奧美沙坦抑制低滲液誘導的豚鼠心房肌細胞I Ks電流增加和動作電位時程縮短
2015-12-16 08:27:38劉傳鎬西安交通大學第二附屬醫院干部二病區西安7000西安交通大學第一附屬醫院干五病區西安交通大學醫學部藥理學系西安交通大學醫學部機能教學中心通訊作者mailshengyingmailxjtueducn
山西醫科大學學報 2015年4期
高 潔,盛 嬰,葉 莎,劉傳鎬,趙 進(西安交通大學第二附屬醫院干部二病區,西安 7000;西安交通大學第一附屬醫院干五病區;西安交通大學醫學部藥理學系;西安交通大學醫學部機能教學中心;通訊作者,E-mail:shengying@mail.xjtu.edu.cn)
越來越多資料表明[1-4],腎素-血管緊張素系統(renin-angiotensin system,RAS)與實驗性房性心律失常的發生有關。最新的臨床研究也發現[5-10],RAS阻滯劑包括血管緊張素轉換酶(ACE)抑制劑和1型血管緊張素Ⅱ受體(AT1R)阻滯劑能夠有效治療房顫。然而,此類藥物治療房顫的機制尚未完全闡明,特別是對房顫發生的心臟電生理特性影響更是知之甚少。
心肌細胞動作電位時程(APD)和有效不應期(ERP)的縮短通常被認為是以折返為基礎的房顫發生的關鍵因素。房顫發生期間,心房收縮功能受損造成心房肌細胞腫脹或牽張[11,12],血管緊張素Ⅱ分泌增加[13,14]。Zankov 等[15]證實,外源性血管緊張素Ⅱ和低滲液誘導的豚鼠心肌細胞膜擴張可增加心肌細胞緩慢整流性外向鉀電流 (slow delayed outward rectifying potassium channel,IKs)并使心房肌細胞APD縮短,此作用是通過激活心房肌細胞AT1受體來實現的。這表明AT1受體激活后引發的IKs電流增強和心房肌細胞APD縮短在房顫的發生及維持中起著重要作用[15,16]。Moreno 等報道,AT1受體阻滯劑厄貝沙坦(irbesartan)能夠抑制異源表達的KCNQ1/KCNE1通道電流[17],此結果提示1型血管緊張素Ⅱ受體(AT1R)阻滯劑有可能是通過阻滯AT1受體來產生治療房顫作用的。
本研究觀察了選擇性AT1R阻滯劑奧美沙坦(olmesartan)對低滲液(Hypo-S)誘導的豚鼠心房肌細胞IKs電流增強和APD縮短的影響。結果 表明,奧美沙坦對擴張豚鼠心房細胞膜誘導的電生理變化與阻斷AT1受體有關,這可能就是AT1R阻滯劑治療房顫的重要作用機制之一。
1 材料和方法
1.1 豚鼠心房肌細胞分離
成年Hartley豚鼠,體重(300±25)g,雌雄兼用。腹腔注射戊巴比妥鈉40 mg/kg麻醉后,采用Langendorff灌流裝置灌注豚鼠心臟,酶法分離單個心房肌細胞[16]。
1.2 溶液和藥品
標準臺氏液:即“等滲”細胞外液(Iso-S,平均滲透壓 285 mOsm/kg)包括 140 mmol/L NaCl、5.4 mmol/L KCl、1.8 mmol/L CaCl2、0.5 mmol/L MgCl2、0.33 mmol/L NaH2PO4、5.5 mmol/L 葡萄糖和 5.0 mmol/L HEPES(用1 mol/L NaOH將pH調節至7.4)。“低滲”細胞外液(Hypo-S,平均滲透壓 ~210 mOsm/kg):將標準臺式液中NaCl濃度降至100 mmol/L 即可,余相同[17]。
