絲線與薇喬線縫合軀干四肢裂傷的臨床研究
2016-12-17 08:14:51林富祥
中國醫藥科學 2016年18期
黃 波 林富祥
1.廣東省惠州市第三人民醫院 廣州醫科大學附屬惠州醫院急診科,廣東惠州 516002;2.廣東省惠州市衛生職業技術學院外科教研室,廣東惠州 516002
絲線與薇喬線縫合軀干四肢裂傷的臨床研究
黃 波1林富祥2▲
1.廣東省惠州市第三人民醫院 廣州醫科大學附屬惠州醫院急診科,廣東惠州 516002;2.廣東省惠州市衛生職業技術學院外科教研室,廣東惠州 516002
目的 比較絲線與薇喬線縫合急診軀干及四肢裂傷的美容效果及并發癥。 方法 這是一項隨機對照試驗,研究對象為2010年1月~2014年6月到我院急診外科就診患者,根據患者就診先后順序隨機編為單雙號,單號進入絲線組,雙號進入薇喬線組。縫合后隨訪14d,隔天換藥,絲線組于第14天均拆線,薇喬線組無需拆線,隨訪期間觀察患者傷口感染及裂開情況,拆線后3個月囑患者返院復診,并由整形科醫生使用100mm視覺模擬評分法對傷口美容效果進行評估。 結果 完成隨訪者中,兩組在性別、年齡、創傷類型及裂口長度上均無差異。絲線組感染發生率較薇喬線組低(2.8% VS 5.3%,P=0.138),絲線組和薇喬線組均無傷口裂開,絲線組的100mm視覺模擬評分得分較薇喬線組稍高(53.2mm VS 52.6mm,P=0.900),統計檢驗表明,兩組的美容效果和并發癥發生率差異無統計學意義。 結論 在縫合急診軀干及四肢裂傷時,薇喬線的美容效果和并發癥發生率無差異,可以替代絲線使用。
可吸收線;不可吸收線;裂傷;美容;并發癥
軀干和四肢裂傷,是急診外科常見的疾病,需急診清創縫合。臨床上用于縫合傷口的縫線包括不可吸收線(如絲線)和可吸收線(如薇喬線,羊腸線),兩者對于裂傷口縫合的美容效果及并發癥發生情況尚無定論,本研究通過隨機對照試驗,探討和比較絲線與薇喬線縫合急診軀干及四肢裂傷的美容效果及并發癥,為臨床合理選擇縫線提供理論依據。
1 資料與方法
1.1一般資料
研究對象選取2010年1月~2014年6月到惠州市第三人民醫院院急診外科就診的軀干和四肢裂傷患者(不包括頭面部裂傷),傷口無明顯污染,對皮完整,可一期縫合的。
1.2方法
研究方案由醫院倫理委員會討論通過。告知患者治療方法,是否接受追蹤隨訪,獲得患者同意后,進行研究。納入的研究對象,根據就診的時間先后順序編碼為單雙號,單號進入絲線組,雙號進入薇喬線組,各納入300例。縫線大小選擇3-0,均選擇單純間斷縫合,傷口隔天換藥,絲線組第14天均拆線,薇喬線組線結自行脫落。見圖1。

圖1 研究流程圖
1.3觀察指標
觀察患者傷口感染及裂開情況,拆線后3個月由整形科醫生(不知道縫線類型)使用100mm視覺模擬評分法(VAS)對美容效果進行評估[1],VAS評分越低說明傷口愈合美容效果越差,評分越高說明傷口愈合美容效果越好。
1.4統計學方法
應用SPSS 17.0統計軟件,計量資料組間比較采用t檢驗,計數資料用χ2檢驗,P<0.05為差異有統計學意義。
2 結果
2.1研究對象一般情況
絲線組300例,完成隨訪與美容評估者有247例,失訪或未完成美容評估者53例。完成隨訪和評估的病例中,男134例,女113例;年齡3~75歲,平均(37.8±15.4)歲。薇喬線組300例,完成隨訪與美容評估者有235例,失訪或未完成美容評估者65例,完成隨訪和評估的病例中,男109例,女126例;年齡4~68歲,平均(39.1±19.2)歲。絲線組和薇喬線組在性別(P=0.084),年齡(P=0.671),裂口長度(P=0.703)等情況的差異無統計學意義(P>0.05),具有可比性。見表1。
2.2研究對象各項觀察指標的結果
在隨訪期間,絲線組和薇喬線組發生傷口感染分別為7例和13例(2.8% VS 5.3%,P=0.138),兩組均無傷口裂開。絲線組和薇喬線組VAS評分分 別 為(53.2±10.6)(43.8~66.5)和(52.6±8.4)(45.6~67.2)(P=0.900),統計學檢驗證實兩組在并發癥及傷口美容效果無明顯差異。見表2。

表1 絲線組及微喬線組完成隨訪的患者的一般情況比較
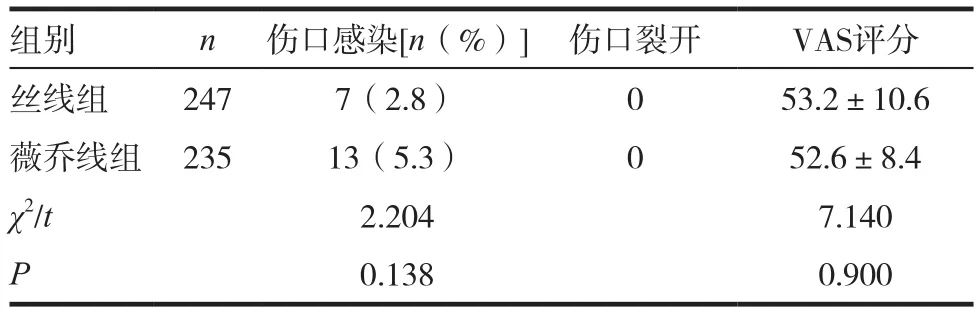
表2 絲線組及微喬線組完成隨訪的患者發生的并發癥及VAS評分比較
3 討論
