t-PSA和f/t-PSA對前列腺癌的診斷意義及其與Gleason評分的相關性分析
2016-09-05 09:01:16李亞朋曹鳳宏李曉強華北理工大學附屬醫(yī)院泌尿外科河北唐山063000
現(xiàn)代醫(yī)藥衛(wèi)生 2016年4期
李亞朋,曹鳳宏,李曉強(華北理工大學附屬醫(yī)院泌尿外科,河北唐山063000)
t-PSA和f/t-PSA對前列腺癌的診斷意義及其與Gleason評分的相關性分析
李亞朋,曹鳳宏,李曉強△
(華北理工大學附屬醫(yī)院泌尿外科,河北唐山063000)
目的探討血清總前列腺特異性抗原(t-PSA)、游離前列腺特異性抗原/總前列腺特異性抗原(f/t-PSA)在前列腺癌和前列腺增生中的診斷意義及其與前列腺癌Gleason評分的關系。方法采用回顧性分析方法,按照一定的入組標準,收集2007~2014年在該院行前列腺增生(110例)和前列腺癌(75例)手術治療的患者,查閱詳細的病歷資料,對兩組患者入院時t-PSA及f/t-PSA水平、Gleason評分等相關資料進行對比分析。結(jié)果兩組血清t-PSA、f/t-PSA水平比較,差異均有統(tǒng)計學意義(P<0.01),血清t-PSA與Gleason評分呈正相關(rs=0.247,P<0.05),f/t-PSA值與Gleason評分呈負相關(rs=-0.298,P<0.05)。結(jié)論血清t-PSA、f/t-PSA水平在前列腺癌早期診斷中有重要臨床意義,且與Gleason評分有關。
前列腺腫瘤;前列腺增生;前列腺特異抗原/診斷;Gleason評分
前列腺癌在美國占男性惡性腫瘤的27%[1]。前列腺癌的流行病學分布有明顯的地域及人種差異。近年來,前列腺癌在我國的發(fā)病情況也不容樂觀,1994~2002年其發(fā)病率每年增長率約13.4%[1]。隨著我國人口老齡化及人們生活方式的改變,國內(nèi)前列腺癌發(fā)病率也呈增長趨勢[2]。前列腺癌在男性泌尿系統(tǒng)腫瘤中發(fā)病率已居于第3位,嚴重危害著我國中老年男性的身體健康,逐漸成為泌尿外科系統(tǒng)的一項重要研究方向[3]。血清總前列腺特異性抗原(t-PSA)作為臨床上前列腺癌篩查的一個常用指標,具有相對較高的靈敏性和特異性。臨床工作中,前列腺癌患者的Gleason評分高低往往與患者血清t-PSA有關,但目前在t-PSA、游離前列腺特異性抗原/總前列腺特異性抗原(f/t-PSA)與Gleason評分關系方面的文獻報道較少。本研究根據(jù)本院泌尿外科收治的前列腺癌與前列腺增生(BPH)患者的相關病歷資料及術后病理結(jié)果進行對比分析,現(xiàn)報道如下。
1 資料與方法
1.1一般資料選擇2007~2014年本院收治的前列腺癌和BPH患者,按照以下入組條件進行病例篩選:患者入院時不伴前列腺局部炎癥、術后病理結(jié)果可靠、術前未行內(nèi)分泌等方面的治療且均為首次行手術治療。前列腺癌組患者75例,年齡51~92歲,平均(73.49±8.66)歲;BPH組患者110例,年齡55~90歲,平均(71.38±8.95)歲。在病案科查閱所有前列腺癌和BPH患者臨床資料并加以總結(jié)分析,編制成數(shù)據(jù)集合。
1.2t-PSA、f/t-PSA值及Gleason評分的測定t-PSA、f/t-PSA測定:測t-PSA前14 d應避免尿道檢查、直腸指檢、前列腺按摩或者穿刺,對留置導尿管者暫不予測定。檢查當天早晨空腹采靜脈血2 mL,采用放射免疫法測f-PSA和t-PSA,計算二者比值。Gleason評分標準采用經(jīng)過2005年國際泌尿病理學協(xié)會(ISUP)修改后的Gleason分級標準[4]。依據(jù)Gleason評分將前列腺癌分成三組,高分化癌組(2~<5分)10例,中分化癌組(5~<8分)31例和低分化癌組(8~10分)34例。