奧美沙坦(Sigma-Aldrich公司,美國),先用二甲亞砜(DMSO,Sigma公司,美國)配制成7 mmol/L的母液,臨用前再用標準臺氏液或“低滲”細胞外液稀釋成所需濃度。DMSO在灌流浴槽中的終濃度<0.1%(V/V),對 IKs電流無影響。
電極內液:70 mmol/L門冬氨酸鉀、50 mmol/L KCl、10 mmol/L KH2PO4、1 mmol/L MgSO4、3 mmol/L Na2ATP(Sigma 公司,美國)、0.1 mmol/L Li2GTP(羅氏診斷有限公司,曼海姆,德國)、5 mmol/L EGTA和5 mmol/L HEPES(用1 mol/L KOH將pH調節至 7.2)。
1.3 電生理記錄和數據分析
將分離好的心房肌細胞置于安裝在倒置顯微鏡上的5 ml灌流浴槽中,(36±1)℃恒溫下1-2 ml/min灌流細胞外液。觀察藥物作用時,將灌流液換成用標準臺氏液或“低滲”液稀釋成所需濃度藥物。實驗分別觀察了1 μmol/L和7 μmol/L奧美沙坦對豚鼠心房肌細胞IKs影響。采用EPC-8膜片鉗放大器(HEKA Electronics,Lambrecht,Germany)全細胞記錄心房肌細胞電流或電壓。采樣頻率2 kHz,數據信號經5 kHz的低通濾波器后,LIH-1600型數模轉換器(HEKA)輸入計算機,PATCHMASTER軟件(HEKA)處理數據。硼硅玻璃電極充灌電極內液后電阻值2.5-4.0 MΩ。觀察IKs電流時采用從鉗制電位-50 mV去極化至不同的測定電位。通過設置鉗制電位-50 mV使鈉通道失活,分別將0.4 μmol/L尼索地平(nisoldipine,拜耳公司,德國)和 0.5 μmol/L多非利特(dofetilide,Sigma公司,美國)加入到細胞外液中阻斷L型Ca2+通道(ICa,L)和快速整流性外向鉀電流(rapidly delayed outward rectifying potassium channel,IKr)。
測定IKs電流時,先去極化至+30 mV(刺激波寬2 s,間隔10 s),以復極至-50 mV時的尾電流作為IKs電流幅度并據此測定電流時程。通過Boltzmann方程 IK,tail=1/[1+exp((Vh– Vm)/k)]擬合 IKs尾電流的電流-電壓關系來測定IKs的電壓依賴性激活關系,其中IK,tail是尾電流值,Vh是半效最大激活電位,Vm是測定電位,k是斜率。利用單指數方程擬合尾電流曲線來測定IKs通道的去活化時間常數。細胞膜電容(Cm)測定采用波寬20 ms、振幅±5 mV脈沖對細胞施加刺激,然后利用公式Cm=τCI0/ΔVm(1-Iss/I0)求出膜電容。其中τC是電容瞬態時間常數,I0是初始峰電流,Iss是穩態電流值,ΔVm為刺激電壓幅度(5 mV)。鉗制電流模式下,通過記錄電極對心房細胞施加頻率0.2 Hz、波寬2 ms的閾上刺激誘發動作電位(AP)。以復極90%的動作電位時間作為動作電位時程(APD90)。
