11 096例體檢者幽門螺桿菌感染現狀分析
2016-03-15 12:08:32李萌輝張弛梁曉峰李世霞劉俊田
天津醫藥 2016年1期
關鍵詞:幽門螺桿菌
李萌輝,張弛,梁曉峰,李世霞,劉俊田
?
11 096例體檢者幽門螺桿菌感染現狀分析
李萌輝,張弛,梁曉峰,李世霞,劉俊田△
摘要:目的了解天津地區體檢人群中幽門螺桿菌(Hp)感染的現狀及其分布特征。方法選取2014全年間在我院行Hp檢測的11 096例體檢者為研究對象,應用快速尿素酶法檢測其Hp的感染情況;以體檢者的性別、年齡、職業為依據進行分組分析。結果11 096例體檢者Hp總感染率為30.52%(3 386/11 096),其中男性為34.77% (1 784/5 131),女性為26.86%(1 602/5 965),男性高于女性(P < 0.05);將體檢者按照年齡分為19~29歲、30~39歲、40~49歲、50~59歲、60~69歲和70~92歲組,其Hp感染率分別為19.50%(379/1 944)、25.82%(650/2 517)、31.59%(908/2 874)、37.48%(915/2 441)、41.09%(353/859)和39.18%(181/462),其中50~59歲、60~69歲和70~92歲組>40~49歲組>30~39歲組>19~29歲組(P < 0.003);根據體檢者職業不同進行分組研究,在醫務工作者、工人、教師、工程師、職員、公務員、其他等7個組中Hp感染率分別為25.42%(586/2 305)、29.35%(1 062/3 618)、30.61%(360/1 176)、32.49%(116/357)、33.44%(205/613)、34.52%(455/1 318)和35.23%(602/1 709),醫務工作者Hp感染陽性率25.42(586/2 305)低于工人、教師、職員、公務員和其他人員各組(P<0.002)。結論應加強中老年尤其是男性的Hp診療管理,普及Hp感染預防相關醫學知識,從而更有效地預防Hp感染相關疾病的發生。
關鍵詞:幽門螺桿菌;感染;分布特征;天津
幽門螺桿菌(Hp)是由Marshall和Warren于1983年首次鑒定出來的,因其感染可以導致慢性胃炎、胃潰瘍,甚至胃癌的發生,在過去的30年中受到廣泛關注[1-2]。此外,現有研究還發現Hp感染與潰瘍性結腸炎[3]、牙周病變[4]、酒渣鼻[5]、終末期腎病[6]、2型糖尿病[2]、動脈粥樣硬化[7]、帕金森氏病[8]等多種疾病的發生有關。我國居民Hp的感染率在50%以上,且感染率在不同人群和地區之間有所不同,基本波動在41.35%~72.30%[1]。但目前關于天津地區Hp感染情況及分布特征的研究鮮見報道。鑒于Hp感染對健康帶來的不利影響,以及其在人群中極高感染率的特點,Hp感染檢測作為常規的健康體檢項目是必要的。本研究應用快速尿素酶法對天津地區人群Hp感染現狀和分布特征進行分析,以確定Hp感染重點人群,為流行病學研究及Hp感染相關疾病的預防提供參考。
1 對象與方法
1.1研究對象選取2014年1月—12月在我院行Hp感染檢測的體檢者11 096例,年齡19~92歲,中位年齡44歲。
1.2方法和試劑采用北京康美天鴻生物科技有限公司生產的幽門螺桿菌尿素酶抗體檢測試劑盒(膠體金法)的體外診斷試劑盒進行檢測。嚴格按照無菌操作原則抽取靜脈血2mL,將全血加入無抗凝劑的無菌試管中,經1 000 r/min離心5min后取血清室溫備用。待試劑盒平衡至室溫后,在測試板樣品孔中加入100 μL樣本血清,20min內觀察結果,此過程2h內完成。比較不同性別、年齡組及職業人群Hp感染的陽性率。
1.3結果判定嚴格按照試劑盒說明書進行判定,對照線和測試線均為紅色線判定為陽性;對照線為紅色線,測試線未出現為陰性;對照線未出現,判定為無效。
1.4統計學方法采用SPSS 18.0軟件進行統計分析。計數資料采用χ2檢驗,以P<0.05或P<(0.05/n)為差異有統計學意義。
