17
中國內鏡雜志(2017年2期)2017-03-20 16:18:12
實用臨床醫學(2016年8期)2016-06-08 06:10:09
腹腔鏡外科雜志(2016年11期)2016-06-01 12:10:09
腹腔鏡外科雜志(2016年9期)2016-06-01 12:10:07
中國衛生標準管理(2015年16期)2016-01-20 09:27:19
中國醫療器械雜志(2015年5期)2015-12-31 06:15:30
衛生職業教育(2014年16期)2014-05-16 03:48:30
西南軍醫(2014年1期)2014-02-03 03:06:16