1.4 統計學分析
2 結果
2.1 奧美沙坦不影響基礎I Ks電流,但可減弱Hypo-S誘導的I Ks增強
圖1A顯示,將灌流液換成低滲液Hypo-S時,心房肌細胞IKs尾電流明顯增加。其中第二次將灌流液換成 Hypo-S液之前,預先在浴槽中加入7 μmol/L奧美沙坦處理心房肌細胞。結果 表明,1 μmol/L和7 μmol/L奧美沙坦不影響豚鼠心房肌細胞的基礎IKs電流(圖1B中1和3分別為圖1A中的時間點測得IKs電流曲線),Hypo-S明顯增加IKs穩態及尾電流幅度(圖1B所示電流曲線2和4)。
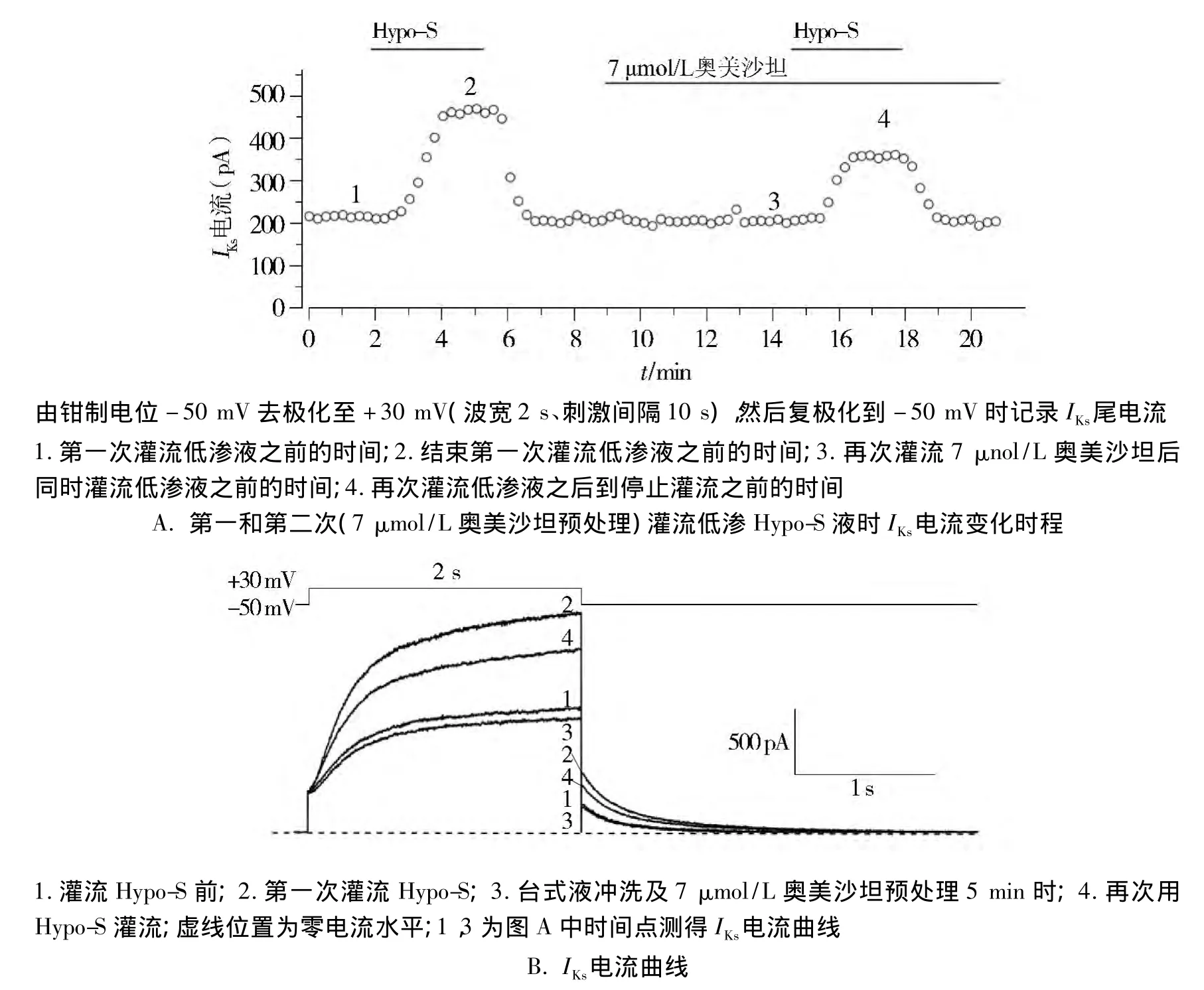
圖1 奧美沙坦不影響豚鼠心房肌細胞的基礎I Ks電流Figure 1 Olmesartan did not affect baseline I Ks in guinea-pig atrial myocytes
圖2A和圖2B分別顯示灌流低滲液Hypo-S及Hypo-S+1 μmol/L奧美沙坦時,采用臺階刺激(鉗制電位-50 mV,步幅10 mV)去極化至+50 mV時所獲得的典型IKs電流曲線。圖2C為灌流Hypo-S、Hypo-S+1 μmol/L 奧美沙坦和 Hypo-S+7 μmol/L奧美沙坦三種不同條件下IKs電流增加百分率。結果 表明,Hypo-S、Hypo-S+1 μmol/L 奧美沙坦和 Hypo-S+7 μmol/L奧美沙坦的IKs電流增加的百分率分別為(105.60 ± 10.25)%(n=22),(70.64 ±9.39)%(n=11,與 Hypo-S 比較,P <0.05)和(68.22 ±8.52)%(n=14,與 Hypo-S 比較,P <0.05)。方差分析結果表明,Hypo-S+奧美沙坦的IKs電流增加百分率明顯低于單純Hypo-S(圖2C)。圖2 D為灌流 Iso-S、Hypo-S和 Hypo-S+1 μmol/L奧美沙坦時IKs電流-電壓關系曲線。利用Boltzmann方程對曲線進行擬合,求出Iso-S、Hypo-S及Hypo-S+1 μmol/L奧美沙坦三種不同條件下IKs通道的半效激活電壓(Vh)分別為(9.06 ±1.28)mV(n=22)、(2.08 ±1.29)mV(n=13,與 Iso-S 比較,P < 0.01)及(2.10 ±1.40)mV(n=10,與 Iso-S 比較,P <0.01)。結果 顯示,Hypo-S可使激活曲線明顯向左偏移,即低滲使IKs通道更加容易開放,但奧美沙坦不能使之改變。
表1顯示了1 μmol/L奧美沙坦在四種不同復極化電位下對IKs通道去活化時間常數的影響。Hypo-S明顯減慢-60 mV到-30 mV電位之間的IKs電流去活化時間,而奧美沙坦對Hypo-S的作用并無明顯影響(P >0.05)。
2.2 奧美沙坦減弱Hypo-S誘導的豚鼠心房肌細胞動作電位縮短