2 結果
2.1Hp感染與性別的關系11 096例體檢者的Hp總感染率為30.52%(3 386/11 096),其中男性為34.77%(1 784/5 131),女性為26.86%(1 602/5 965),男性高于女性(χ2=81.443,P<0.001)。
2.2Hp感染與年齡的關系將11 096例體檢者分為19~29歲、30~39歲、40~49歲、50~59歲、60~69歲和70~92歲6個組,上述6個年齡組的Hp感染率分別為19.50%(379/1 944)、25.82%(650/2 517)、31.59%(908/2 874)、37.48%(915/2 441)、41.09%(353/859)和39.18%(181/462);其中50~59歲、60~69歲和70~92歲組>40~49歲組>30~ 39歲組>19~29歲組(P < 0.003),而50~59歲、60~69歲和70~92歲3組間差異無統計學意義,見圖1。

Fig.1 H.pylori infection distribution in different age groups圖1 Hp在不同年齡組健康體檢者中感染情況分析
2.3Hp感染在不同職業人群中的分布根據體檢者職業不同進行分組研究,將其分為醫務工作者、工人、教師、工程師、公司職員、公務員、其他等7個組,其Hp感染陽性率分別為25.42%(586/2 305)、29.35%(1062/3 618)、30.61%(360/1 176)、32.49% (116/357)、33.44%(205/613)、34.52%(455/1 318)和35.23%(602/1 709),其他、公務員、公司職員、教師和工人>醫務工作者,其他和公務員>工人,其他、公務員>工人>醫務工作者(P < 0.002),而其余各組間差異無統計學意義,見圖2。
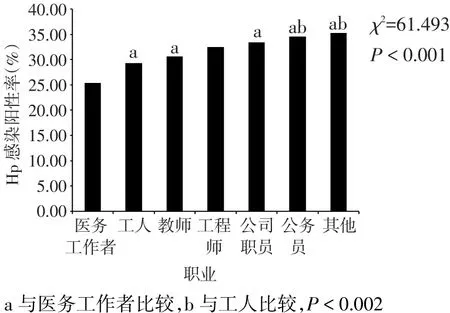
Fig.2 H.pylori infection distribution in different occupational groups圖2 Hp不同職業健康體檢者中感染情況分析
3 討論
Hp感染很常見,是導致胃炎、消化性潰瘍、胃黏膜相關淋巴組織淋巴瘤、胃癌、糖尿病和心血管疾病等多種疾病的致病因素,Hp感染不但對人類健康造成危害,同時也帶來了巨大的社會經濟成本[2,9-10]。隨著經濟水平的增長和社會進步,國家衛生工作重點已經逐步轉向疾病預防。調查人群Hp感染現狀和主要特征,有助于制定Hp感染控制措施,預防Hp感染相關疾病的發生發展。
Hp感染后導致疾病發生的機制尚不完全清楚。研究表明,Hp是導致胃癌發生的重要原因,治療Hp感染可以降低胃癌的發病率,并可能抑制胃癌癌前病變向胃癌進展的過程,根除Hp感染可能是預防胃癌癌前病變發展的一種有效治療方法[11]。最新研究提示,自噬多態性與中國人群胃癌有關,高致病性Hp菌株可能通過調節宿主細胞自噬參與胃癌的發生[12]。流行病學研究發現Hp慢性感染者罹患2型糖尿病的風險增加了,Hp感染患者和實驗小鼠的空腹血糖水平提高了,Hp感染的糖尿病小鼠模型表現為糖代謝受損、胰島素抵抗和超高胰島素血癥,揭示Hp感染通過下調miR-203、上調胰島素信號抑制因子SOCS3的表達參與早期肝細胞胰島素信號通路損傷的過程[13]。而最新的一項研究卻提出了相反的觀點,其認為Hp感染可以作為保護性因素,抵抗女性發生多發性硬化的風險,并推測生命早期感染Hp對免疫系統的建立是必要的,可以阻止一生中過敏和自身免疫疾病的發生,但Hp對多發性硬化的保護是否僅僅局限于女性還有待進一步研究[14]。