1.3統(tǒng)計學處理應用SPSS17.0統(tǒng)計軟件進行數(shù)據(jù)分析,計量資料以±s表示,組間比較采用t檢驗;計數(shù)資料以率或構成比表示,采用χ2檢驗;對t-PSA、f/t-PSA 與Gleason評分關系采用Spearman等級相關性分析。P<0.05為差異有統(tǒng)計學意義。
2 結(jié) 果
2.1兩組t-PSA、f/t-PSA水平比較兩組t-PSA及f/t-PSA水平比較,差異均有統(tǒng)計學意義(P<0.01)。見表1。
表1 兩組t-PSA、f-PSA水平及f/t-PSA比較(±s)
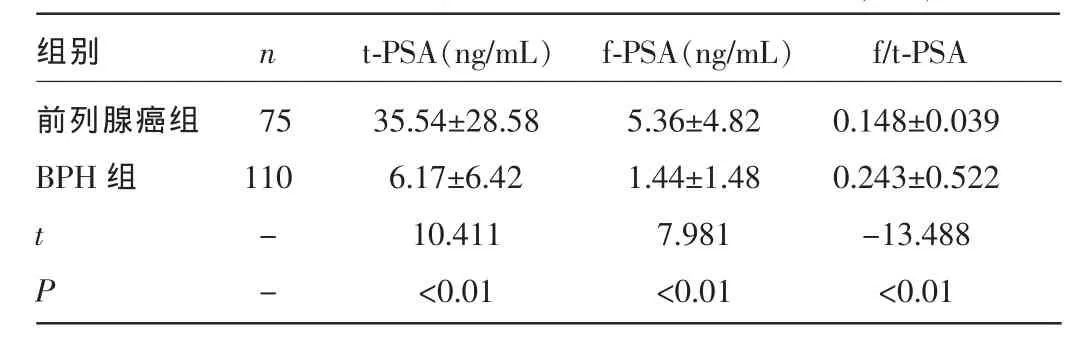
表1 兩組t-PSA、f-PSA水平及f/t-PSA比較(±s)
注:-表示無此項。
組別前列腺癌組B P H 組n t -P S A (n g / m L) f -P S A (n g / m L) f / t -P S A 7 5 1 1 0 t P --3 5 . 5 4 ± 2 8 . 5 8 6 . 1 7 ± 6 . 4 2 1 0 . 4 1 1 <0 . 0 1 5 . 3 6 ± 4 . 8 2 1 . 4 4 ± 1 . 4 8 7 . 9 8 1 <0 . 0 1 0 . 1 4 8 ± 0 . 0 3 9 0 . 2 4 3 ± 0 . 5 2 2 -1 3 . 4 8 8 <0 . 0 1
2.2兩組患者t-PSA水平在不同區(qū)段比較兩組t-PSA<4 ng/mL、4 ng/mL≤t-PSA<10 ng/mL和 t-PSA≥10 ng/mL患者占比比較,差異均有統(tǒng)計學意義(P<0.01)。見表2。

表2 兩組患者t-PSA值在不同區(qū)段比較[n(%)]
2.3前列腺癌組中t-PSA及f/t-PSA與Gleason評分相關性75例前列腺癌患者中,各分化組t-PSA≥4 ng/mL患者占比比較,差異無統(tǒng)計學意義(P>0.05)。Spearman等級相關性分析顯示,t-PSA與Gleason評分呈正相關(rs=0.247,P<0.05)。Spearman等級相關性分析顯示,f/t-PSA 與Gleason評分呈負相關(rs=-0.298,P<0.05)。見表3、4。

表3 75例前列腺癌患者血清t-PSA水平與Gleason評分關系(n)

表4 75例前列腺癌患者血清f/t-PSA與Gleason評分關系(n)
3 討 論
在當前臨床工作中,PSA測定仍然是篩查和診斷前列腺癌的最好指標[5],已被廣泛認可,但實際上PSA并不是前列腺器官及前列腺癌的特異性抗原[6],PSA結(jié)果較易受前列腺體積、炎癥及某些臨床操作如直腸指檢、導尿等因素的影響[7-10],當患者同時伴前列腺炎癥、尿潴留等情況時,血清t-PSA水平會有所升高,因此,t-PSA在前列腺癌的早期診斷方面,尚缺乏足夠的敏感性及特異性,但f-PSA較t-PSA所受的影響相對較小。劉欣等[11]相關研究認為,t-PSA結(jié)合f/t-PSA能夠在兼顧檢測敏感性與特異性的基礎上提高BPH和前列腺癌的鑒別水平,使一部分t-PSA水平增高但不是特別明顯的疾病免除了不必要的前列腺穿刺活檢。因此,為了提高前列腺癌早期診斷水平,不同PSA方面的相關指標,如f-PSA、f/t-PSA及PSA等開始應用在臨床診斷中。