圖3A-3C分別顯示了Iso-S和Hypo-S(對照組,圖 3A)、Iso-S 和 Hypo-S+1 μmol/L 奧美沙坦(圖3B)、Iso-S 和 Hypo-S+7 μmol/L 奧美沙坦(圖3C)三組豚鼠心房肌細胞動作電位。圖3D條形圖顯示,Hypo-S使心房肌細胞APD90縮短了(20.22±1.28)%(n=15),而 Hypo-S+1 μmol/L 奧美沙坦和Hypo-S+7 μmol/L奧美沙坦則分別僅使APD90縮短(11.89±1.15)%(n=11,與對照組比較,P <0.01)、(11.56 ±1.23)%(n=12,與對照組比較,P<0.01)。以上結果說明1-7 μmol/L奧美沙坦可對抗Hypo-S引發的心房動作電位縮短。
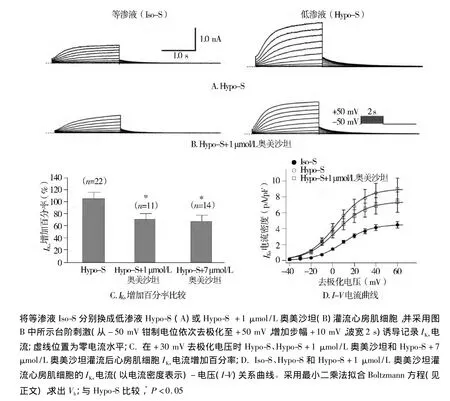
圖2 奧美沙坦減弱Hypo-S誘導豚鼠心房肌細胞I Ks電流增強Figure 2 Olmesartan attenuated the increase of I Ks induced by Hypo-S

表1 奧美沙坦在不同復極化電位下對I Ks通道去活化時間常數(τ)的影響 (ms)Table 1 Effect of olmesartan on the I Ks channel deactivation time constant(τ)in guinea-pig atrial myocytes perfused with hypotonic solution (ms)
3 討論
心肌細胞電生理研究表明,房顫對離子通道最主要的影響是 ICa,L向內電流顯著減少[11],導致心房收縮功能障礙,引發細胞膜牽張和外向IKs電流增加[16,18,19]。ICa,L和 IKs通道電流變化引起心房肌細胞APD縮短,心房生理性節律紊亂,進而促進心房發生電生理和組織結構重構,這些均是持久性房顫的形成基礎[11,20]。Hypo-S引發的心房細胞擴張擬似房顫早期通常發生的心肌細胞膜牽張[11,21],以及所涉及到的各種離子通道轉運變化,包括心房肌細胞IKs增強[16,20,22]。
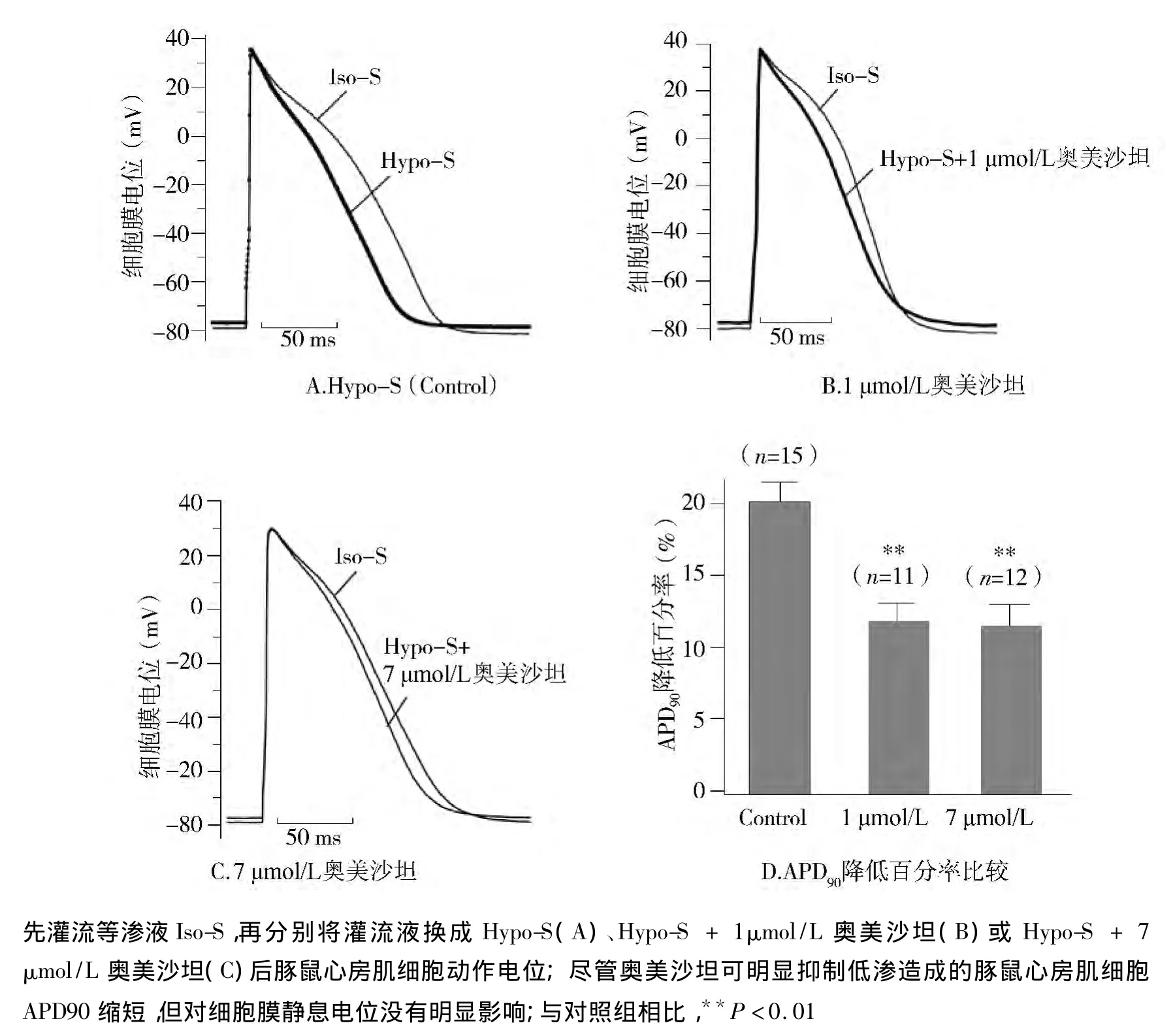
圖3 奧美沙坦降低低滲液Hypo-S誘導的豚鼠心房肌細胞APD90縮短Figure 3 Olmesartan attenuated the shortening of APD90 induced by Hypo-S
本研究發現奧美沙坦可抑制牽張豚鼠心房肌細胞誘導的IKs增強,提示該藥物具有改善房顫作用。近期臨床研究發現[23,24],引發家族性房顫的 KCNQ1基因(編碼IKs通道的α-亞基)變異S140G和R14C可使IKs電流增強,這些研究結果為我們的實驗推測提供了臨床支持。心房細胞膜牽張導致IKs電流增強,心房肌細胞APD縮短,繼而引發房顫并使其得以長期維持[16,25-27]。奧美沙坦可抑制豚鼠心房肌細胞膜受牽張后引發的APD縮短。提示奧美沙坦治療房顫的機制與其抑制心房肌細胞膜受牽張后引發的APD縮短有關。