Hp具有極高的感染率,我國居民一半以上感染Hp,但各地區之間感染情況卻不盡相同,可能與年齡、地區、飲食習慣等多種因素相關[15]。目前檢測Hp的方法很多,包括培養法、免疫組織化學染色、快速尿素酶試驗、尿抗體檢測以及最新的便Hp抗原一步法等[16-17]。快速尿素酶法便于操作,更適合大規模人群篩查。本研究應用快速尿素酶法對11 096例體檢者中進行Hp感染現狀分析,結果顯示Hp總感染率為30.52%,男性和女性感染率分別為34.77%和26.86%,男性明顯高于女性,且Hp感染率基本隨年齡增加呈增加趨勢,與現有研究結果一致[15]。但50歲以上各年齡組間Hp感染分布無明顯差異,Hp感染率基本在40%左右,趨于穩定水平。以上結果提示,天津地區居民Hp感染率明顯低于全國平均水平[1],性別與年齡可能是影響Hp感染的2個重要因素,且50歲以上居民是Hp感染相關疾病預防的重點人群。
預防Hp感染的傳播也是疾病防治工作的重點內容。在發展中國家,家族內部成員之間,尤其是母嬰、兄弟姐妹之間是Hp感染傳播的主要途徑。其次,夫妻之間也是Hp感染傳播的主要途徑[18]。一直以來,大家都認為Hp感染與缺乏恰當的凈水和保證水衛生的方法有關,但是沒有研究證實Hp污染的水源是導致Hp感染的原因。最新的研究發現,Hp在水中是具有感染性的,提示人類飲用Hp污染的水存在感染Hp的風險[19]。但還需要大量的研究工作進行論證。本研究發現醫務工作者Hp感染率僅為25.42%,低于從事其他職業者,表明Hp相關醫學知識的普及在Hp感染預防中起著重要作用,工人Hp感染率較公務員低,推測可能與社會活動等因素相關,具體原因尚不清楚。
總之,Hp感染可以導致多種疾病的發生,控制Hp感染及傳播仍是預防疾病發生的重要措施,加強Hp預防感染知識的普及、避免水源污染,可能對預防Hp感染起重要作用。
參考文獻
[1] Xie C, Lu NH.Review: clinicalmanagement ofhelicobacter pylori infection in China[J].Helicobacter, 2015, 20(1):1-10.doi: 10.1111/hel.12178.
[2] Abadi AT.Type 2 diabetes andhelicobacter pylori infection: Start?ing point for the reality[J]?Indian J Endocrinolmetab, 2015, 19(2): 306.doi: 10.4103/2230-8210.149330.
[3] Jin X, Chen YP, Chen SH, et al.Association betweenhelicobacter Pylori infection and ulcerative colitis--a case control study from China[J].Int Jmed Sci, 2013 , 10(11):1479- 84.doi: 10.7150/ijms.6934.
[4] Nisha KJ, Nandakumar K, Shenoy KT, et al.Periodontal disease andhelicobacter pylori infection: a community-based study using serology and rapid urease test[J].J Investig Clin Dent, 2014 Aug 30.doi: 10.1111/jicd.12122.[Epub ahead of print]
[5] Gravina A, Federico A, Ruocco E, et al.Helicobacter pylori infec?tion but not small intestinal bacterial overgrowthmay play a patho?genic role in rosacea[J].United European Gastroenterol J, 2015, 3 (1):17-24.doi: 10.1177/2050640614559262.