t-PSA在4~10 ng/mL時,f/t-PSA值已被證實對前列腺癌的早期診斷具有相當重要的意義,但在預測前列腺癌患者Gleason評分這些方面尚存在著一些爭議[12]。Pannek等[13]在針對某一部分前列腺癌患者的調(diào)查研究中得出了f/t-PSA與Gleason評分及臨床分期有關。因此,f/t-PSA可以與t-PSA、前列腺穿刺活檢等檢查結(jié)合起來用于預測Gleason評分及臨床分期。
本研究結(jié)果顯示,兩組血清t-PSA水平及f/t-PSA值比較,差異均有統(tǒng)計學意義(P<0.01),以上指標的檢測對于二者之間的鑒別、診斷有較大的臨床意義。當t-PSA水平在不同區(qū)段時,與前列腺癌組比較,差異均有統(tǒng)計學意義(P<0.05)。在前列腺癌組中,各分化組t-PSA≥4 ng/mL患者占比差異不顯著。Spearman等級相關性分析結(jié)果顯示,前列腺癌患者t-PSA與Gleason評分呈正相關(P<0.05),f/t-PSA值與Gleason評分呈負相關(P<0.05)。
綜上所述,t-PSA、f/t-PSA值對于前列腺癌的早期診斷具有很重要的臨床意義,t-PSA、f/t-PSA與Gleason評分之間分別呈正、負相關,該結(jié)果與Grossklaus等[12]的研究結(jié)果基本一致,當t-PSA≥4ng/mL時,f/t-PSA與Gleason評分、臨床分期呈顯著負相關。但是,t-PSA、f/t-PSA值在前列腺癌早期診斷和臨床預后等方面的意義仍需要更加深入的研究。
[1]Shipitsin M,Small C,Choudhury S,et al.Identification of proteomic biomarkers predicting prostate cancer aggressiveness and lethality despite biopsy-sampling error[J].Br J Cancer,2014,111(6):1201-1212.
[2]韓蘇軍,張思維,陳萬青,等.中國前列腺癌發(fā)病現(xiàn)狀和流行趨勢分析[J].臨床腫瘤學雜志,2013,18(4):330-334.
[3]孫穎浩.我國前列腺癌的研究現(xiàn)狀[J].中華泌尿外科雜志,2004,25 (2):77-80.
[4]Epstein JI,Allsbrook WC Jr,Amin MB,et al.The 2005 International Society of Urological Pathology(ISUP)consensus conference on Gleason grading of prostatic carcinoma[J].Am J Surg Pathol,2005,29(9):1228-1242.
[5]Hayes JH,Barry MJ.Screening for prostate cancer with the prostate-specific antigen test:a review of current evidence[J].JAMA,2014,311(11):1143-1149.
[6] Oesterling JE,Jacobsen SJ,Klee GG,et al.Free,complexed and total serum prostate specific antigen:the establishment ofappropriate reference ranges for their concentrations and ratios[J].J Urol,1995,154(3):1090-1095.