RAS在房顫的發生和維持過程中起著極為關鍵的作用。房顫發生時心房牽張不僅激活AT1R[27,28],而且會引起心肌細胞分泌血管緊張素Ⅱ[13,14]。Madrid 等[29]報道,與單獨使用胺碘酮相比,AT1受體阻滯劑厄貝沙坦與胺碘酮聯用能夠更有效地防止房顫的復發。雖然存在爭議[30],但一系列近期臨床報道[5-9]和動物實驗均證實了AT1R阻滯劑對房顫的治療作用[1,22]。在本實驗中,奧美沙坦抑制牽張豚鼠心房肌細胞引發的IKs增加,但不影響基礎IKs電流,表明該藥所引起心肌細胞電生理變化與阻斷AT1受體有關。這與Von Lewinski等研究結果相近[31],他們發現厄貝沙坦通過阻斷人心房肌AT1受體可防治血管緊張素Ⅱ誘導的心律失常。有研究報道[15,16],選擇性 AT1R 阻滯劑纈沙坦(valsartan)和坎地沙坦(candesartan)通過激活豚鼠心房肌細胞AT1受體分別抑制AngⅡ和牽張豚鼠心房肌細胞誘發的IKs增強和APD縮短。結合本實驗對奧美沙坦的觀察結果,我們認為,ARB類藥物可改善心房擴張所產生的細胞電生理變化,其機制涉及對AT1受體的阻滯,有利于阻止房顫時發生的急性電生理重構。以往有關ARB類藥物與房顫的關系研究,主要關注的是藥物對心臟組織結構再建的影響[2,4,6],本實驗研究表明在 ARB 類藥物的作用下,心臟電生理再建也會發生。提示,ARB類藥物治療房顫的機制不但涉及心臟組織再建,對心臟電生理再建也具有重要影響。
本實驗還觀察到,Hypo-S可使豚鼠心房肌細胞膜靜息電位上移。但與坎地沙坦一樣[16],奧美沙坦并不影響心房牽張引起的細胞膜靜息電位變化(見圖3)。由于心房肌細胞膜靜息電位的形成主要與內向整流電流 IK1關系密切[20],提示 IK1通道不是AT1受體阻滯劑治療房顫的作用靶點[31]。
[1]Nagayama T,Hirooka Y,Kishi Y,et al.Blockade of brain angiotensinⅡtype I receptor inhibits the development of atrial fibrillation in hypertensive rats[J].Am J Hypertens,2015,28(4):444-451.
[2]Fujita M,Cheng XW,Inden Y,et al.Mechanisms with clinical implications for atrial fibrillation-adssociated remodeling:cathepsin K expression,regulation,and therapeutic target and biomarker[J].J Am Heart Assoc,2013,2(6):e000503.
[3]Ehrlich JR,Nattel S.Novel approaches for pharmacological management of atrial fibrillation[J].Drugs,2009,69(7):757-774.
[4]Spinarova L,Spinar J.Pharmacotherapy of dilated cardiomyopathy[J].Curr Pharm Des,2014,21(4):449-458.
