富血小板血漿聯合透明質酸鈉關節內注射治療膝骨關節炎的前瞻性隨機對照研究
2017-04-14 05:17:57丁權威呂帥潔沈興潮童培建
上海醫藥 2017年5期
丁權威+呂帥潔+沈興潮+童培建
摘 要 目的:評價富血小板血漿(PRP)聯合透明質酸鈉(HA)治療膝骨關節炎(KOA)的臨床療效。方法:選取47例KOA患者分成PRP組和PRP+HA組,采用WOMAC、VAS和Lequesne評分評估它們在治療前后的臨床表現及比較臨床療效差異。結果: PRP組患者隨訪6個月時的有效率為74.1%,而PRP+HA組為80%。2組的WOMAC、VAS和Lequense評分較治療前比較均有統計學差異(P<0.05),且PRP+HA組在3個月療程內的VAS、WOMAC和Lequense評分均優于PRP組(P <0.05)。結論:單純PRP或聯合HA關節內注射治療KOA均有緩解關節疼痛,改善關節功能的作用,而兩者聯合的療效更加明顯。
關鍵詞 富血小板血漿 透明質酸鈉 膝骨關節炎 軟骨
中圖分類號:R684.3 文獻標識碼:B 文章編號:1006-1533(2017)05-0025-04
A prospective randomized controlled study on platelet-rich plasma (PRP) combined with sodium hyaluronate (HA) intra-articular injection in the treatment of knee osteoarthritis*
DING Quanwei1**, LV Shuaijie2, SHEN Xingchao3, TONG Peijian1,2
(1. Zhejiang Chinese Medical University, Hangzhou 310053, China; 2. The First Clinical Medical College of Zhejiang Chinese Medical University, Hangzhou 310053, China; 3. Shaoxing Traditional Chinese Medical Hospital, Shaoxing 312000, China)
ABSTRACT Objective: To evaluate clinical efficacy of platelet-rich plasma (PRP) combined with sodium hyaluronate(HA) in the treatment of knee osteoarthritis (KOA). Methods: Forty-seven cases of patients with KOA were selected and divided into a PRP group and a PRP+HA group and their manifestation in clinic was evaluated before and after treatment and clinical efficacy was compared based on WOMAC, VAS and Lequesne scores. Results: The effective rate was 74.1% in the PRP group and 80% in the PRP+HA group during six months of follow-up. The WOMAC, VAS and Lequense scores of both groups showed significant differences before and after treatment (P<0.05), and the VAS, WOMAC and Lequense scores were better in the PRP+HA group than in the PRP group during 3 months of treatment (P<0.05). Conclusion: PRP or PRP+HA intra-articular injection in the treatment of KOA can relieve joint pain and improve joint function, and furthermore the efficacy of PRP and HA in association is more significant.