[6] Lin SY, Lin CL, Liu JH, et al.Association betweenhelicobacter py?lori infection and the subsequent risk of end-stage renal disease: a nationwide population-based cohort study[J].Int J Clin Pract, 2015, 69(5):604-610.doi: 10.1111/ijcp.12602.
[7] Karbasi-Afshar R, Khedmath, Izadim.Helicobacter pylori Infec?tion and atherosclerosis: a systematic review[J].Actamedica Irani?ca, 2015, 53(2):78-88.
[8] Tan AH,mahadeva S,marras C, et al.Helicobacter pylori infection is associated with worse severity of Parkinson′s disease[J].Parkin?sonism Relat Disord, 2015, 21(3):221-215.doi: 10.1016/j.parkrel?dis.2014.12.009.
[9] Lai CY, Yang TY, Lin CL, et al.Helicobacter pylori infection and the risk of acute coronary syndrome: a nationwide retrospective co?hort study[J].Eur J Clinmicrobiol Infect Dis, 2015, 34(1):69-74.doi: 10.1007/s10096-014-2207-7.
[10]milanim, Sharifi Y, Rahmati-Yamchim, et al.Immunology and vaccines and nanovaccines forhelicobacter pylori infection[J].Ex?pert Rev Vaccines, 2015, 14(6):833-840.doi: 10.1586/14760584.2015.1008460.
[11]mansour-Ghanaei F, Joukar F,mojtahedi K, et al.Does treatment ofhelicobacter pylori infection reduce gastric precancerous lesions [J]?Asian Pac J Cancer Prev, 2015, 16(4):1571-1574.
[12] Casta?o-Rodríguez N, Kaakoush NO, Goh KL, et al.Autophagy inhelicobacter pylori infection and related gastric cancer[J].Helico?bacter, 2015.doi: 10.1111/hel.12211.[Epub ahead of print]
[13] Zhou X, Liu W, Gum, et al.Helicobacter pylori infection causeshe?patic insulin resistance by the c- Jun/miR- 203/SOCS3 signaling pathway[J].J Gastroenterol, 2015.[Epub ahead of print]
[14] PedrinimJ, Seewann A, Bennett KA, et al.Helicobacter pylori in?fection as a protective factor againstmultiple sclerosis risk in fe?males[J].J Neurol Neurosurg Psychiatry, 2015, 86(6):603-607.doi: 10.1136/jnnp-2014-309495.
[15] Zhangm, Zhou YZ, Li XY, et al.Seroepidemiology ofhelicobacter pylori infection in elderly people in the Beijing region, China[J].World J Gastroentero, 2014, 20(13):3635-3639.doi: 10.3748/wjg.v20.i13.3635.
[16]miftahussururm, Shiota S, Suzuki R, et al.Identification ofhelico?bacter pylori infection in symptomatic patients in Surabaya, Indone?sia, using five diagnostic tests[J].Epidemiol Infect, 2015, 143(5): 986-996.doi: 10.1017/S095026881400154X.
[17] Lee YC, Tseng PH, Liou JM, et al.Performance of a one-step fecal sample-based test for diagnosis ofhelicobacter pylori infection in primary care andmass screening settings[J].J Formosmed Assoc, 2014, 113(12):899-907.doi: 10.1016/j.jfma.2012.05.014.