[5]Madrid AH,Peng J,Zamora J,et al.The role of angiotensin receptor blockers and/or angiotensin converting enzyme inhibitors in the prevention of atrial fibrillation in patients with cardiovascular diseases:meta-analysis of randomized controlled clinical trials[J].Pacing Clin Electrophysiol,2004,27(10):1405-1410.
[6]Kiryu M,Niwano S,Niwano H,et al.Angiotensin II-mediated upregulation of connective tissue growth factor promotes atrial tissue fibrosis in the canine atrial fibrillation model[J].Europace,2012,14(8):1206-1214.
[7]Healey JS,Baranchuk A,Crystal E,et al.Prevention of atrial fibrillation with angiotensin-converting enzyme inhibitors and angiotensin receptor blockers:a meta-analysis[J].J Am Coll Cardiol,2005,45(11):1832-1839.
[8]Novo G,Guttilla D,Fazio G,et al.The role of the renin-angiotensin systemin atrial fibrillation and the therapeutic effects of ACEIs and ARBS[J].Br J Clin Pharmacol,2008,66(3):345-351.
[9]Schneider MP,Hua TA,Bohm M,et al.Prevention of atrial fibrillation by rennin-angiotensin systeminhibition a meta-analysis[J].J Am Coll Cardiol,2010,55(21):2299-2307.
[10]Goette A,Schon N,Kirchhof P,et al.Angiotensin II-antagonist in paroxysmal atrial fibrillation(ANTIPAF)trial[J].Circ Arrhythm Electrophysiol,2012,5(1):43-51.
[11]Allessie M,Ausma J,Schotten U.Electrical,contractile and structural remodelling during atrial fibrillation[J].Cardiovasc Res,2002,54(2):230-246.