KEY WORDS platelet-rich plasma; sodium hyaluronate; knee osteoarthritis; cartilage
膝關節骨關節炎(knee osteoarthritis, KOA)是一種由多因素導致的慢性進行性骨關節病,65歲以上人群的患病率達68%,表現為關節腫痛和功能障礙等,具有患病率高、晚期功能障礙程度高等特點[1]。目前為止并沒有明確的藥物和方法能夠阻止軟骨的退化進程,其治療的首要目的是緩解膝關節疼痛和改善膝關節功能,包括藥物療法、關節內注射和手術等方法[2-3]。透明質酸鈉(sodium hyaluronate , HA)作為一種關節潤滑劑已被廣泛應用于臨床[4],具有潤滑關節、保護軟骨、抑制炎癥和緩解疼痛等作用[5]。此外,富血小板血漿(plateletrich plasma,PRP)療法作為具有修復受損軟骨可能的自體生長因子注射療法正逐漸引起重視。目前,有關PRP與HA聯合使用的研究,未見報道。我院自2014年7月至2014年11月期間,對PRP聯合HA關節內注射治療KOA進行了前瞻性隨機對照研究,報告如下。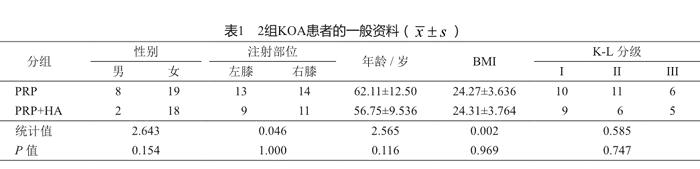
1 資料與方法
1.1 一般資料
本項目是一項臨床前瞻性隨機對照研究,已通過我院醫學倫理委員會倫理審查(2013-X-063),參與本項目的所有患者在治療前均簽署了相關的知情同意書和診療同意書。
病例納入標準:①年齡35至85歲;②符合1995年美國風濕病協會修訂的《膝關節骨關節炎分類標準》[6];③Kellgren-Lawrence(KL)分級I~III級[7];④血小板數量等血液指標正常;⑤患者同意本治療方法,并簽署知情同意書。排除標準:①不符合KOA臨床診斷標準者;②患有糖尿病、血液病等全身性疾病,或局部感染;③血紅蛋白<11 g/L、血小板<1.5×105/L;④治療前5 d內有非甾體類抗炎藥使用史;⑤3個月內有服用抗凝血劑和免疫抑制劑者。
本研究共納入47例,男10例,女37例;KL分級I級19例,II級17例,III級11例;平均年齡59.8歲。通過隨機數字表法,將47例KOA患者分成PRP組和PRP+HA組。2組患者術前資料差異無統計學意義(P>0.05,表1),具有可比性。
1.2 手術方法
1.2.1 術前準備
所有患者術前均攝膝關節正側位X線,并作出KL分級。術前進行膝關節WOMAC、VAS[8]和Lequesne評分[9],以了解患者的生活質量和患膝功能狀況。術前檢查患者血常規+CRP、生化類和凝血功能,以達到治療前要求。
1.2.2 PRP制備
用一次性采血針及采血管,經患者肘前靜脈取全血40 ml,用枸櫞酸鈉抗凝。采用二次離心法:第1次用1 450 r/min離心(離心機型號:TAS10-TLL700A)10 min。用吸管吸取全部上清液至液固交界面下3 mm。將取出的上清液再次離心。第2次3 370 r/min離心10 min。吸取約3/4上清液棄掉,剩余搖勻,即為PRP,共5 ml。取1 ml PRP 行血小板計數。剩余4 ml在2 h內完成注射。注射前在PRP中加入1 ml氯化鈣(上海信誼金朱藥業有限公司)以激活血小板。
1.2.3 注射治療
1)PRP組 患者取仰臥位,伸直患膝。局部消毒,選取髕骨下方的髕韌帶內側或外側關節間隙為進針點,用一次性注射器經皮穿刺入關節腔。如關節腔內有較多積液時可先抽出部分積液。將4 ml PRP注射入膝關節病變部位。1次/周,3次/療程,每個療程間隔1周,共3療程。
2)PRP+HA組 將激活的PRP與HA(25 mg/2.5 ml;Hyalgan, Fidia, Abano Terme, Italy)在一次性注射器內混合后,采用相同體位和方法將6.5 ml混合物注射入膝關節。療程同PRP組。
1.3 術后處理及療效判定