[7]Kim JS,Ryu JG,Kim JW,et al.Prostate-specific antigen fluctuation:what does it mean in diagnosis of prostate cancer?[J].Int Braz J Uro,2015,41(2):258-264.
[8]Pezaro C,Woo HH,Davis ID.Prostate cancer:measuring PSA[J].Intern Med J,2014,44(5):433-440.
[9]Roger K.Optimising the management of early prostate cancer[J].Practitioner,2014,258(1770):15-18.
[10]Walsh PC.Re:Prostate cancer screening in the randomized prostate,lung, colorectal,and ovarian cancer screening yrial:mortality results after 13 years of follow-up[J].J Urol,2012,188(2):429-430
[11]劉欣,唐杰,王知力,等.f-PSA/t-PSA比值在良性前列腺增生和前列腺癌鑒別診斷中的應用[J].臨床泌尿外科雜志,2007,22(2):99-101.
[12]Grossklaus DJ,Shappell SB,Gautam S,et al.Ratio of free-to-total prostate specific antigen correlates with tumor volume in patients with in creased prostate specific antigen[J].J Urol,2001,165(2):455-458.
[13]Pannek J,Rittenhouse HG,Chan DW,et al.The use of percent free prostate specific antigen for staging clinically localized prostate cancer[J].J Urol,1998,159(4):1238-1242.
Significance of t-PSA and f/t-PSA in diagnosis of prostatic cancer and analysis on their correlation with Gleason score
Li Yapeng,Cao Fenghong,Li Xiaoqiang△(Department of Urological Surgery,Affiliated Hospital,North China University of Sciences and Engineering,Tangshan,Hebei 063000,China)
ObjectiveTo investigate the significance of serum total prostate specific antigen(t-PSA)and free prostate specific antigen/total-PSA(f/t-PSA)in the diagnosis of prostatic cancer and prostatic hyperplasia and their correlation with the Gleason score.MethodsThe retrospective analysis method was adopted.The patients with prostatic hyperplasia(110 cases)and prostatic cancer(75 cases)treated by operation were collected in this hospital during 2007-2014 were collected.The detailed medical record data were consulted.The related data of T-PSA and f/t-PSA levels and Gleason scores at admission were performed the contrastive analysis.ResultsThe t-PSA and f/t-PSA values had statisticaldifference between the two groups(P<0.01),serum t-PSA was positively correlated with the Gleason score(rs=0.247,P<0.05),while the f/t-PSA value was negatively correlated with the Gleason score(rs=-0.298,P<0.05).ConclusionThe serum t-PSA and f/t-PSA levels have an important clinical significance for the early diagnosis of prostatic cancer,moreover have a correlation with the Gleason score.
Prostatic neoplasms;Prostatic hyperplasia/analysis;Prostate-specific antigen;Gleason score
10.3969/j.issn.1009-5519.2016.04.005
A
1009-5519(2016)04-0492-02
李亞朋(1987-),在讀碩士研究生,主要從事泌尿系統(tǒng)腫瘤方面的研究。
△,E-mail:lixiaoqiang1962@sina.com。
(2015-11-19)
猜你喜歡
美與時代·美術學刊(2022年3期)2022-04-27 01:18:15
中老年保健(2021年3期)2021-08-22 06:50:04
天津醫(yī)科大學學報(2021年2期)2021-03-29 05:31:08
現(xiàn)代臨床醫(yī)學(2021年1期)2021-01-26 00:56:02
家庭醫(yī)學(下半月)(2020年3期)2020-05-30 12:42:02
家庭醫(yī)學(下半月)(2020年3期)2020-05-30 12:42:00
家庭醫(yī)學(下半月)(2020年3期)2020-05-30 12:42:00
人大建設(2019年12期)2019-05-21 02:55:32
中國生殖健康(2019年7期)2019-01-06 09:27:34
現(xiàn)代檢驗醫(yī)學雜志(2014年4期)2014-02-02 02:44:59