[18] Yokota SI, Konnom, Fujiwara SI, et al.Intrafamilial, preferentiallymother-to-child and intraspousal,helicobacter pylori infection in japan determined bymutilocus sequence typing and random ampli?fied polymorphic DNA fingerprinting[J].Helicobacter, 2015.doi: 10.1111/hel.12217.[Epub ahead of print]
[19] Boehnke KF, Eaton KA, Valdiviesom, et al.Animalmodel reveals potential waterborne transmission ofhelicobacter pylori infection[J].Helicobacter, 2015.doi: 10.1111/hel.12216.[Epub ahead of print]
(2015-06-24收稿2015-7-25修回)
(本文編輯閆娟)
讀者·作者·編者
Pylori infection distribution in 11 096 individuals
LImenghui, ZHANG Chi, LIANG Xiaofeng, LI Shixia, LIU Juntian△
Cancer Prevent Department Center of Tianjinmedical University Cancer Institute andhospital, National Clinical Research Center for Cancer, Tianjin Key Laboratory of Cancer Prevention and Therapy, Tianjin 300060,China
△Corresponding Author E-mail:ljt641024@163.com
Abstract:Objective To investigate the distribution ofhelicobacter pylori (Hp) infections among general population in Tianjin.MethodsIndividuals (n=11 096) who visited ourhospital formedical examination andh.Pylori infection screen were included in the research objects.Rapid ureasemethod was utilized to rapidly detecth.pylori infection among the popultion.Individuals were grouped based on their gender, age and occupations, and then were analyzed.Resultsh.pylori-positive rate was 30.52% (3 386/11 096) in 11 096 individuals, in which there were 34.77% (1 784/5 131)male and 26.86% (1 602/5 965) female respectively.Individuals were divided into 5 groups according to their ages: 19 to 29 years old group, 30 to 39 years old group, 40 to 49 years old group, 50 to 59 years old group, 60 to 69 years old group and 70 to 92 years old group.The positive rates ofh.pylori increased with age: 19.50% ( 379/1 944 ) in 19-29 years old group, 25.82% (650/2 517 ) in 30-39 years old group, 31.59% ( 908/2 874 ) in 40-49 years old group, 37.48% (915/2 441 ) in 50-59 years old group, 41.09% ( 353/859 ) in 60-69 years old group and 39.18% (181/462) in 70-92 years old group.The differences in positive rates between different age groups were all of statistically significant (P < 0.05).Individuals were also divided into seven groups according to their occupations:medical worker group, worker group, teacher group, engineer group, clerk group, civil worker group and other career group.The positive rates ofh.pylori infection were 25.42%(586/2 305), 29.35% (1 062/3 618), 30.61%(360/1 176), 32.49%(116/357), 33.44%(205/613), 34.52%(455/1 318)and 35.23%(602/1 709)respectively.The positive rate was 25.42% (586/2 305)medical workers, which was lower than that of other occupation groups with significant difference (P < 0.002).ConclusionGoodmanagement ofh.pylori diagnosis and treatment inmid?dle age and elderly together with popularizing knowledge ofh.pylori prevention can effectively reduceh.pylori incidence.
Key words:helicobacter pylori;infection;distribution characteristics;Tianjin
通訊作者△E-mail:ljt641024@163.com
作者簡介:李萌輝(1982),女,住院醫師,碩士,主要從事腫瘤預防及發病機制研究
中圖分類號:R183.9
文獻標志碼:A
DOI:10.11958/59136
作者單位:天津醫科大學腫瘤醫院預防醫學中心,國家腫瘤臨床醫學研究中心,天津市腫瘤防治重點實驗室(郵編300060)
猜你喜歡
中國實用醫藥(2016年23期)2016-12-26 14:14:06
中國實用醫藥(2016年29期)2016-12-26 14:02:38
中國現代醫生(2016年27期)2016-12-21 16:50:04
家庭用藥(2016年9期)2016-12-03 08:34:20
中國現代醫生(2016年25期)2016-11-19 10:39:01
中國實用醫藥(2016年25期)2016-11-03 11:46:49
中國實用醫藥(2016年21期)2016-08-19 13:50:12
中國實用醫藥(2016年21期)2016-08-19 13:41:57
中國實用醫藥(2016年9期)2016-05-17 11:54:14
中國實用醫藥(2016年8期)2016-03-30 00:44:43