術后局部無菌包扎,并囑患者屈伸膝關節數次,常規口服頭孢地尼分散片0.1 g tid 2 d以防感染。囑患側關節避免劇烈運動,告知患者術后疼痛及腫脹等相關可能性。采用WOMAC、VAS和Lequesne評分標準進行療效判定。隨訪時以WOMAC評分下降至少36%[10]及以上定義為治療有效。
1.4 統計學處理

2 結果
所有患者均獲得至少6個月隨訪。2組患者在治療過程中均未出現膝關節紅腫、發熱等局部感染和其他不適癥狀。隨訪顯示,2組的WOMAC、VAS和Lequense評分較治療前比較均有統計學差異(P1 <0.05,表2),且PRP+HA組在治療開始后的最初3個月,VAS、WOMAC和Lequense評分均優于PRP組,差異有統計學意義(P<0.05,表2)。但是3個月療程結束后隨訪發現,2組在VAS、WOMAC和Lequense評分方面均無統計學差異(P>0.05,表2)。根據WOMAC評分至少下降36%為治療有效計算,PRP組患者隨訪6個月的有效率為74.1%,略低于PRP+HA組的80%。
3 討論
膝關節骨關節炎作為一種慢性進行性的關節疾病,是造成工作能力喪失的第二大主要原因[11],隨之而來的是沉重的經濟與社會負擔[12]。關于KOA 的病因和發病機制等至今尚不十分明確[13],關節軟骨退行性改變是KOA的基本病理變化和病理基礎,同時受累關節滑膜所分泌的滑液成分也發生改變[14]。由于KOA患者關節腔內HA合成受損、自由基降解[15]和積液稀釋[16]等原因,導致內生HA的分子量和濃度下降,引起關節黏彈性降低,關節軟骨抗機械應力的能力下降而關節受損[17]。
作為滑液中最主要的成分,HA是一種由N-乙酰-D-氨基葡萄糖和D-氨基葡萄糖組成的無支鏈的聚陰離子聚合物,在關節內起營養與保護作用[18]。雖然最新的美國KOA診療指南不推薦使用HA[19],但是動物實驗發現,HA在抗炎、抗細胞凋亡、抗血管生成和抗纖維化方面具有重要作用[20]。而大量臨床研究也表明,HA具有緩解關節疼痛和改善關節功能等作用[21-23]。但是有學者認為,HA對于KOA病情嚴重的患者療效不佳[24],而且隨著時間延長,HA的療效呈下降趨勢[25],這在高齡患者中尤為明顯[26],同時HA也無法使受損軟骨再生[27]。
PRP作為大量生長因子的載體[28],具有促進組織修復的功能[29],正越來越多地被應用于KOA的治療。PRP的制備目前多采用二次離心法[30],通過此法我們將血小板濃縮至原始數值的4.6倍。有學者認為,PRP可能使滑膜組織、脂肪墊或者軟骨下骨中的前體細胞遷移、增殖和分化,從而促進受損軟骨的修復[31-32],同時達到減輕疼痛、減少炎癥反應的作用[33]。本研究顯示,PRP組在VAS、WOMAC和Lequesen評分方面均優于治療前(差異有統計學意義),說明PRP確實具有緩解膝部疼痛和改善關節功能的作用。但臨床療效隨著時間的延長呈逐漸下降趨勢。
有研究發現,HA和PRP可以在不改變兩者最初特性的情況下發揮作用[34]。Anitua等[35]通過比較肌腱細胞和滑膜成纖維細胞在單純PRP溶液和PRP+HA溶液中的遷移能力發現,PRP與HA混合后能顯著提高細胞的運動能力。Marmotti等[36]則發現PRP中加入HA能有效促進軟骨細胞的增殖,提高軟骨修復能力。因此,我們將PRP與HA聯合注射治療,3個月隨訪示,聯合組療效優于單純PRP組,這可能與HA協同潤滑關節、改善關節功能有關。隨訪6個月時,雖然2組在VAS、WOMAC和Lequesen評分方面的差異無統計學意義。但是PRP+HA組的評分結果優于PRP組,說明HA作為載體,或許有延緩生長因子釋放、延長PRP作用時間的功效,這仍有待于進一步研究證實。
治療期間,部分患者出現局部腫脹、酸楚感,大多數患者在1 d后癥狀消失,2組患者中均無感染等不良事件發生。本研究屬于臨床短期療效評價,因此沒有進行關節軟骨變化的觀察,而長期療效則需更大樣本量及更長隨訪時間的觀察。此外,PRP與HA混合后的協同作用及機制,仍需我們進一步的深入探討。
參考文獻
[1] Widuchowski W, Widuchowski J, Trzaska T. Articular cartilage defects: study of 25, 124 knee arthroscopies[J]. Knee, 2007, 14(3): 177-182.