本研究結果表明,絲線和薇喬線縫合軀干和四肢裂傷的美容效果和并發癥無明顯差異。目前,臨床上醫生主要傾向于使用絲線縫合裂口,理由是絲線比較容易縫合,且較牢固,在傷口愈合前不易開裂,很少引起患者不適感覺,如疼痛等[2-4]。但對于絲線縫合,薇喬線的優點是縫線可自行脫落,不需要拆線,可以明顯減輕患者的不安和焦慮,尤其是兒童患者,減少后續護理[5-8]。本研究證實絲線縫合軀干和四肢,其傷口愈合后美容效果相當,可替代使用。傳統縫合軀干四肢多采用絲線,較少采用微喬線,主要擔心其并發癥的發生,比如傷口感染,比如傷口裂開等,本研究結果顯示,絲線組和微喬線組術后并發癥的發生并無差異,可放心使用,而且微喬線的諸多優點,結合本研究的結果,我們認為薇喬線可以作為外傷性裂傷縫合的良好選擇。但微喬線縫合價格較高,仍是限制其使用的主要原因[6]。有學者認為羊腸線價格便宜,是較好的替代品,且具有可吸收線的一般優點,但由于羊腸線傷口疼痛較薇喬線大,且更容易發生傷口感染[9],本研究暫不予對照,但在后續研究中可能探討。
薇喬線在過去的頭面部裂傷研究中早已探討[10-11],本研究的創新之處在于探討薇喬線在軀干和四肢的縫合,這些部位往往愈合更慢[12-13],使用薇喬線縫合是否增加傷口感染和裂開的機會,尚存爭議。薇喬線在軀體其他部位均顯現出較好的應用價值[14-15],本研究結果可作為這些研究的補充。雖然我們的結果顯示絲線組和薇喬線組之間的差異不大,但與以往的頭面部裂傷研究相比,我們的美容效果評分VAS明顯低得多[10]。究其原因是頭面部愈合時間快,軀干及四肢愈合時間長,且本研究VAS評估時間較短,為拆線后3個月,如果VAS評估時間調整為拆線后6個月或更長時間,本研究的VAS可能較當前的VAS高,這有待繼續隨訪和評價。
雖然我們發現兩個研究組之間的結果差別不大,但這正為我們使用薇喬線縫合軀干及四肢裂傷提供了依據,尤其是應用于小兒患者。我們的結果提示使用薇喬線縫合這些部位的裂傷美容效果與絲線相當,且并不增加感染和裂開的風險。
綜上所述,在縫合軀干及四肢裂傷時,急診科醫生需考慮到可以使用可吸收線薇喬線進行縫合,尤其是兒童患者及焦慮患者。因為薇喬線在美容效果及并發癥發生率上與絲線無明顯差異,而薇喬線具有自行脫落,無需拆線等優點。
[1]Bagabas OA. Assessment of Dental Esthetics by Patients and Dentists Before and After Treatment[D]. Boston:Tufts University School of Dental Medicine, 2015.
[2]Hernandez K A, Hooper R C, Boyko T, et al. Reduction of suture associated inflammation after 28 days using novel biocompatible pseudoprotein poly (ester amide)biomaterials[J]. Journal of Biomedical Materials Research Part B: Applied Biomaterials, 2015, 103(2): 457-463.
[3]Karounis H, Gouin S, Eisman H, et al. A randomized,controlled trial comparing long-term cosmetic outcomes of traumatic pediatric lacerations repaired with absorbable plain gut versus nonabsorbable nylon sutures[J]. Academic Emergency Medicine, 2004, 11(7): 730-735.
[4]Sala-Pérez S, López-Ramírez M, Quinteros-Borgarello M, et al. Antibacterial suture vs silk for the surgical removal of impacted lower third molars. A randomized clinical study[J]. Medicina oral, patología oral y cirugía bucal, 2016, 21(1): e95.
[5]Rettenmaier MA, Abaid LN, Brown JV, et al. Dramatically reduced incidence of vaginal cuff dehiscence in gynecologic patients undergoing endoscopic closure with barbed sutures: A retrospective cohort study[J]. International Journal of Surgery, 2015, 19: 27-30.