[12]Nattel S.New ideas about atrial fibrillation 50 years on[J].Nature,2002,415(6868):219-226.
[13]Sadoshima J,Xu Y,Slayter HS,et al.Autocrine release of angiotensinⅡmediates stretch-induced hypertrophy of cardiac myocytes in vitro[J].Cell,1993,75(5):977-984.
[14]Gassanov N,Brandt MC,Michels G,et al.Angiotensin II-induced changes of calcium sparks and ionic currents in human atrial myocytes:potential role for early remodeling in atrial fibrillation[J].Cell Calcium,2006,39(2):175-186.
[15]Zankov DP,Omatsu-Kanbe M,Isono T,et al.Angiotensin II potentiates IKspotassium current via AT1receptors in guinea-pig atrial myocytes[J].Circulation,2006,113(10):1278-1286.
[16]Zankov DP,Toyoda F,Omatsu-Kanbe M,et al.Angiotensin II type 1 receptor mediates partially hyposmotic-induced increase of IKscurrent in guinea pig atrium[J].Pflugers Arch,2009,458(5):837-849.
[17]Moreno I,Caballero R,Gonzalez T,et al.Effects of irbesartan on cloned potassium channels involved in human cardiac repolarization[J].J Pharmacol Exp Ther,2003,304(2):862-873.
[18]Kocic I.Modulators of ion channels activated by hypotonic swelling in cardiomyocytes:new perspectives for pharmacological treatment of life-threatening arrhythmias[J].Curr Med Chem Cardiovasc Hematol Agents,2005,3(4):333-339.
[19]GISSI-AF Investigators,Disertori M,Latini R,et al.Valsartan for prevention of recurrent atrial fibrillation[J].N Engl J Med,2009,360(16):1606-1617.
[20]Schotten U,Verheule S,Kirchhof P,et al.Pathophysiological mechanisms of atrial fibrillation:a translational appraisal[J].Physiol Rev,2011,91(1):265-325.
[21]Sasaki N,Mitsuiye T,Wang Z,et al.Increase of the delayed rectifier K+and Na+-K+pump currents by hypotonic solutions in guinea pig cardiac myocytes[J].Circ Res,1994,75(5):887-895.
[22]Xue XD,Huang JH,Wang HS.Angiotensin II activates signal transducers and activators of transcription 3 via rac1 in the atrial tissue in permanent atrial fibrillation patients with rheumatic heart disease[J].Cell Biochem Biophys,2015,71(1):205-213.
[23]Otway R,Vandenberg JI,Guo G,et al.Stretch-sensitive KCNQ1 mutation:A link between genetic and environmental factors in the pathogenesis of atrial fibrillation[J].J Am Coll Cardiol,2007,49(5):578-586.
[24]Chen YH,Xu SJ,Bendahhou S,et al.KCNQ1 gain-of-function mutation in familial atrial fibrillation[J].Science,2003,299(5604):251-254.
[25]Vandenberg JI,Bett GCL,Powell T.Contribution of a swelling-activated chloride current to changes in the cardiac action potential[J].Am J Physiol,1997,273(2 Pt 1):C541-C547.
[26]Kocic I,Hirano Y,Hiraoka M.Ionic basis for membrane potential changes induced by hypoosmotic stress in guinea-pig ventricular myocytes[J].Cardiovasc Res,2001,51(1):59-70.
[27]Zou Y,Akazawa H,Qin Y,et al.Mechanical stress activates angiotensin II type 1 receptor without the involvement of angiotensinⅡ[J].Nat Cell Biol,2004,6(6):499-506.
[28]Yasuda N,Miura S,Akazawa H,et al.Conformational switch of angiotensinⅡtype 1 receptor underlying mechanical stress-induced activation[J].EMBO Rep,2008,9(2):179-186.
[29]Madrid AH,Bueno MG,Rebollo JM,et al.Use of irbesartan to maintain sinus rhythmin patients with long-lasting persistent atrial fibrillation:a prospective and randomized study[J].Circulation,2002,106(3):331-336.
[30]Von Lewinski D,Kockskamper J,Rubertus SU,et al.Direct proarrhythmogenic effects of angiotensinⅡcan be suppressed by AT1receptor blockade in human atrial myocardium[J].Eur J Heart Fail,2008,10(12):1172-176.
[31]Ehrlich JR.Inward rectifier potassium currents as a target for atrial fibrillation therapy[J].J Cardiovasc Pharmacol,2008,52(2):129-135.