[2] Filardo G, Kon E, Buda R, et al. Platelet-rich plasma intraarticular knee injections for the treatment of degenerative cartilage lesions and osteoarthritis[J]. Knee Surg Sports Traumatol Arthrosc, 2011, 19 (4): 528-535.
[3] Kon E, Buda R, Filardo G, et al. Platelet-rich plasma: intraarticular knee injections produced favorable results on degenerative cartilage lesions[J]. Knee Surg Sports Traumatol Arthrosc, 2010, 18(4): 472-479.
[4] Peyron JG, Balazs EA. Preliminary clinical assessment of Na hyaluronate injection into human arthritic joints[J]. Pathol Biol(Paris), 1977, 22(8): 731-736.
[5] 侯德才. 膝關節骨性關節炎的分期治療[J]. 中醫正骨, 2014, 26(1): 3-5.
[6] Hochberg MC, Altman RD, Brandt KD, et al. Guidelines for the medical management of osteoarthritis. Part II. Osteoarthritis of the knee. American College of Rheumatology[J]. Arthritis Rheum, 1995, 38(11): 1541-1546.
[7] Kellgren JH, Lawrence JS. Radiological assessment of osteoarthrosis[J]. Ann Rheum Dis, 1957, 16(4): 494-502.
[8] Bellamy N, Buchanan WW, Goldsmith CH, et al. Validation study of WOMAC: a health status instrument for measuring clinical important patient relevant outcomes to antirheumatic drug therapy in patients with OA of the hip or knee[J]. J Rheumatol, 1988, 15(12): 1833-1840.
[9] Lequesne MG. The algofunctional indices for hip and knee osteoarthritis[J]. J Rheumatol, 1997, 24(4): 779-781.
[10] Goldsmith CH, Boers M, Bombardier C, et al. Criteria for clinically important changes in outcomes; development, scoring and evaluation of rheumatoid arthritis patient and trial profiles. OMERACT Committee[J]. J Rheumatol, 1993, 20(3): 516-527.
[11] Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States Part II[J]. Arthritis Rheum, 2008, 58(1): 26-35.
[12] Stewart WF, Ricci JA, Chee E, et al. Lost productive time and cost due to common pain conditions in the US workforce[J]. JAMA, 2003, 290(18): 2443-2454.
[13] Gobbi A, Lad D, Karnatzikos G. The effects of repeated intra-articular PRP injections on clinical outcomes of early osteoarthritis of the knee[J]. Knee Surg Sports Traumatol Arthrosc, 2015, 23(8): 2170-2177.
[14] Aigner T, Kim HA. Apoptosis and cellular vitality: issues in osteoarthritic cartilage degeneration[J]. Arthritis Rheum, 2002, 46(8): 1986-1996.
[15] Myint P, Deeble DJ, Beaumont PC, et al. The reactivity of various free radicals with hyaluronic acid: steady-state and pulse radiolysis studies[J]. Biochim Biophys Acta, 1987, 925(2): 194-202.
[16] Ono Y, Sakai T, Hiraiwa H, et al. Chondrogenic capacity and alterations in hyaluronan synthesis of cultured human osteoarthritic chondrocytes[J]. Biochem Biophys Res Commun, 2013, 435(4): 733-739.
[17] Campo GM, Avenoso A, DAscola A, et al. 4-mer hyaluronan oligosaccharides stimulate inflammation response in synovial fibroblasts in part via TAK-1 and in part via p38-MAPK[J]. Curr Med Chem, 2013, 20(9): 1162-1172.
[18] Reitinger S, Lepperdinger G. Hyaluronan, a ready choice to fuel regeneration: a mini review[J]. Gerontology, 2013, 59(1): 71-76.
[19] Jevsevar DS, Brown GA, Jones DL, et al. The American Academy of Orthopaedic Surgeons evidence-based guideline on: treatment of osteoarthritis of the knee, 2nd edition[J]. J Bone Joint Surg Am, 2013, 95(20): 1885-1886.