[6]Sharma HSH, Kangesu LKL. Vicryl rapide inclusion cysts and suture sinus tracts following hypospadias repair[J]. JPRAS Open, 2015, 3: 13-16.
[7]Mahdy RA, Wagieh MM. Safety and efficacy of fibrin glue versus vicryl sutures in recurrent pterygium with amniotic membrane grafting[J]. Ophthalmic Research, 2012, 47(1): 23-26.
[8]Gartti-Jardim EC, de Souza AP, de Souza Carvalho ACG,et al. Comparative study of the healing process when using Vicryl, Vicryl Rapid, Vicryl Plus, and Monocryl sutures in the rat dermal tissue[J]. Oral and Maxillofacial Surgery,2013, 17(4): 293-298.
[9]Bharathi A, Reddy DBD, Kote GSSAA. A prospective randomized comparative study of vicryl rapide versus chromic catgut for episiotomy repair[J]. Journal of Clinical and Diagnostic Research: JCDR, 2013, 7(2): 326-330.
[10]Luck R P, Flood R, Eyal D, et al. Cosmetic outcomes of absorbable versus nonabsorbable sutures in pediatric facial lacerations[J]. Pediatric Emergency Care, 2008, 24(3): 137-142.
[11]Israr M, Stassen LF. The comparison of scalp closure with staples,silk,prolene and vicryl following a gillies temporal approach for malar/zygomatic complex fracture:a prospective study[J]. Pakistan Oral & Dental Journal, 2013, 33(1):3-5.
[12]DeBoard RH, Rondeau DF, Kang CS, et al. Principles of basic wound evaluation and management in the emergency department[J]. Emergency Medicine Clinics of North America, 2007, 25(1): 23-39.
[13]Cagatay HH, Gokce G, Ekinci M, et al. Long-term comparison of fibrin tissue glue and vicryl suture in conjunctival autografting for pterygium surgery[J]. Postgraduate Medicine, 2014, 126(1): 97-103.
[14]Al-Abdullah T, Plint AC, Fergusson D. Absorbable versus nonabsorbable sutures in the management of traumatic lacerations and surgical wounds: a meta-analysis[J]. Pediatric Emergency Care, 2007, 23(5): 339-344.
[15]Mahdy R A, Wagieh M M. Safety and efficacy of fibrin glue versus vicryl sutures in recurrent pterygium with amniotic membrane grafting[J]. Ophthalmic Research,2012, 47(1): 23-26.
Clinical research on stitching laceration of trunk limbs with silk thread and vicryl
HUANG Bo1LIN Fuxiang2
1. Department of Emergency, the Third People's Hospital of Huizhou, Guangzhou Hospital Affiliated to Huizhou Medical University, Guangdong, Huizhou 516002, China; 2. Department of Surgery, Huizhou Career Technical College, Guangdong, Huizhou 516002, China
Objective To compare the cosmetic results and complications of silk thread and vicryl to stitch laceration of trunk limbs. Methods This was a randomized controlled trial. The patients cured in the department of surgery of our hospital from January 2010 to June 2014 were selected as the objects. According to the order of visiting, patients were randomly assigned to odd numbers and even numbers. Patients of odd numbers were silk group, and patients of even numbers were vicryl group. The patients were followed up for 14 days with next day dressing. Patients in silk group took out stitches on the fourteenth day. Patients in vicryl group were no stitches. Wound infection and rupture in patients should be observed during the follow-up period. Patients were asked to return to the hospital to visit 3 months after stitches. The cosmetic effect was evaluated by the plastic surgeon using the 100mm visual analogue scale. Results For patients complete followed up, there were no differences in sex, age, type of trauma and length of the gap between the two groups. Incidence of infection of silk group was less than that of vicryl group (2.8% VS 5.3%, P=0.138). No wound was split in the two groups. The 100mm visual analogue scale score of silk group was higher than that of vicryl group (53.2mm VS 52.6mm, P=0.900). Statistical tests showed that there was no significant difference in the cosmetic results and the incidence of complications between the two groups. Conclusion When the emergency trunk and extremities laceration suture, cosmetic effect and complication incidence of vicryl are no difference, which can replace the use of silk thread.
Absorbable line; Non absorbable line; Laceration; Cosmetic; Complication
R641
B
2095-0616(2016)18-168-03
▲
(2016-03-19)
猜你喜歡
體育科技文獻通報(2022年3期)2022-05-23 13:46:54
中老年保健(2021年12期)2021-11-30 02:58:01
天津外國語大學學報(2021年3期)2021-08-13 08:32:18
遼金歷史與考古(2021年0期)2021-07-29 01:06:54
科技傳播(2019年22期)2020-01-14 03:06:54
民用飛機設計與研究(2019年4期)2019-05-21 07:21:24
攝影之友(影像視覺)(2019年2期)2019-03-05 08:27:14
中華詩詞(2018年11期)2018-03-26 06:41:34
汽車工程學報(2017年2期)2017-07-05 08:13:02
Coco薇(2016年8期)2016-10-09 02:11:50