[20] Abate M, Pulcini D, Di Iorio A, et al. Viscosupplementation with intra-articular hyaluronic acid for treatment of osteoarthritis in the elderly[J]. Curr Pharm Des, 2010, 16(6): 631-640.
[21] Hunter DJ, Lo GH. The management of osteoarthritis: an overview and call to appropriate conservative treatment[J]. Rheum Dis Clin North Am, 2008, 34(3): 689-712.
[22] Campbell J, Bellamy N, Gee T. Differences between systematic reviews/meta-analyses of hyaluronic acid/ hyaluronan/hylan in osteoarthritis of the knee[J]. Osteoarthritis Cartilage, 2007, 15(12): 1424-1436.
[23] Miller LE, Block JE. US-approved intra-articular hyaluronic acid injections are safe and effective in patients with knee osteoarthritis: systematic review and meta-analysis of randomized, saline controlled trials[J]. Clin Med Insights Arthritis Musculoskelet Disord, 2013, 6: 57-63.
[24] Dagenais S. Intra-articular hyaluronic acid(viscosupplementation) for knee osteoarthritis[J]. Issues Emerg Health Technol, 2006(94): 1-4.
[25] Bannuru RR, Natov NS, Dasi UR, et al. Therapeutic trajectory following intraarticular hyaluronic acid injection in knee osteoarthritis-meta-analysis[J]. Osteoarthritis Cartilage, 2011, 19(6): 611-619.
[26] U?ar D, D?ra?o?lu D, Süleyman T, et al. Intra-articular hyaluronic Acid as treatment in elderly and middle-aged patients with knee osteoarthritis[J]. Open Rheumatol J, 2013, 7: 38-41.
[27] Andia I, Abate M. Knee osteoarthritis: hyaluronic acid, platelet-rich plasma or both in association? [J]. Expert Opin Biol Ther, 2014, 14(5): 635-649.
[28] Cole BJ, Seroyer ST, Filardo G, et al. Platelet-rich plasma: where are we now and where are we going? [J]. Sports Health, 2010, 2(3): 203-210.
[29] Patel S, Dhillon MS, Aggarwal S, et al. Treatment with platelet-rich plasma is more effective than placebo for knee osteoarthritis: a prospective, double-blind, randomized trial[J]. Am J Sports Med, 2013, 41(2): 356-364.
[30] Karystinou A, DellAccio F, Kurth TB, et al. Distinct mesenchymal progenitor cell subsets in the adult human synovium[J]. Rheumatology (Oxford), 2009, 48(9): 1057-1064.
[31] Manferdini C, Maumus M, Gabusi E, et al. Adipose-derived mesenchymal stem cells exert anti-inflammatory effects on chondrocytes and synoviocytes from osteoarthritis patients through prostaglandin E2[J]. Arthritis Rheum, 2013, 65(5): 1271-1281.
[32] de Vries-van Melle ML, Narcisi R, Kops N, et al. Chondrogenesis of mesenchymal stem cells in an osteochondral environment is mediated by the subchondral bone[J]. Tissue Eng Part A, 2013, 20(1-2): 23-33.
[33] 呂帥潔, 厲駒, 何斌, 等. 富血小板血漿關節內注射治療膝骨關節炎的前瞻性隨機對照研究[J]. 中華創傷雜志, 2016, 32(7): 626-631.
[34] Sundman EA, Cole BJ, Karas V, et al. The anti-inflammatory and matrix restorative mechanisms of platelet-rich plasma in osteoarthritis[J]. Am J Sports Med, 2013, 42(1): 35-41.
[35] Anitua E, Sanchez M, De la Fuente M, et al. Plasma rich in growth factors (PRGF-Endoret) stimulates tendon and synovial fibroblasts migration and improves the biological properties of hyaluronic acid[J]. Knee Surg Sports Traumatol Arthrosc, 2012, 20(9): 1657-1665.
[36] Marmotti A, Bruzzone M, Bonasia DE, et al. One-step osteochondral repair with cartilage fragments in a composite scaffold[J]. Knee Surg Sports Traumatol Arthrosc, 2012, 20(12): 2590-2601.
